

***LISTEN TO THE PODCAST HERE***
Anatomy
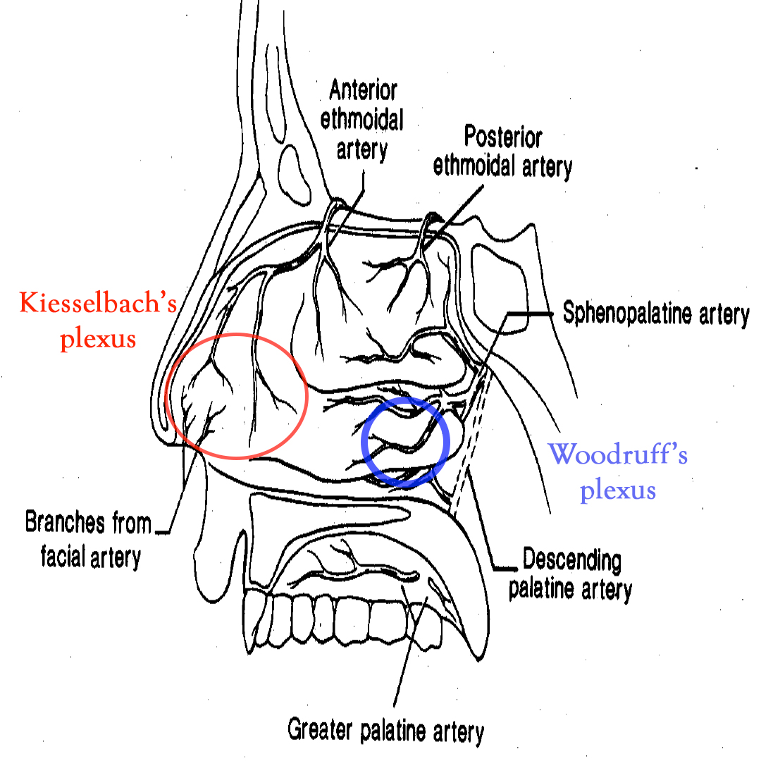
Anterior
- Kiesselbach’s Plexus (Little’s area)
- Confluence of three main vessels
- Septal branch of the anterior ethmoidal artery
- Lateral nasal branch of the sphenopalatine artery
- Septal branch of the superior labial branch of the facial artery
- Confluence of three main vessels
Posterior
- Woodruff’s Plexus
- Posteriorlateral branches of the sphenopalatine artery
- Posterior inferior turbinate
- Posteriorlateral branches of the sphenopalatine artery
Epidemiology
- Up to 60% of population will experience a significant nosebleed each year
- Only 10% need to seek attention
- Common ENT admission condition, but rarely needs surgical intervention
- Bimodal age distribution
- Before 10 years or between 45-65 years
- Male predominance before the age of 49, then equalizes
- Estrogen has been shown to protective for mucosa
- Anterior bleeds are significantly more common (>90%) and resolve with minor interventions
- Posterior bleeds can result in significant hemorrhage
Etiologies
- Nose picking
- Low environmental moisture
- Mucosal hyperemia of viral or allergic rhinitis
- Trauma
- Foreign body
- Anticoagulation
- Coagulopathies
- Osler-Weber-Rendu, von Willebrand, hemophilias
- Connective tissue disease
- Aneurysm development
- Neoplasm
- Squamous cell, inverted papilloma
- Hypertension
- Debated as a cause, but has shown to prolong bleeding
- Nasal medications
- Steroids, oxymetazoline
- Heart failure
Patient Assessment
- Primary
- Airway assessment
- RR, O2
- Cardiovascular stability
- HR, BP
- Airway assessment
- Secondary
- History
- Medications
- Anticoagulation, aspirin, nasal medications
- PMH
- Bleeding disorders, HTN, liver disease
- Recent trauma
- History of nosebleeds
- How often, how long do they last, ever been admitted for one
- Medications
- History
- Diagnostic Studies
- Coagulation studies should NOT be routinely ordered
