Definition – Autoimmune disease that can effect the entire system…most commonly skin, joints, and constitutional.
Clinical Significance – For this eponym, there is no clinical significance. Just a cool fact I wanted to bring up….
History – You may have been wondering (or maybe not) where the “lupus” part of this disease comes from. Having studied Latin in high school all four years, this perplexed me in PA school because “lupus” is Greek for wolf. So why did early physicians decide on throwing “wolf” into the disease title?
Well (since you asked), it has been attributed to the 13th century Rogerius (who practiced with his friend, Stevius) who thought the characteristic erosive, dermatologic skin findings were similar to the effects of a wolf bite.
For those fellow PotterHeads out there, now you know the foreshadowing of (my favorite character) Remus LUPIN in the series.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Blotzer JW. Systemic lupus erythematosus I: historical aspects. Maryland State Medical Journal. 1983; 32(6):439-41. [pubmed]
Bertino LS, Lu LC. The bite of a wolf: systemic lupus erythematosus. Rehabilitation nursing : the official journal of the Association of Rehabilitation Nurses. 1993; 18(3):173-8. [pubmed]
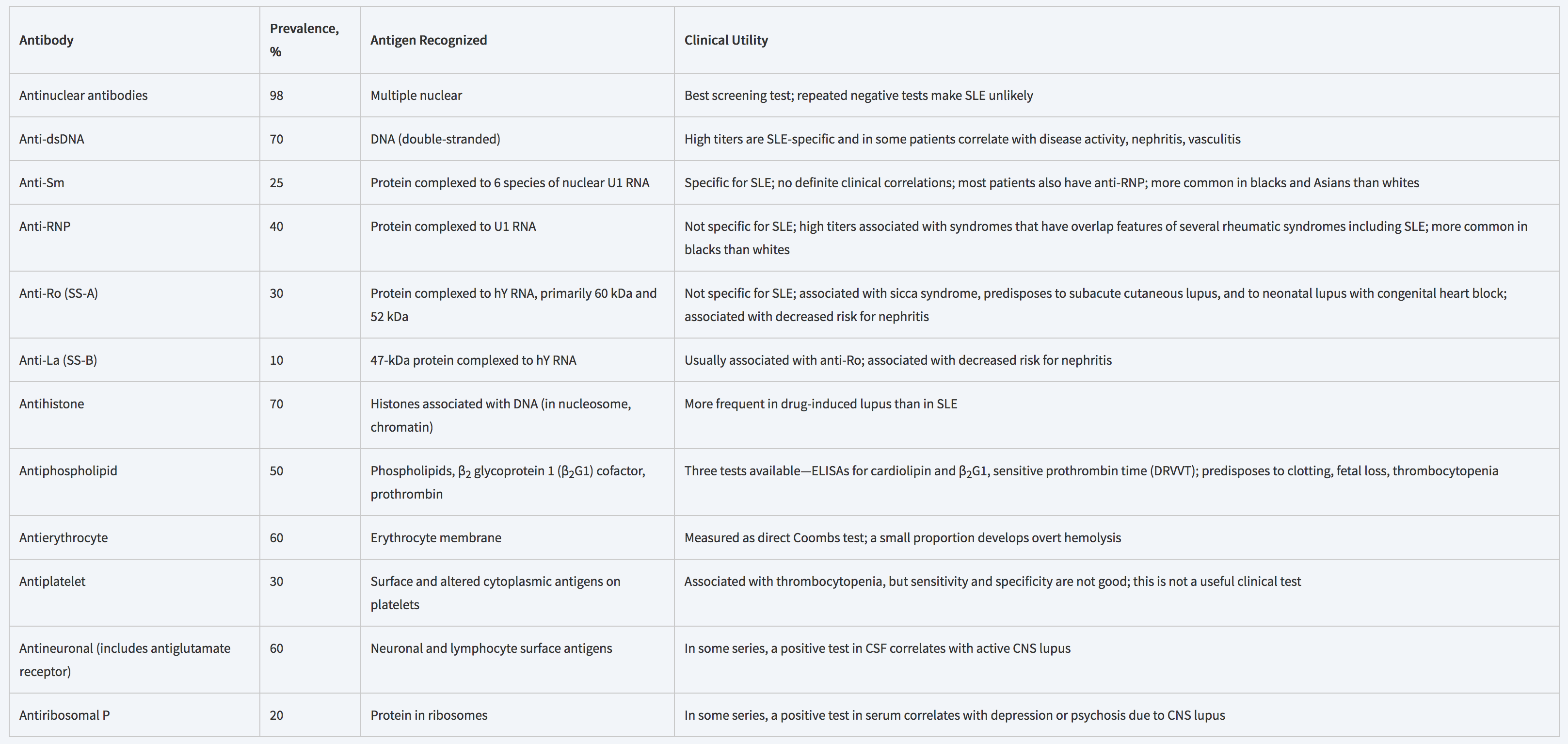
Anti-dsDNA is the MOST SPECIFIC for SLE when positive, but ANA is MOST SENSITIVE. This is why ANA is the antibody is used for screening and anti-dsDNA is used for confirming.
