#BOOM


#BOOM

Question #1
Which of the following genetic mutations is seen with chronic myelogenous leukemia?
Answer:
Translocation of chromosome 9 and 22. This new chromosome 22 is called “Philadelphia chromosome” after the city where the two hospitals that first identified the gene mutation in 1960 were both located.
Question #2
Which of the following cancer markers are classically associated with ovarian cancer?
Answer:
CA-125


The textbook definition of anemia is a reduction of the absolute number or mass of circulating red blood cells. This then causes a global reduction in the oxygen carrying capacity of the patient’s circulatory system. Clinically, we use hemoglobin and hematocrit as the surrogate markers and define anemia as 2 SD below the mean for gender:

Patel KV. Haematologica. 2008;93(9):1281-1283.
There are two general approaches you can use to help identify the cause of anemia in adults.
Anemia is usually first diagnosed by CBC. Once you have a documented low H/H, then you need order follow-up studies to help differentiate the cause of the anemia. These include:

Schrier SL, et al. Approach to adults with anemia. In: Up To Date. Waltham, MA (Accessed 03/23/2016)
Something new I thought I would bring to the PAINE Podcast. As you all know, I am quite a fan of medicine and antiquity. Shortly after I married my wife, her grandfather past away from a progressive esophageal cancer. One of the things I was able to keep when helping clean out his house, was a copy of The Cottage Physician printed in 1893. It was basically a handbook on how to treat common ailments of the time. I will try to add excerpts from this book when appropriate so you can have a sense of how medicine was practiced in the late 19th century.
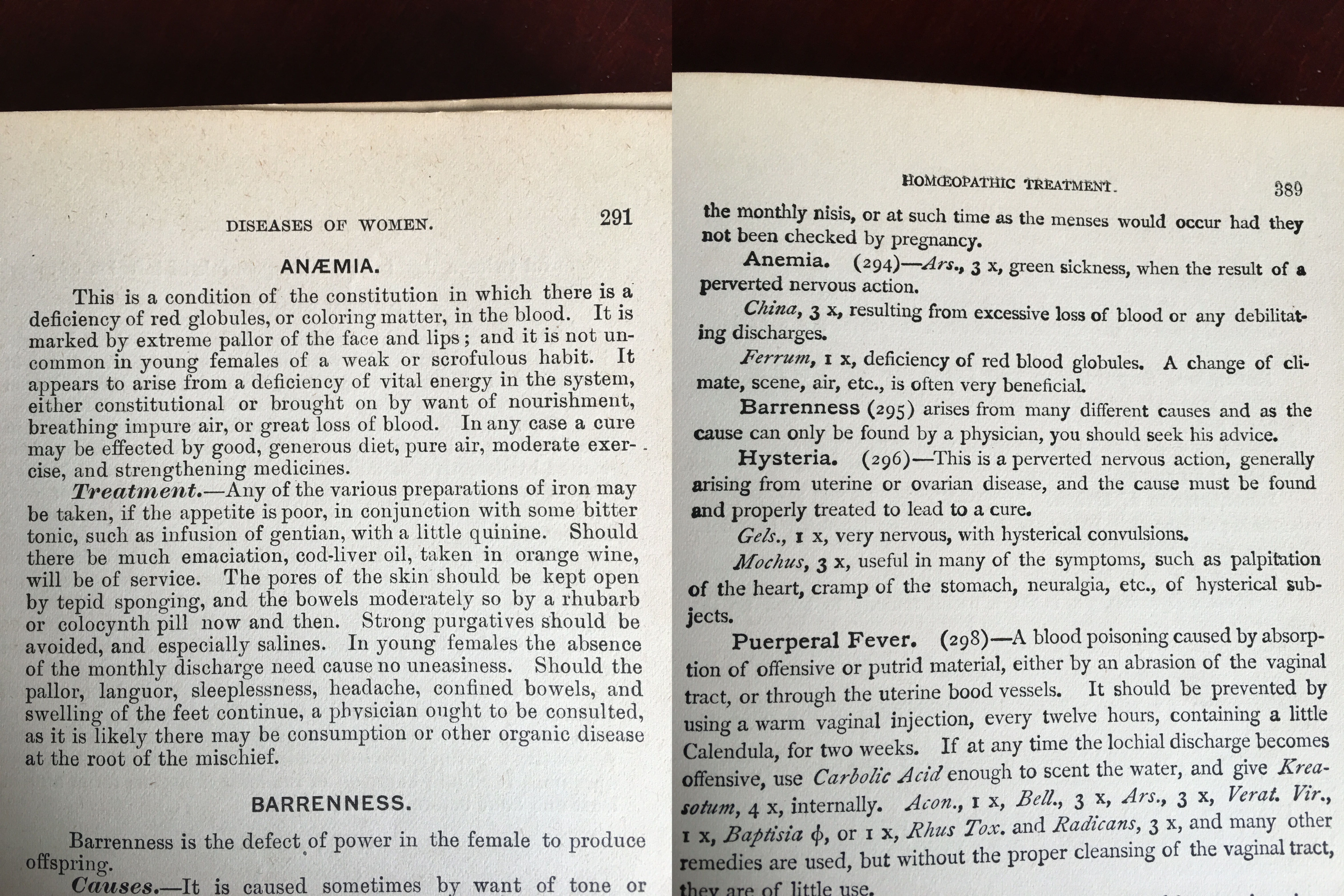
The Cottage Physician. 1863
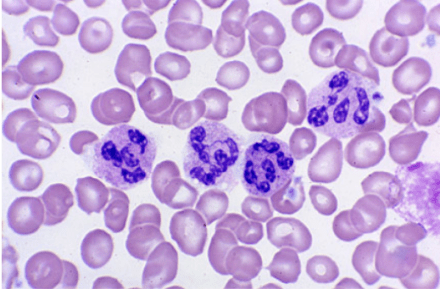
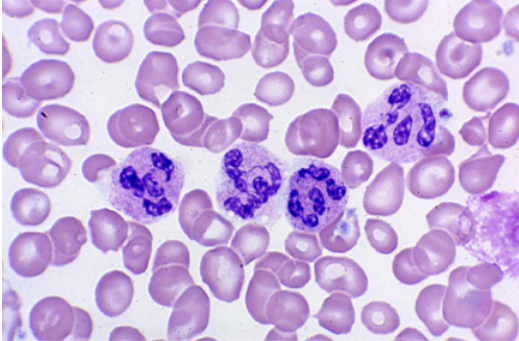