- Should be in patients on anticoagulation
- In patients with prolonged bleeds:
- CBC
- Type and cross
- Coagulation studies should NOT be routinely ordered
- Examination
- Have patient blow nose to remove clots and blood
- Examine nasal cavity to see if you can see the bleeding site
- Otoscope, nasal speculum
- Don’t have patient tilt head back
- Nasopharynx lies in anteroposterior plane and this will obscure the majority of the cavity from view
Interventions
- Initial (Woodpecker/Walrus technique)
- Have patient blow nose to remove clots
- In a small basin mix any or all of the following:
- Oxymetazoline
- Lidocaine with epinephrine
- Tranexamic acid
- If available, soak GelFoam/Surgicel in this fluid and place BEFORE the sponge sticks
- Trim two oral sponge swabs to better fit in the nasal cavity and soak in the fluid
- Make a nasal bridge clamp by taping two tongue depressors together on one end
- Place swabs in nasal cavities and apply nasal clamp for 10-15 minutes
- Ice pack can also be used
- Cautery
- If the bleeding site can be visualized on direct examination
- Apply topical anesthetic
- Silver nitrate sticks
- Start from periphery and roll to center of bleeding
- No more than 10 seconds
- A white eschar should form

- Nasal packing
- Use if cautery fails
- Ensure topical anesthesia
- Soak in sterile water
- Insert by sliding along the floor of the nasal cavity PARALLEL to floor
- Insufflate the balloon with air
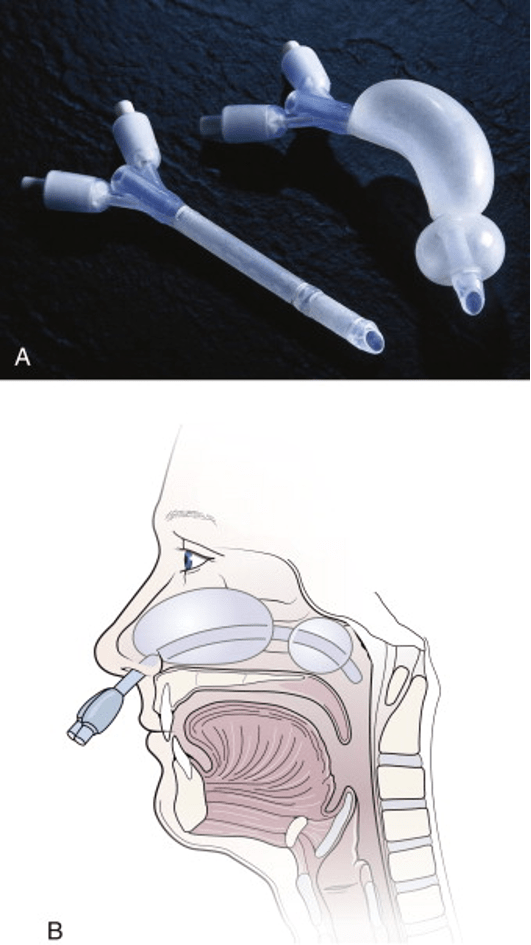
- Nasal Balloon Catheters
- For posterior bleeds
- Follow same steps for nasal packing
- Insufflate posterior balloon FIRST and apply gently traction
- Then insufflate the anterior balloon
- Foley Catheters
- If you don’t have a prefabricated nasal balloons, a foley catheter can work
- Insert the catheter until you can see it in the posterior oropharynx
- Insufflate with 5-10cc of water
- Apply traction to seat balloon in posterior choana