200,000-300,000 estimated new cases each year in the United States
Cause of approximately 10% of total hip replacements
Mean age at time of diagnosis is < 50 years
Pathogenesis and Etiologies
Current thoughts on exact mechanisms are an area of hot debate, but include:
Genetic predisposition
Metabolic factors
Vascular factors
Vascular damage
Increased intraosseous pressure
Mechanical stresses
80% of all atraumatic cases of AVN are due to:
Glucocorticoid Use
Theories
Microemboli in the arteries of the bone from alterations in lipid metabolism
Increased bone marrow adipocyte size and number causing decreased venous outlow
Changes venous endothelial cells of the bone leading to stasis and necrosis
Dose of prednisone < 15-20 mg/day has lowest risk of developing AVN (<3%)
Alcohol Use
Causes fat emboli, venous stasis, elevated cortisol, and adipocyte hyperrophy
While not considered an absolute risk factor, it is associated with up to 31% of AVN cases
Trauma can also predispose patients to develop AVN and most commonly associated with:
Femoral neck fracture
Hip dislocations
Other atraumatic causes of AVN include sickle cell disease, Gaucher disease, decompression disease, treatment for ALL, and transplantation
Signs and Symptoms
Pain
Groin, thigh, and/or buttock pain
Worse with weightbearing or motion
Although 2/3rd may have rest pain
1/3rd may have night pain
Decreased ROM with forced internal rotation and abduction
Limp
Imaging
Plain Radiographs
May not see any changes early in disease course
Progression of changes
Decreased density –> sclerosis –> subchondral radiolucency (crescent sign) and collapse
Magnetic Resonance Imaging
Much more sensitive than plain films
May see early changes undetectable on plain radiographs
T1 – Signal low-density line differentiating healthy and ischemic bone
T2 – Second high-density line showing hypervascular granulation
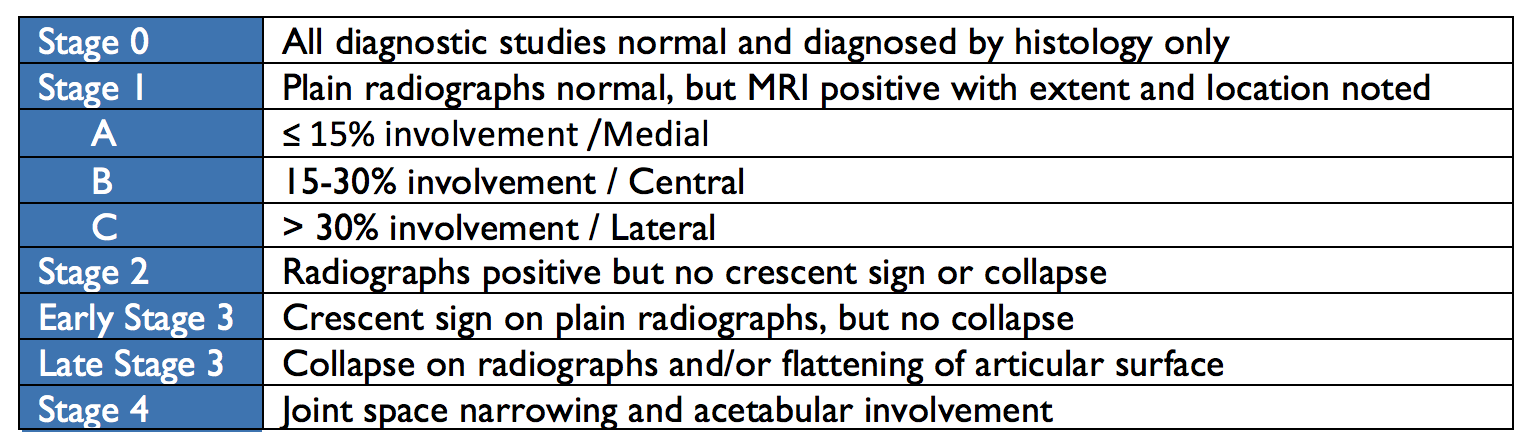
Classification and Staging
In 1993, The Association of Research Circulation Osseous (ARCO) staging system for AVN was developed to unify descriptions for treatment and research purposes.
