
***LISTEN TO THE PODCAST HERE***
PURPOSE
- The first full examination of the child’s life
- Occurs within 24 hours after birth
- Comprehensive review of history (maternal, family, prenatal) and complete physical examination
- Identify medical conditions while still in the hospital to address any significant pathologies
- Congenital anomalies, birth injuries, cardiopulmonary disease, neurologic abnormalities
HISTORY
- Maternal and Family History
- Chronic medical conditions, medications taken during pregnancy, dietary habits during pregnancy, tobacco/alcohol/substance use during pregnancy
- UTIs, PIH, eclampsia, gestational diabetes, vaginal bleeding
- Family history of congenital anomalies
- Chronic medical conditions, medications taken during pregnancy, dietary habits during pregnancy, tobacco/alcohol/substance use during pregnancy
- Obstetric History
- Maternal age (<19 or >35), gravidity and parity, pregnancy outcomes, blood type
- Procedures and tests performed during pregnancy (US, amniocentesis)
- Results any antepartum well-being tests
- Peripartum History
- Maternal fever
- Duration of labor
- Fetal distress
- Duration of ruptured membranes
- Type of delivery, anesthesia used, complications
- Any resuscitative measures performed
APGAR Scores
- Recorded at 1- and 5-minutes after birth
- Score out of 10, 2 points for each criteria
- < 7 warrants resuscitation and intervention
- Appearance, Pulse, Grimace, Activity, Respiration (APGAR)
- How (heart rate) Ready (respiration) Is (irritability) This (tone) Child (color)

ASSESSMENT OF GESTATIONAL AGE AND PHYSICAL MATURITY
- Important to calculate to determine what is physiologically “normal” for the infant

