
***LISTEN TO THE PODCAST HERE***
Classifications of Pneumonia
- Community-Acquired (CAP)
- Healthcare-Associated (HAP)
- Any IV therapy, wound care, or chemotherapy within 20 days
- Resident of nursing home or other long term care facility
- Hospitalization for ≥ 2 days within 90 days
- Visit to outpatient clinic or hemodialysis within 30 days
- Ventilator-Associated (VAP)
- Currently or previously intubated during current hospitalization
Epidemiology
- 6 cases per 1000 persons per year (~ 5 million cases per year)
- Top 10 in mortality in US (~60,000 deaths/year)
- 12% 30-day mortality in patients requiring admission
- 28% all-cause mortality within one year
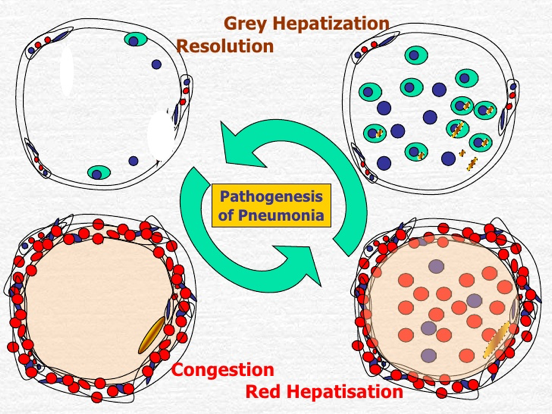
Pathogenesis
4 phases of development
- Edema
- Proteinaceous exudate in the alveoli
- Bacteria accumulation
- Red hepatization
- Erythrocyte extravasation
- Grey hepatization
- Neutrophil extravasation with bacterial clearance
- Resolution
- Macrophage proliferation with inflammatory response
Risk Factors
- Age
- Winter months
- Increased risk of aspiration (AMS, CVA, intoxication, seizures)
- Smoking
- Underlying pulmonary disease (Asthma, COPD, cancer)
- Immunosupression
- Viral URI
- Decreased host defenses (impaired ciliary clearance)
- Acid-reducing medications
- Malnutrition
- Inhalation exposures
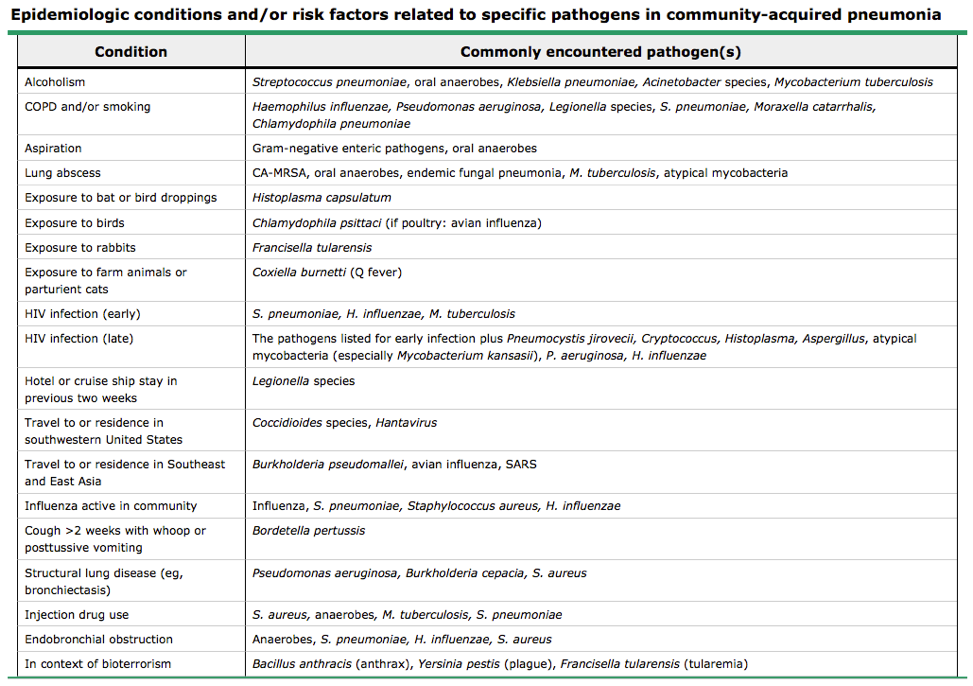
Pathogens
- Viral (most common)
- Rhinovirus (most common)
- Influenza
- Adenovirus
- Respiratory Syncytial Virus (RSV)
- Bacterial
- S. pneumoniae (most common CAP)
- H. influenza
- M. pneumoniae (most common atypical)
- K. pneumoniae (tends to be more severe)
- Legionella
- ESKAPE bugs (>80% of VAP)
- Enterococcus
- Staphylococcus
- Klebsiella
- Acinetobacter
- Pseudomonas
- Enterobacter
- Fungal (immunocompromised)
- Histoplasmosis
- Cryptococcus
- Coccidioides
- Blastomycosis
- Aspergillus
Signs and Symptoms
- Productive cough
- Fever
- Chills and/or rigors
- Dyspnea
- Pleuritic chest pain
- Nausea/vomiting
- Altered mental status
Physical Exam Findings
- Vital signs
- Febrile (elderly may not mount a response)
- Tachycardic
- Tachypnic
- Pulmonary
- Rales and/or rhonchi
- Signs of consolidation
- Decreased breath sounds
- Dullness to percussion
- Increased tactile fremitus
- Egophany
- Whispered pectoriliquoy
Radiographic Evaluation
- Bacterial
- Unilateral, lobar, air bronchograms