This patient has had a history of gastric cancer with a partial gastrectomy and now presents with a fatigue and gait disturbances. CBC reveals a macrocytic aneamia and peripheral smear shows multinucleated neutrophils. The gait disturbances are most likely due to the progressive peripheral neuropathy. This is most consistent with vitamin B12 deficiency. Intrinsic factor, which is secreted by the parietal cells of the stomach, is required for vitamin B12 absorption in the terminal ileum.
Work-Up for Vitamin B12 Deficiency
Serum B12 Level
Metobolites
Possible additional testing in the setting of macrocytic anemia:
Treatment for B12 Deficiency
References
62-year-old male presents to primary provider’s office with a six-month history of fatigue and gait disturbance. He denies recent falls, weakness, pain, paralysis, or dizziness.
Medications
Lisinopril 10mg daily
Metformin 1000mg BID
Men’s multivitamin
Fish oil
Past Medical History
Diabetes Mellitus II
Hypertension
Gastric cancer
Past Surgical History
Cholecystectomy – 1997
Partial gastrectomy – 2004
Vitals
BP-128/79, HR-81, RR-14, O2-100%, Temp-98.9o
Physical Exam
General – WN/WD, NAD
Skin – scattered senile purpura, no petechiae
CV – RRR without M/G/R
Pulmonary – CTA bilaterally without adventitial breath sounds
Neurologic – A&Ox3, 5/5 strength throughout bilaterally, DTR 2+ and equal, FROM, vibratory sensation decreased in bilateral lower extremities
Laboratory Studies
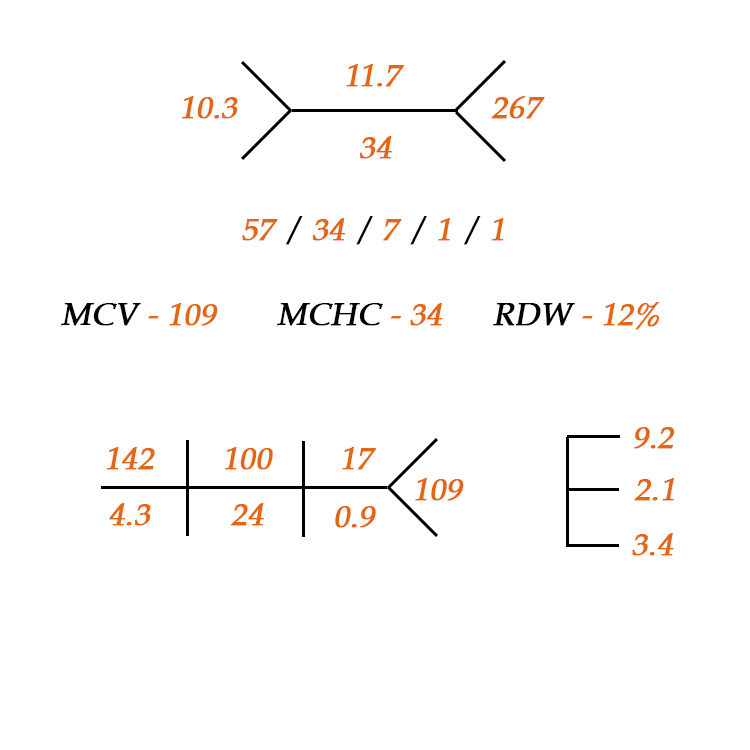


Fishbone diagram for CBC with differential
References
1) Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboratory Tests. 5th ed. St. Louis, MO. Elsevier. 2014.
2) Lee M. Basic Skills in Interpreting Laboratory Data. 5th ed. Bethesda, MD. American Society of Health-Systems Pharmacists. 2013
3) Laposata M. Laboratory Medicine: The Diagnosis of Disease in the Clinical Laboratory. 2nd ed. New York, NY. 2014.