MEASUREMENTS
- Compared in relation to gestational age
- Birth weight
- Appropriate for Gestational Age (AGA)
- Small for Gestational Age (SGA) or Intrauterine Growth Restriction (IUG)
- < 10th percentile
- Low-Birth Weight < 2500g
- Very-Low Birth Weight < 1500g
- Large for Gestational Age (LGA)
- >90th percentile
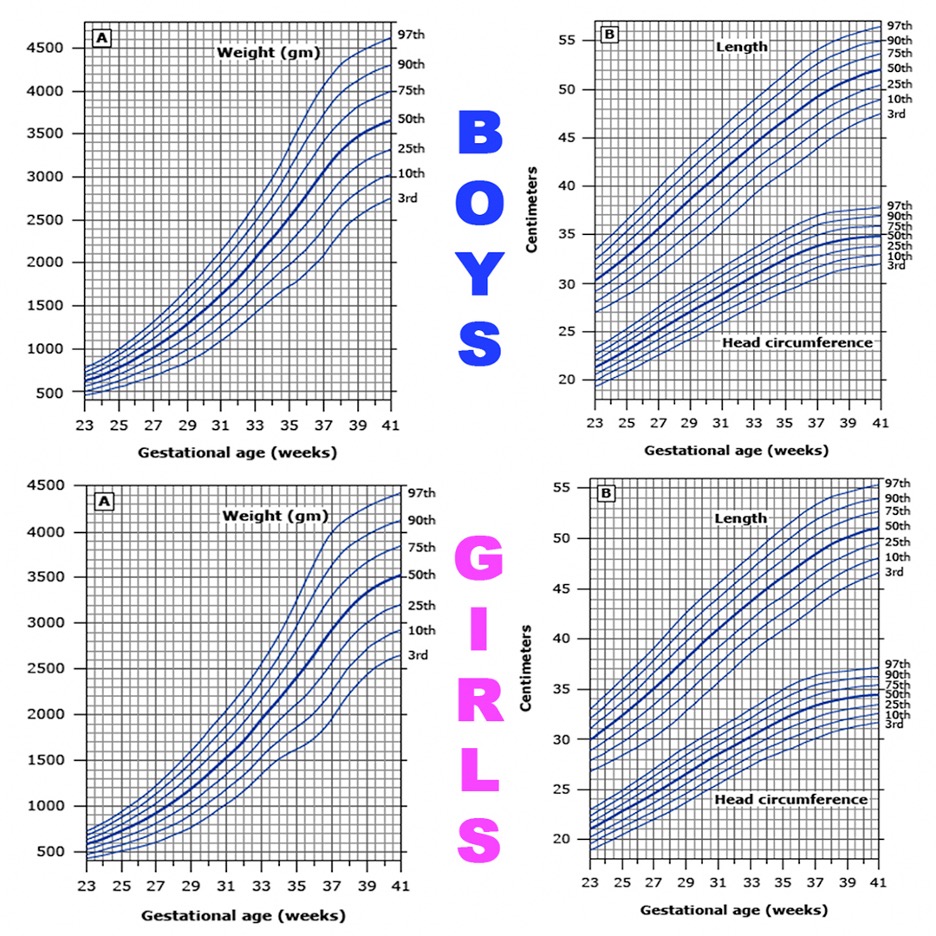
- Length and Head Circumference
- Length = top of head to bottom of feet with legs fully extended
- HC = above eyebrows around most prominent posterior aspect of head
- Use Olson Growth Curves to determine percentiles by gender
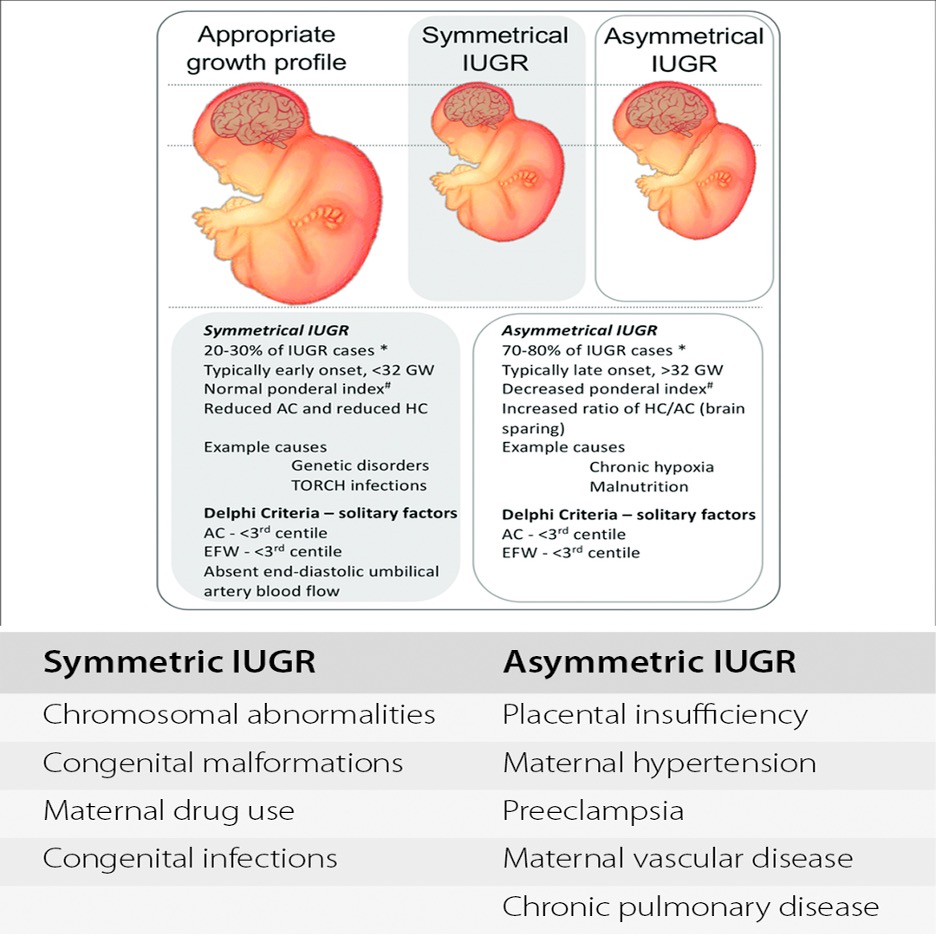
- If SGA/IUG, then determine if symmetrical or asymmetrical