Treatment
The goal of treatment is to preserve the native joint for as long as possible.
Nonoperative Management
Generally ineffective at halting the process
Includes bed rest, partial weightbearing, and pharmacotherapeutics
Bisphosphonates
Slows bone resorption
Vasodilators
Decrease intraosseous pressure and improve blow flow
Statins
Anticoagulants
Joint-Preserving Procedures
Core Decompression
Drills holes into femoral neck decrease pressure and allow for neovascularization
Displacement of the capital femoral epiphysis from the neck of the femur through the physeal plate anterolaterally and superiorly
Risk Factors
Obesity is #1 risk factor
> 60% of patients in > 90th percentile for weight
Renal failure
History of radiation therapy
Endocrine abnormalities
Hypothyroidism, GH deficiency
Signs and Symptoms
The most common clinical presentation of SCFE are pain and altered gait, but can be divided into four presentation patterns:
Preslip
(+) pain, but no radiographical displacement of epiphysis
May show widening of the physis
Acute
< 3 weeks duration
(+) joint effusion but no metaphyseal remodeling
10-15% of initially presentation of hip pain and often associated with trauma
Acute-on-chronic
Worsening symptoms in known SCFE
Chronic
Most common pattern of presentation
Vague, intermittent symptoms > 3 weeks
(+) metaphyseal remodeling but no effusion
Pain is classically characterized as dull, aching in the hip, groin, thigh, or knee. Physical exam reveals decreased internal rotation and abduction ROM with increased pain. Passively flexing the affected hip while the leg is extended will cause external rotation and abduction.
Stability
Stable Slips
Walking and weightbearing still possible with or without crutches
Unstable Slips
No ability to weightbear, even with crutches
No examination of the ROM of the hip should occur until orthopaedic consultation
Radiographic Evaluation
Most SCFE are diagnosed by plain radiography and have characteristic findings on each view:
AP view
Mild, widening, lucency, and irregularity of the physis
Blurring of the junction between metaphysis and growth plate
Klein’s Line
Normal = intersecting lateral portion of femoral head from superior femoral neck
SCFE = line passes outside of epiphysis
Lateral View
Usually obtained via frog-leg or cross-table
Unstable SCFE should have true lateral
Posterior displacements are best seen on lateral views
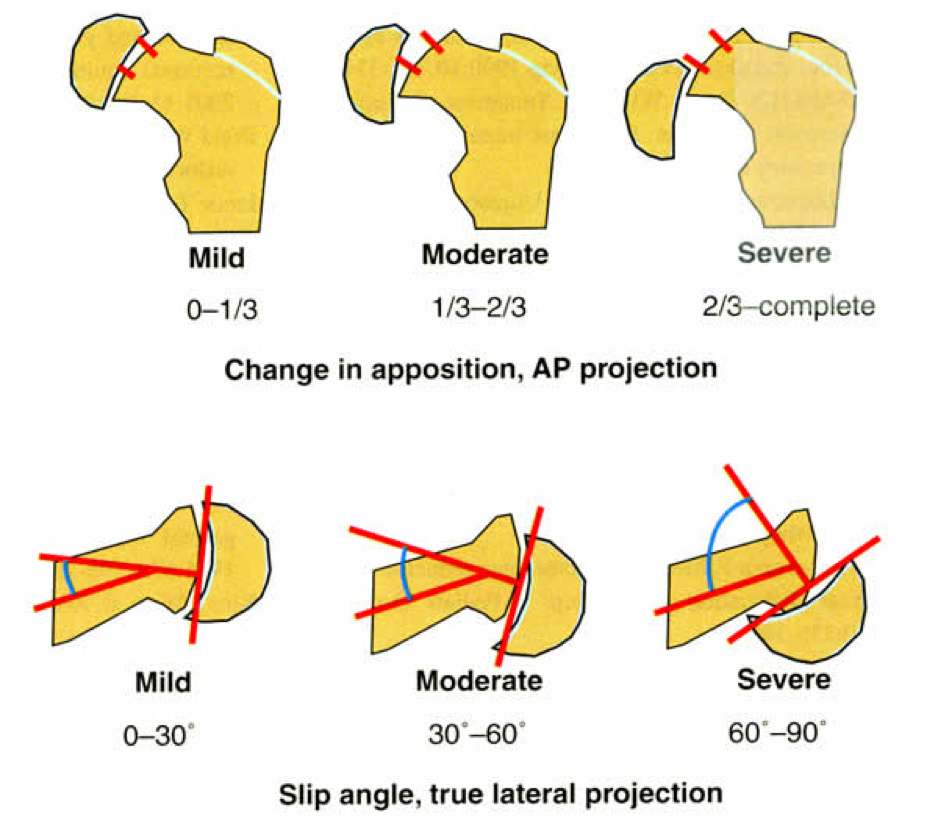
Grading of Severity
2 ways to grade severity: Displacement of femoral neck or Angle of Southwick.
