
LISTEN TO THE PODCAST HERE
This is actually a special episode for the PAINE Podcast as I have the opportunity to do a joint-interview podcast with Chip Lange from TOTAL EM. This was the first time I got to dabble with a conversational-style podcast and I think it went pretty good. Chip and I had a great time doing it and will most definitely be doing more of these in the future.
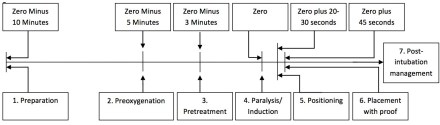
One of the many saying my Army Airborne Ranger dad has instilled in me growing (and one that I still use today) is the seven “P” approach to accomplishing tasks:
Proper
Planning
and
Preparation
Prevents
Piss
Poor
Performance
What is nice about this saying is that it applies very nicely to the steps of intubation as well.
Prepare
You need to to have everything at the bedside you MIGHT need prior to any intubation attempt. This includes equipment, medications, and any personnel or team members who will assist. If you even suspect this could be a difficult airway, you should have your plan B and plan C options in the room to ward off the evil spirits.
- Endotracheal tubes (3 sizes), stylets, bougies, syringes
- Test the balloons on all the tubes
- Laryngoscope
- Multiple blades and handles
- Check the lights
- If using video, plug it in and make sure it turns on
- Patent IV lines x 2
- Suction
- Cardiac and pulse oximetry monitor
- Bag-valve mask
- End-tidal CO2 monitor
- Medications
- Drawn up and labeled
- Concentration read aloud
This also gives you the opportunity to talk with you team about the plan for intubation (how many attempts, progression should plan A, steps of what will happen during the intubation and everyone’s roles during the procedure, etc..), as well as reviewing assisting maneuvers (external laryngeal manipulation, etc.).
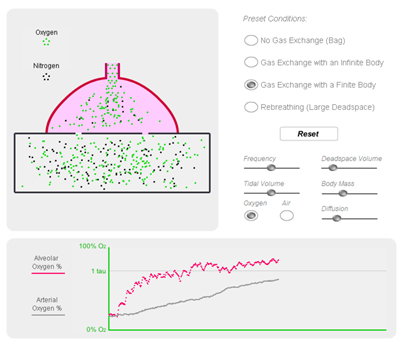
Preoxygenate
In order to decrease any deoxygenation-related issues during the intubation attempt, your patient should recieve 100% oxygen at 15 liters per minute through a non-rebreather mask for 3-5 minutes. This will properly de-nitrogenate and super-saturate all the hemoglobin and give you the time you need to visualize and intubate.
Position
“EAR HOLE TO CHEST HOLE”

For ideal visualization, you want to position your patient so that their external auditory meatus lined up to the sternal notch
Premedicate
There are several different medications you can give for premedication purposes to modify the physiologic response during intubation (lidocaine, opiates, atropine, defasculating agents, etc..), but the main one is the sedative. It is generally poor form to paralyze someone before you sedate them. There are several medications you can choose from for sedation in intubation:
- Ketamine – 1-2mg/kg IV
- My ideal sedative
- Etomidate 0.3mg/kg IV
- Less hemodynamic compromise
- Can cause adrenal suppression
- Propofol – 1.5-3mg/kg IV
- Can cause hemodynamic instability
Paralyze
There are 2 choices for classes of paralytics:
- Depolarizing
- Succinylcholine – 1.5-2mg/kg IV
- Rapid onset, shortest duration of action
- Caution in burn/crush injuries, hyperkalemic patients
- Non-Depolarizing
- Rocuronium – 1.2mg/kg IV
- Vecuronium – 0.3mg/kg IV
Pass The Tube
Once you patient is properly sedative and paralyze, you can proceed to laryngoscopy.
Post-intubation Assessment
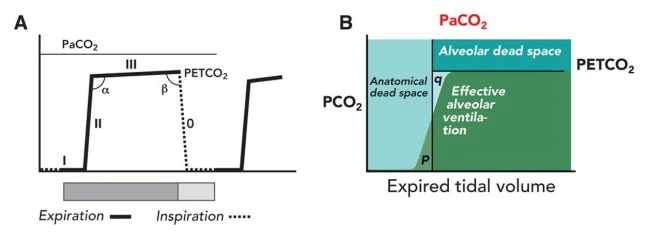
Capnography
This is used for confirmation of correct placement of the endotracheal in the trachea and tests for end-tidal CO2. There are 2 main types:
- Qualitative
- Color change calorimeter
- Attaches to end of endotracheal tube and detects CO2 by changes in exhaled pH

GOLD IS GOOD
- Quantitative
- Continuous Waveform Capnography
- Gold standard
- Gives you a visual waveform to see if the ventilations are adequate
- Continuous Waveform Capnography
Securing the Tube
Once you know you are in the right spot and have been confirmed by capnography, you need to secure the tube. There are different ways to achieve and I often defer to the respiratory therapist or nurse on how they want it secured. There are commercial devices that lock the tube in place and secure using velcro straps, all the way to the old standby of adhesive tape. This is a great site that shows several different ways you can secure the endotracheal tube (http://aam.ucsf.edu/article/securing-endotracheal-tube).