- Symmetrical = weight, length, AND head circumference all < 10th percentile
- Implies early pregnancy event
- Asymmetrical = only weight < 10th percentile
- Implies late pregnancy event
- Symmetrical = weight, length, AND head circumference all < 10th percentile
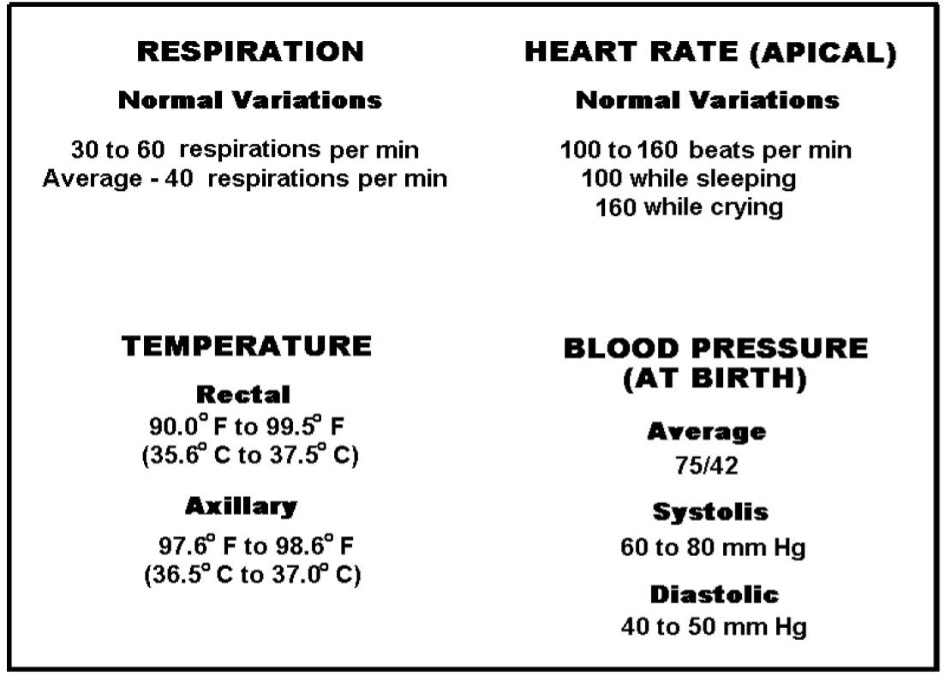
VITAL SIGNS
- Should be documented every 30-60 minutes for first 6 hours of life, then every 8-12 hours
- Axillary temperature (36.5-37.5oC) (97.7-99.5oF)
- Any deviation from normal, proceed with rectal measurement
- Respiratory Rate (35-60 bpm)
- Counted over a FULL minute
- Heart Rate (100-160 bpm)
- Blood Pressure (60-80/30-50 mmHg)
- General rule = MAP > GA
SKIN

