
Question
What are 3 pretest probability scoring systems used to evaluate patients with a suspected pulmonary thromboembolism?
Answer
There are 3 validated pretest probability scoring systems that can be used to help clinicians decide who can be sent home, who needs a D-dimer, and who goes straight to CT for suspected PTE.
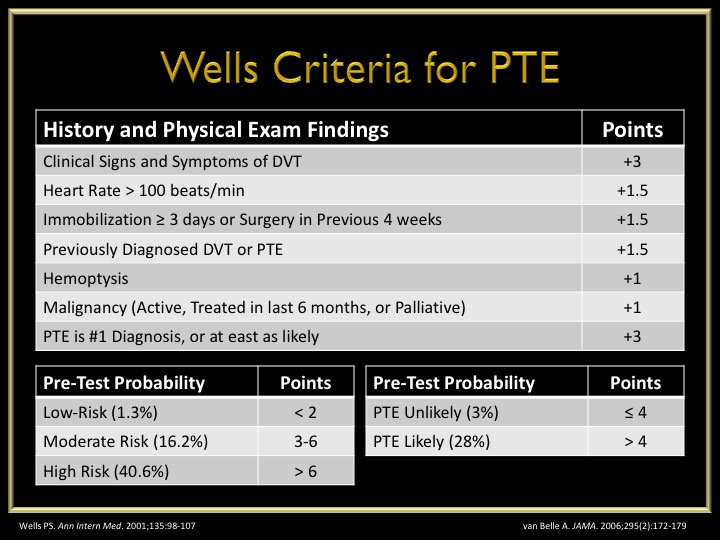
Wells Criteria
Developed – 1998
Revised – 2000
Simplified – 2001
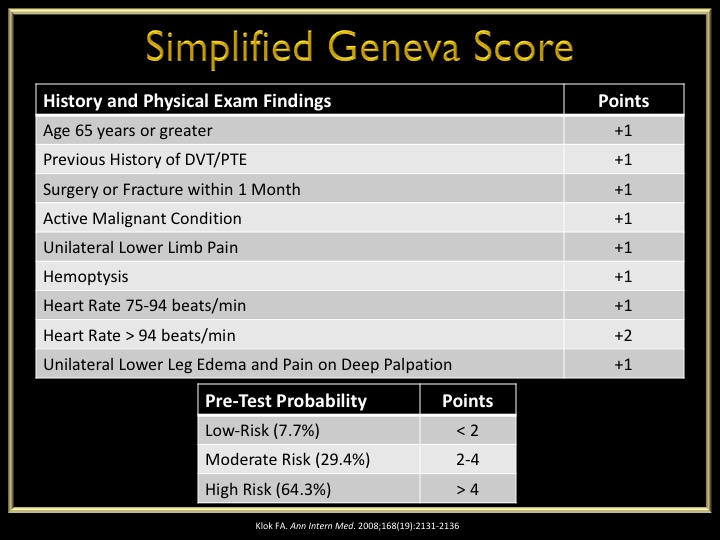
Geneva Score
Developed – 2001
Revised – 2006
Simplified – 2008
Pulmonary Embolism Rule-Out Criteria (PERC) Score
Developed – 2008
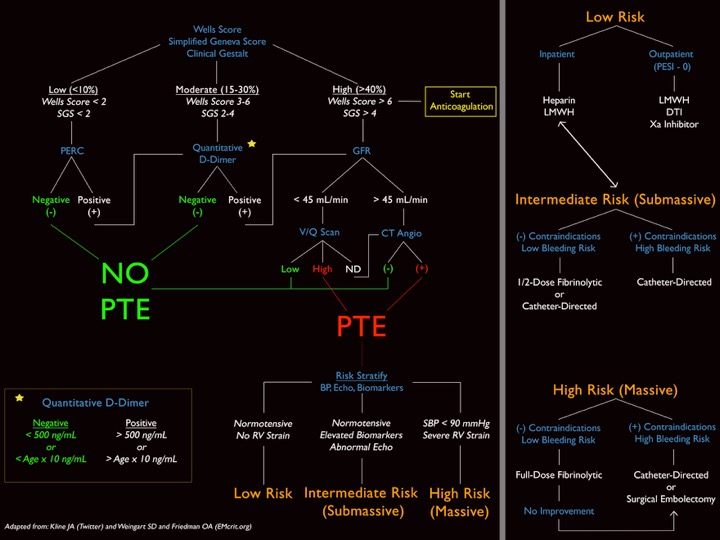
This score is used AFTER the patient is determined to be low-risk using the Well’s or Geneva score. In patients who are low-risk and PERC negative, there is only a 1.6% false-negative rate for missed PTE. Any one of these would deem the patient PERC positive.

Why is this so important?
Although it does help us in deciding who maybe at higher risk of PTE, I personally feel these scoring systems help us document who DOES NOT need work-up. There are quite a few patients who come in with non-specific chest pain or shortness of breath, and you should ALWAYS entertain the idea of PTE in these patients. But, not every single one of these patients need a d-dimer or CTA. Better yet, some of these patients can be discharged home without any investigation if they are low-risk and PERC negative.
Below is an algorithm I modified from Jeff Kline using these clinical decision instruments.
All these images are slides from my talk at the 2015 AAPA Conference
References
-
Wells PS, Ginsberg JS, Anderson DR. Use of a clinical model for safe management of patients with suspected pulmonary embolism. Annals of Internal Medicine. 1998;129(12):997-1005. [pubmed]
-
Wells PS, Anderson DR, Rodger M. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer. Thrombosis and Haemostasis. 2000;83(3):416-20. [pubmed]
-
Wells PS, Anderson DR, Rodger M. Excluding pulmonary embolism at the bedside without diagnostic imaging: management of patients with suspected pulmonary embolism presenting to the emergency department by using a simple clinical model and d-dimer. Annals of Internal Medicine. 2001;135(2):98-107. [pubmed]
-
Wicki J, Perneger TV, Junod AF, Bounameaux H, Perrier A. Assessing clinical probability of pulmonary embolism in the emergency ward: a simple score. Archives of Internal Medicine. 2001;161(1):92-7. [pubmed]
-
Le Gal G, Righini M, Roy PM. Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Annals of Internal Medicine. 2006;144(3):165-71. [pubmed]
-
Klok FA, Mos IC, Nijkeuter M. Simplification of the revised Geneva score for assessing clinical probability of pulmonary embolism. Archives of Internal Medicine. 2008;168(19):2131-6. [pubmed]
-
Kline JA, Courtney DM, Kabrhel C. Prospective multicenter evaluation of the pulmonary embolism rule-out criteria. Journal of Thrombosis and Haemostasis. 2008; 6(5):772-80. [pubmed]