Displacement
Mild = < 1/3rd the diameter of the femoral neck
Moderate = > 1/3rd, but < 2/3rd the diameter of the femoral neck
Severe = > 2/3rd the diameter of the femoral neck
Angle of Southwick
Mild = < 30o
Moderate = 30-60o
Severe = > 60o
Treatment
All SCFEs must be repaired surgically and the goals of surgery are to stabilize the diseased physis to prevent further slippage and avoid complications (AVN). Treatment of choice is a single cannulated screw placed in the center of the epiphysis.
References
Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World Journal of Orthopedics. 2015; 6(8):590-601. [pubmed]
Mankin HJ. Nontraumatic necrosis of bone (osteonecrosis). The New England journal of medicine. 1992; 326(22):1473-9. [pubmed]
Jones JP. Fat embolism and osteonecrosis. The Orthopedic clinics of North America. 1985; 16(4):595-633. [pubmed]
Dilisio MF. Osteonecrosis following short-term, low-dose oral corticosteroids: a population-based study of 24 million patients. Orthopedics. 2014; 37(7):e631-6. [pubmed]
Fukushima W, Fujioka M, Kubo T, Tamakoshi A, Nagai M, Hirota Y. Nationwide epidemiologic survey of idiopathic osteonecrosis of the femoral head. Clinical orthopaedics and related research. 2010; 468(10):2715-24. [pubmed]
Shigemura T, Nakamura J, Kishida S. The incidence of alcohol-associated osteonecrosis of the knee is lower than the incidence of steroid-associated osteonecrosis of the knee: an MRI study. Rheumatology (Oxford, England). 2012; 51(4):701-6. [pubmed]
Slobogean GP, Sprague SA, Scott T, Bhandari M. Complications following young femoral neck fractures. Injury. 2015; 46(3):484-91. [pubmed]
LaPorte DM, Mont MA, Mohan V, Jones LC, Hungerford DS. Multifocal osteonecrosis. The Journal of rheumatology. 1998; 25(10):1968-74. [pubmed]
Mont MA, Hungerford DS. Non-traumatic avascular necrosis of the femoral head. The Journal of bone and joint surgery. American volume. 1995; 77(3):459-74. [pubmed]
Loder RT. The demographics of slipped capital femoral epiphysis. An international multicenter study. Clinical orthopaedics and related research. 1996; [pubmed]
Benson EC, Miller M, Bosch P, Szalay EA. A new look at the incidence of slipped capital femoral epiphysis in new Mexico. Journal of pediatric orthopedics. 2008; 28(5):529-33. [pubmed]
Murray AW, Wilson NI. Changing incidence of slipped capital femoral epiphysis: a relationship with obesity? The Journal of bone and joint surgery. British volume. 2008; 90(1):92-4. [pubmed]
Koop S, Quanbeck D. Three common causes of childhood hip pain. Pediatric clinics of North America. 1996; 43(5):1053-66. [pubmed]
Causey AL, Smith ER, Donaldson JJ, Kendig RJ, Fisher LC. Missed slipped capital femoral epiphysis: illustrative cases and a review. The Journal of emergency medicine. 1995; 13(2):175-89. [pubmed]
Reynolds RA. Diagnosis and treatment of slipped capital femoral epiphysis. Current opinion in pediatrics. 1999; 11(1):80-3. [pubmed]
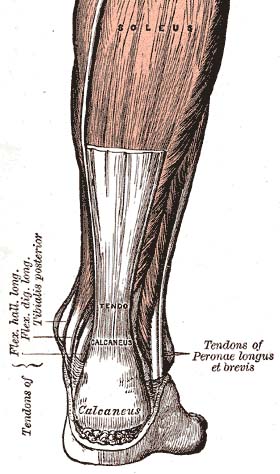
Definition – The tendon attaching the gastrocnemius, plantaris, and soleus muscle to the calcaneus.
Clinical Significance – The Achilles tendon is the thickest tendon in the body and rupturing this structure takes a tremendous amount of force. Powerful plantarflexion while jumping is the most common mechanism and most commonly occurs in inflammed or chronically stressed tendons.
History – I am a bit of a mythology geek and I love this eponym. The Achilles tendon was named after the famous Greek warrior, Achilles, who was the hero of the Trojan War for killing Prince Hector, son of King Priam of Troy. This is a major part of Homer’s Illiad.