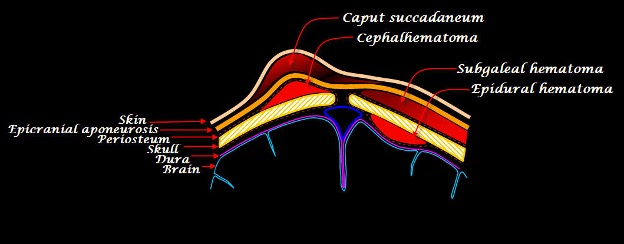
HEAD
- Assess the shape and size of the head
- Presence of any abnormal hair/scalp defects, unusual protuberances
- Cephalohematoma
- Subperiosteal collection of blood
- Does NOT cross suture lines, resolves over several weeks
- Caput succedaneum
- Edema over presenting part of the head
- Crosses suture lines, resolves in a few days
- Subgaleal hematoma
- Collection of blood between aponeurosis and periosteum of scalp
- Crosses suture lines, may be significant enough to cause hemodynamic problems
- Cephalohematoma
- Fontanelles and Sutures
- Anterior
- Posterior
- Should be open, soft, and flat
- Closed = craniosynostosis
- Tense, bulging = raised ICP, infections

FACE
- Examine for symmetry during crying
- Facial Palsies
- Usually associated with forceps delivery with injury to the mandibular branch of the facial nerve
- Loss of nasolabial fold, partial closing of the eye, inability to contract lower facial muscles
- Generally, resolve over days to weeks
- Persistent palsy may indicate complete nerve laceration
- Usually associated with forceps delivery with injury to the mandibular branch of the facial nerve

- Asymmetric Crying Facies (ACF)
- Syndromic condition due to congenital absence of depressor anguli oris muscle
- Eye and forehead muscles normal, only affects the mouth

EYES
- Spacing
- Wide interpupillary distances suggest syndromic abnormality

- Symmetry
- Prominent epicanthal folds, size of globes, ptosis
- Palpebral Fissures
- Wide or narrow palpebral fissures can be normal or syndromic
- Examine sclera, conjunctiva, cornea, pupils for abnormalities
- Red Light Reflex

EARS
- Examine for position, size, and appearance
- Normal position = helix intersected by horizontal line drawn from outer canthus of eye perpendicular to the vertical axis of the head
- Preauricular skin tags, branchial cleft cysts, and pits could indicate syndromic conditions

NOSE
- Assess for patency, shape, and position
- Hold mirror or cold metal under nose and look for bilateral fogging
- Any concern for patency should be assessed with small NG tube passage
MOUTH
- External
- Assess for size and shape, cleft lip, micrognathism
- Internal
- Epstein pearls = benign, small, white inclusion cysts on palate
- Lingual frenulum
- Cleft of palate
- Macroglossia associated with syndromic conditions

NECK
- Masses
- Cystic hygromas – transilluminated, soft mass above clavicles, posterior to SCM
- Branchial cleft cysts – anterior margin of SCM
- Thyroglossal cysts – midline neck mass

- Mobility
- Torticollis – caused by birth injury or neurologic syndrome
- Excessive Skin
- Webbing – feature of syndromic or genetic conditions

CLAVICLES
- Palpate for BOTH clavicles
- Absence associated with congenital syndrome
- Fractures or birth injuries
CHEST
- Assess for size, symmetry, and structure during respirations
- Pectus excavatum, pectus carinatum

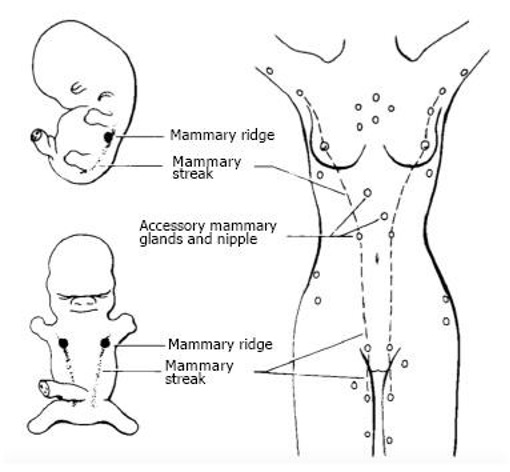
BREAST
- Nipple spacing
- Wide spaced may be associated with genetic conditions
- Supernumerary nipple presence along milk line
LUNGS
- Assess for retraction, grunting, nasal flaring
- Abnormal breath sounds are unusual in the absence of other respiratory distress findings
CARDIAC
- PMI in newborn is near left lower sternal border
- RV is dominant in the newborn
- Auscultation for murmurs
- Most newborns have benign, transient flow murmur as physiology shifts from in-utero to ex-utero
- Assess for potential cyanotic congenital defects
- Pulses
- Palpate femoral pulses
- If diminished, evaluate for coarctation of aorta
- Upper and lower BP
- If diminished, evaluate for coarctation of aorta
- Palpate femoral pulses
ABDOMEN
- Assess for size and protuberance
- Distension – congenital intestinal atresia, organomegaly, ascites
- Scaphoid – diaphragmatic hernia
- Assess for abdominal wall defects or masses
- Palpate for tenderness or organomegaly
- Umbilical Cord Stump
- Assess for erythema or streaking of omphalitis