- Add additional water to tamponade
- Clamp catheter with umbilical clamp or c-clamp from NG tube

Disposition and Follow-up
- For simple nasal packing, patients should be evaluated by ENT within 24-48 hours
- Discuss with consultant need for antibiotic prophylaxis
- No good evidence supports routine use, but ENT often prefers
- Amoxicillin-Clavulanate is most commonly used
- Clindamycin or trimethoprim/sulfamethoxazole should be used if concern for nasal carrier of MRSA
- No good evidence supports routine use, but ENT often prefers
- Discuss with consultant need for antibiotic prophylaxis
- Posterior bleeds should be immediately assessed by ENT for potential surgical intervention
- Endoscopic sphenopalatine artery ligation
- Anterior ethmoid artery ligation
- Open or endoscopic

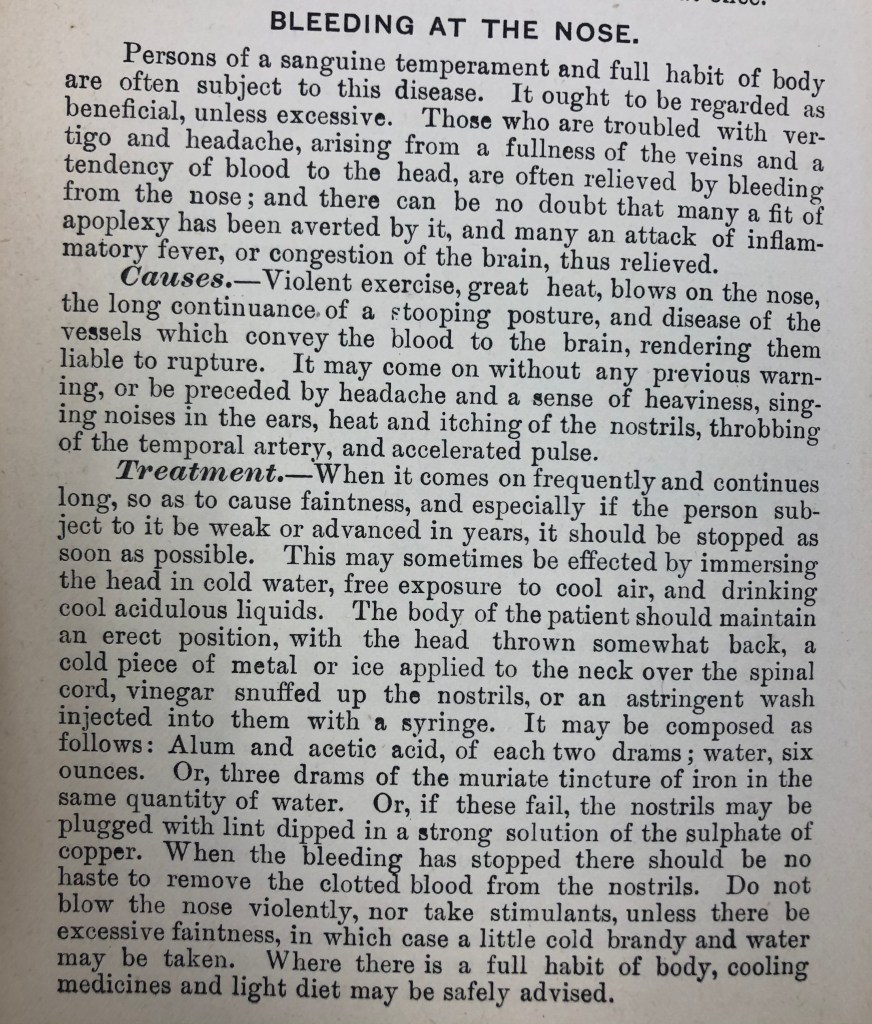
1893 Cottage Physician
References
- Kucik CJ, Clenney T. Management of epistaxis. Am Fam Physician. 2005; 71(2):305-11. [pubmed]
- Villwock JA, Jones K. Recent Trends in Epistaxis Management in the United States JAMA Otolaryngol Head Neck Surg. 2013; 139(12):1279-84. [pubmed]
- Kotecha B, Fowler S, Harkness P, Walmsley J, Brown P, Topham J. Management of epistaxis: a national survey. Ann R Coll Surg Engl. 1996; 78(5):444-6. [PDF]
- Fishpool SJ, Tomkinson A. Patterns of hospital admission with epistaxis for 26,725 patients over an 18-year period in Wales, UK. Ann R Coll Surg Engl. 2012; 94(8):559-62. [PDF]
- Min HJ, Kang H, Choi GJ, Kim KS. Association between Hypertension and Epistaxis: Systematic Review and Meta-analysis. Otolaryngol Head Neck Surg. 2017; 157(6):921-927. [pubmed]
- Shakeel M, Trinidade A, Iddamalgoda T, Supriya M, Ah-See KW. Routine clotting screen has no role in the management of epistaxis: reiterating the point. Eur Arch Otorhinolaryngol. 2010; 267(10):1641-4. [pubmed]
- Lin G, Bleier B. Surgical Management of Severe Epistaxis. Otolaryngol Clin North Am. 2016; 49(3):627-37. [pubmed]