I digress…..
The reason for this eponym is that Achilles’ mother is Thetis, an immortal sea nymph, who could not bear to see her child injured or killed. To remedy this, she dipped him in the River Styx to make him invulnerable. Since he was mortal, she couldn’t just drop him in, so she held him by the heel. The spot on his heel that was held by Thetis was unprotected and ultimately would be his “Achilles Heel” (get it) when an arrow shot by Paris, brother of Hector, pierced this spot and killed him.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
What is a good mnemonic for the red flag history and/or symptoms of acute back pain?
Answer
The majority of the back pain you will see in clinical practice is non-emergent, but you need to be able to identify the cases that need emergent referral, consultation, or imaging. Just remember TUNAFISH……
Trauma
Any trauma can cause fracture and cord compromise. Back pain + trauma = imaging
Unintentional weight loss
Think vertebral metastasis of cancer
Neurologic deficits
Big ones are saddle anesthesia and bowel/bladder dysfunction. Paresthesias, weakness, and numbness are concerning, but emergent.
Age > 50
New-onset back pain in patients > 50 years old can be cancer, infection, or AAA
Fever
Again…think osteomyelitis, spinal abscess, or cancer
IVDU
Hematogenous infectious seeding of the vertebral bodies or spinal abscess
Steroid Use
Chronic steroid use weakens bones and even low energy mechanisms or spontaneous fractures are possible
History of cancer
Metastases
References
Della-Giustina D. Evaluation and treatment of acute back pain in the emergency department. Emergency medicine clinics of North America. 2015; 33(2):311-26. [pubmed]
Borczuk P. An evidence-based approach to the evaluation and treatment of low back pain in the emergency department. Emergency medicine practice. 2013; 15(7):1-23; Quiz 23-4. [pubmed]
Other Known Aliases – Tarsometatarsal fracture/dislocation
Definition – Fracture/dislocation of the articulation of the tarsal bones with the metatarsals of the foot.
Clinical Significance – The Lisfranc joint of the foot is where the first three metatarsals articulate with the three cuneiforms and the fourth and fifth metatarsals articulate with the cuboid. The Lisfranc ligament attaches the medial cuneiform to the 2nd metatarsal bone on the the plantar surface of the foot. This is a very serious injury of the foot and sometimes may simple present as a bad sprain. This injury is most common seen with direct crush injuries and indirect load onto a plantar flexed foot.
History – This injury was first described by Jacques Lisfranc de St. Martin (1790-1847), a French surgeon who served in Napoleon’s army in 1813. He noted this injury pattern in Calvary soldiers who fell from their horse and caught their foot in the stirrup.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Definition – Any fracture dislocation of the talus.
Clinical Significance – None. This is an antiquated term for talar injuries
History – First coined in 1919 by Henry Graeme Anderson, who was a consulting surgeon for the Royal Flying Corps during World War I. He described 18 cases of fracture and dislocation of the talus in pilots between 1914-1919. During the early history of flight, planes did not reach lethal speeds and when they crashed, the rudder bar (which was controlled by the pilot’s feet) would get driven up into the instep of the foot just anterior to the calcaneous.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Question #1 – What are the muscles that make up the rotator cuff?
Answer – Supraspinatus, Infraspinatus, Teres Minor, and Subscapularis
Question #2 – What is AT LEAST one maneuver to assess each of these muscles
Keep in mind, there are several maneuvers of the shoulder and many overlap into other structures. These are the more common individual maneuvers that I think general practice PAs need to know.
Supraspinatus
Drop Arm test
Description – Patient is seated with examiner to the front. Examiner grasps the patient’s wrist and passively abducts the patient’s shoulder to 90 degrees. Examiner releases the patient’s arm with instructions to slowly lower the arm. Test is positive if the patient is unable to lower his or her arm in a smooth, controlled fashion
Infraspinatus
Dropping Sign
Description – The patient stands with the arm at the side with the elbow at 90 degrees and the humerus medially rotated to 45 degrees. Patient then resists external rotation. Pain or the inability to resist medial rotation indicates a positive test for an infraspinatus strain.
Teres Minor
Hornblower (Patte) Test
Description – Elevate the patient’s arm to 90 degrees in the scapular plane and then flex the elbow to 90 degrees, and the patient is asked to laterally rotate the shoulder. A positive test occurs with weakness and/or pain.
Subscapularis
Lift Off (Gerber) Test
Description – The patient stands and places the dorsum of the hand against mid-lumbar spine. The patient then lifts hand away from the back. An inability to perform this action indicates subscapularis weakness or injury.