GENITALIA
- Identify infant’s gender at birth
- Phenotypic Female
- Assess size and location of labia, clitoris, meatus, vaginal opening
- Phenotypic Male
- Presence of both testes, size of penis, appearance of scrotum, position of urethral opening
- Ambiguous Genitalia
- Female – enlarged clitoris, fused labial folds
- Males – bifid scrotum, severe hypospadias, micropenis, cryptorchidism
- Consultation with endocrinology, urology, and genetics is warranted
ANUS
- Assess location, patency, sphincter tone

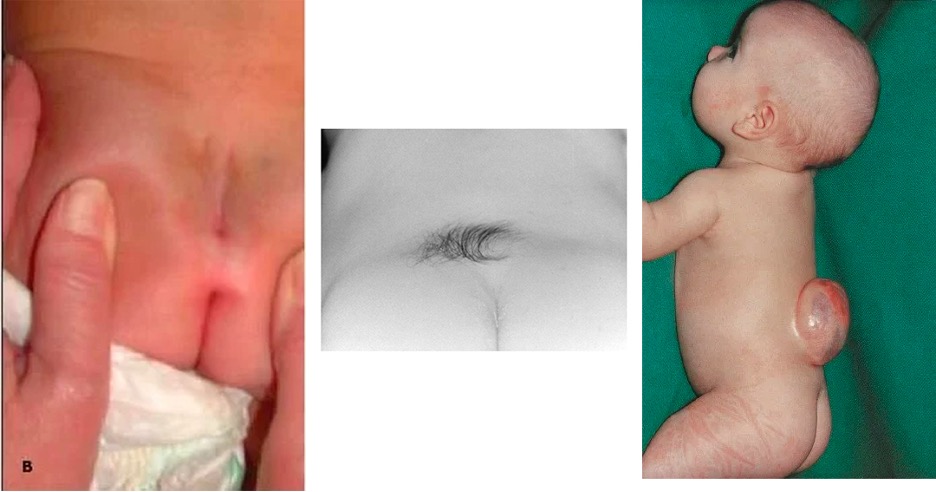
TRUNK AND SPINE
- Assess down vertebral column for masses, hair tufts, dimples
EXTREMITIES
- Hands and Feet
- Inspect for syndactyly or polydactyly
- Single palmar crease

- Hips
- Assess for developmental hip dysplasia
- Ortolani – adduction and posterior pressure to feel dislocation
- Barlowe – abduction and elevation to feel for reduction
- Assess for developmental hip dysplasia
- Movement
- Assess for spontaneous and symmetric movement
- If upper asymmetric movement present:
- Assess for brachial plexus injury
- C5-6 – Erb’s Palsy
- Upper arm is adducted, internally rotated, forearm extended (Waiter’s tip)
- C7-T1 – Klumpke Palsy
- forearm extension and pronation and flexion of wrist and fingers (“claw hand”)
- C5-6 – Erb’s Palsy
- Assess for brachial plexus injury
- If upper asymmetric movement present:
- Assess for spontaneous and symmetric movement

NEUROLOGIC
- Assess resting motor tone
- Hypertonia
- Spasticity, tractional positioning
- Hypotonia – infant lying supine with hips fully abducted (frog-leg position) and limbs fully extended
- Vertical Suspension Test
- Decreased shoulder girdle tone allows infant to slip through examiner’s hands
- Ventral Suspension Test
- Infant appears limp with extended limbs and head drooping
- Head Control Test
- Head lags behind as infant is pulled up from supine to sitting position
- Vertical Suspension Test
- Hypertonia