- Viral
- Diffuse or perihilar, bilateral

Laboratory Evaluation
- CBC with differential
- Blood cultures
- Sputum culture and gram stain
- Good sample = PMNs with < 10 squamous cells per LPF
- Urine antigen (pneumococcal and Legionella)
- Multiplex PCR

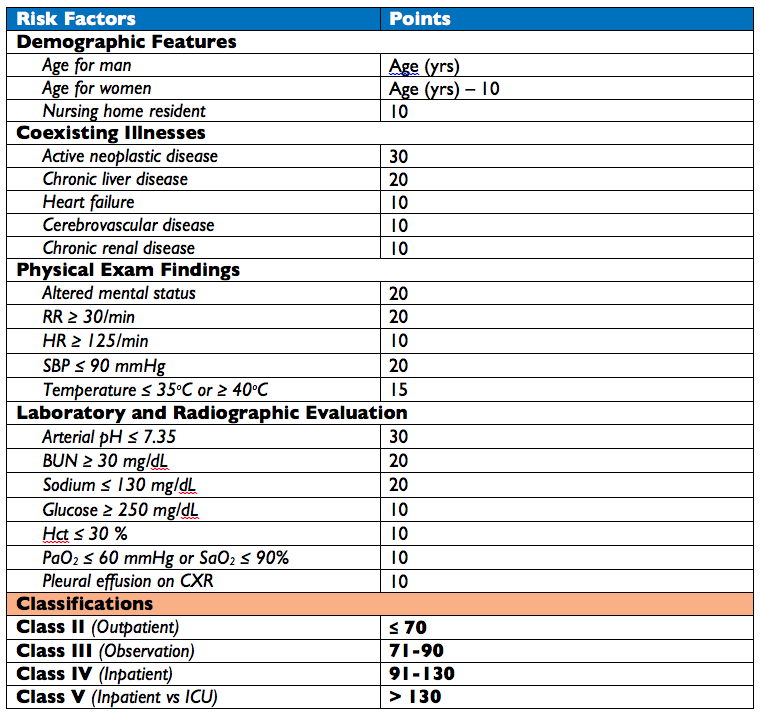
Should They Stay or Should They Go Now????
- Pneumonia Severity Index (PSI)
- Step 1
- If none of the following, then Class I and outpatient treatment
- Age > 50 years
- Neoplastic disease
- Heart failure
- Cerebrovascular disease
- Renal disease
- Liver disease
- Altered mental status
- HR ≥ 125/min
- RR ≥ 30/min
- SBP ≤ 90 mmHg
- Temperature ≤ 35oC or ≥ 40oC
- If none of the following, then Class I and outpatient treatment
- Step II
- Step 1
- CURB-65 Score
- 5 variables
- Confusion
- Urea (BUN ≥ 20 mg/dL)
- Respiratory rate ≥ 30/min
- Blood pressure (SBP < 90 mmHg or DBP < 60 mmHg)
- Age ≥ 65 years
- Interpretation
- Score 0-1 = Outpatient management
- Score 2-3 = Inpatient management
- Score 4-5 = ICU management
- 5 variables
- SMART-COP Score
- Used to predict need for respiratory or vasopressor support
Treatment
- Care should be taken to think about patients with risk factors for drug-resistant S. pneumoniae:
- Age > 65 years
- Beta-lactam, macrolide, or fluouroquinolone in the past 3-6 months
- Alcoholism
- Medical comorbidities
- Immunosuppression
- Exposure to child in daycare
- Community-Acquired
- Healthcare-Associated
Cottage Physician
References
- Mandell LA, Wunderink RG. Pneumonia. In: Kasper D, Fauci A, Hauser S, Longo D, Jameson J, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 19e. New York, NY: McGraw-Hill; 2015. http://accessmedicine.mhmedical.com/content.aspx?bookid=1130&Sectionid=79733578. Accessed July 11, 2016.
- Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. American journal of respiratory and critical care medicine. 171(4):388-416. 2005. [pubmed]
- File TM, Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgraduate medicine. 122(2):130-41. 2010. [pubmed]
- Murthy SV. Pathology of Pneumonia. http://www.slideshare.net/vmshashi/pathology-of-pneumonia. Accessed on July 11, 2016.
- Almirall J, Bolíbar I, Balanzó X, González CA. Risk factors for community-acquired pneumonia in adults: a population-based case-control study. The European respiratory journal. 13(2):349-55. 1999. [pubmed]
- Mandell LA, Wunderink RG, Anzueto A. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 44 Suppl 2:S27-72. 2007. [pubmed]
- Musher DM, Thorner AR. Community-acquired pneumonia. The New England journal of medicine. 371(17):1619-28. 2014. [pubmed]
- Jain S, Self WH, Wunderink RG. Community-Acquired Pneumonia Requiring Hospitalization among U.S. Adults. The New England journal of medicine. 373(5):415-27. 2015. [pubmed]
- Metlay JP, Kapoor WN, Fine MJ. Does this patient have community-acquired pneumonia? Diagnosing pneumonia by history and physical examination. JAMA. 278(17):1440-5. 1997. [pubmed]
- Fine MJ, Auble TE, Yealy DM. A prediction rule to identify low-risk patients with community-acquired pneumonia. The New England journal of medicine. 336(4):243-50. 1997. [pubmed]
- Lim WS, van der Eerden MM, Laing R. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 58(5):377-82. 2003. [pubmed]
- Charles PG, Wolfe R, Whitby M. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 47(3):375-84. 2008. [pubmed]
- Pugh R, Grant C, Cooke RP, Dempsey G. Short-course versus prolonged-course antibiotic therapy for hospital-acquired pneumonia in critically ill adults. The Cochrane database of systematic reviews. 2015. [pubmed]

Pingback: Update to Pneumonia Podcast | PAINE Podcast and Medical Blog