Radiography
Chest xray is the gold standard for the radiographical confirmation of endotracheal placement, as well as ensuring the proper depth. The ideal position for the tube depth should be 3-5cm from the carina or at T3-4 position.
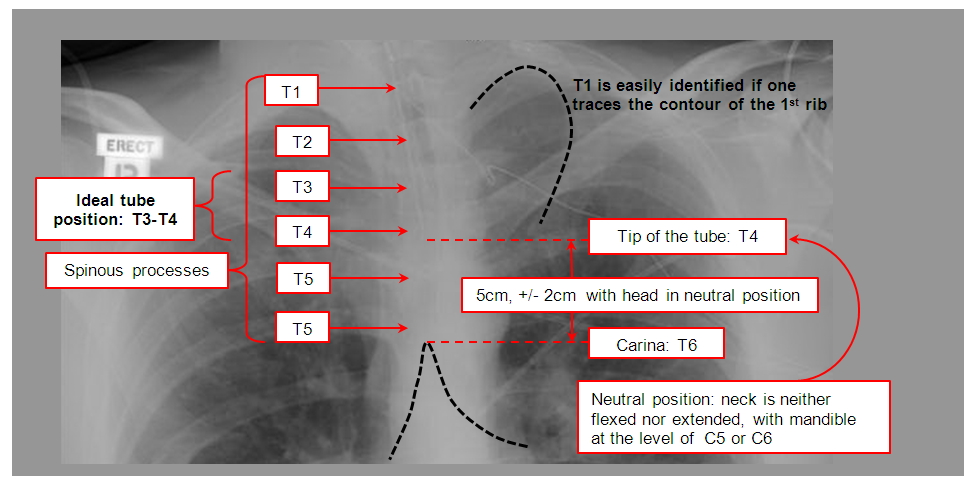
Josh Farkas (PulmCrit) did a great review on endotracheal tube positioning and depth just last week.
Ultrasound is being used more frequently as a confirmatory tool for endotracheal tube placement.
Great review by EmDocs on ultrasound for endotracheal tube confirmation.
Sedation/Analgesia
Now that the tube is in place, secured, and confirmed, you are done right? WRONG!!! Your patient now has a tube shoved into the tracheal and it is a tad uncomfortable. Postintubation sedation/analgesia is PARAMOUNT for good patient care.
- Sedation
- Ketamine – 0.1-0.5mg/kg bolus and 0.1-0.5mg/kg/hr infusion
- Propofol – 5mcg/kg bolus and 5-50mcg/kg/hr infusion
- Midazolam – 0.05mg/kg bolus and 0.025mg/kg/hr infusion
- Analgesia
- Fentanyl – 2mcg/kg bolus and 1mcg/kg/hr infusion
- Hydromorphone – 0.5-1mg/kg bolus and 0.5-3mg/kg/hr infusion
- Morphine – 5-10mg/kg bolus and 2-30mg/hr infusion
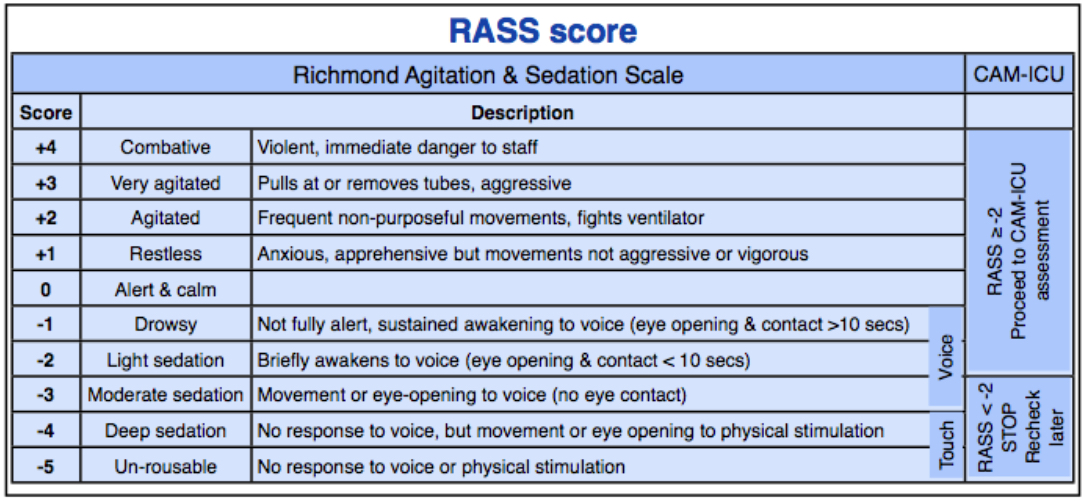
You should be shooting for a Richmond Agitation Sedation Scale (RASS) of -1 to -3 for adequate sedation following intubation.
Really good intubation checklist from Scott Weingart of EmCrit
References
- http://lifeinthefastlane.com/ccc/rapid-sequence-intubation/
- http://emcrit.org/podcasts/emcrit-intubation-checklist/
- Weingart SD, Levitan RM. Preoxygenation and Prevention of Desaturation During Emergency Airway Management. Annals of Emergency Medicine. 2012;59(3):165-175.
- http://www.capnography.com/Emergencydevice/emergencyintubtion.htm
- http://www.capnography.com/new/emergency-intubations
- http://www.capnography.com/new/emergency-intubations?id=216
- http://lifeinthefastlane.com/ccc/capnography-waveform-interpretation/
- http://www.derangedphysiology.com/main/core-topics-intensive-care/mechanical-ventilation-0/Chapter%201.2.3/endotracheal-tube-detail
- http://emcrit.org/podcasts/post-intubation-sedation/
- https://coreem.net/core/post-intubation/

Appreciiate you blogging this
LikeLike