- Assess primitive reflexes
- Why important
- Brainstem mediated
- Complex automatic movement patterns (not really reflexes)
- Pathology may be present if absent when it should be present or present when it should be absent
- Why important
- Rooting and Sucking Reflex
- Rooting – infant turns head toward examiner stroking cheek or mouth
- Sucking – infant strongly latches onto finger
- Present – at birth
- Disappears – by 4 months
- Moro or Startle Reflex
- Lifting infants head and shoulders and allow head to drop relative to the body
- Normal – infant extends and abducts arms, then flexes and adducts
- Present – at birth
- Disappears – by 6 months
- Palmar Grasp Reflex
- Examiner places finger in the palm and applies gentle pressure
- Normal – fingers curl to grasp finger and hold
- Present – at birth
- Disappears – by 6 months
- Stepping Reflex
- Hold infant upright and slightly leaning forward and allow feet to touch a surface
- Normal – infant raises leg as if stepping
- Present – at birth
- Disappears – by 2 months
- Babinski Reflex
- Apply lateral pressure on plantar surface moving from heel curving towards 1st metatarsal
- Normal – fanning (extension) or toes
- This is a POSITIVE Babinski and NORMAL in infants
- Present – at birth
- Changes from POSITIVE to NEGATIVE by 2 year’s of age
- Asymmetric Tonic Neck Reflex
- Infant is supine and examiner turns head for 15 seconds
- Normal – Ipsilateral extremities extend and contralateral extremities flex
- Present – at birth
- Disappears – by 6 months
COTTAGE PHYSICIAN (1893)

REFERENCES
- Smith D. The Newborn Infant. In: Hay Jr. WW, Levin MJ, Abzug MJ, Bunik M. eds. Current Diagnosis & Treatment: Pediatrics, 25e. McGraw-Hill; Accessed April 24, 2021. https://accessmedicine-mhmedical-com.ezproxy.uthsc.edu/content.aspx?bookid=2815§ionid=244254981
- Ballard JL, Khoury JC, Wedig K, Wang L, Eilers-Walsman BL, Lipp R. New Ballard Score, expanded to include extremely premature infants. J Pediatr. 1991; 119(3):417-23. [pubmed]
- Olsen IE, Groveman SA, Lawson ML, Clark RH, Zemel BS. New intrauterine growth curves based on United States data. Pediatrics. 2010; 125(2):e214-24. [pubmed]
- American Academy of Pediatrics, American College of Obstetricians and Gynecologists. Care of the Newborn. In: Guidelines for Perinatal Care, 7th ed, Riley LE, Stark AR (Eds), American Academy of Pediatrics, Elk Grove Village, IL 2012.
- Tveiten L, Diep LM, Halvorsen T, Markestad T. Respiratory Rate During the First 24 Hours of Life in Healthy Term Infants. Pediatrics. 2016; 137(4):. [pubmed]
- Red reflex examination in neonates, infants, and children. Pediatrics. 2008; 122(6):1401-4. [pubmed]
- Lewis ML. A comprehensive newborn exam: part I. General, head and neck, cardiopulmonary. Am Fam Physician. 2014; 90(5):289-96. [pubmed]
- Lewis ML. A comprehensive newborn exam: part II. Skin, trunk, extremities, neurologic. Am Fam Physician. 2014; 90(5):297-302. [pubmed]
- Salandy S, Rai R, Gutierrez S, Ishak B, Tubbs RS. Neurological examination of the infant: A Comprehensive Review. Clin Anat. 2019; 32(6):770-777. [pubmed]
- Hamer EG, Hadders-Algra M. Prognostic significance of neurological signs in high-risk infants – a systematic review. Dev Med Child Neurol. 2016; 58 Suppl 4:53-60. [pubmed]
- Futagi Y, Toribe Y, Suzuki Y. The grasp reflex and moro reflex in infants: hierarchy of primitive reflex responses. Int J Pediatr. 2012; 2012:191562. [PDF]
- Allen MC, Capute AJ. The evolution of primitive reflexes in extremely premature infants. Pediatr Res. 1986; 20(12):1284-9. [pubmed]
- Pediatric EM Morsels. Primitive Reflexes in Children. 04/23/2021. https://pedemmorsels.com/primitive-reflexes-in-infants/
