

***LISTEN TO THE PODCAST HERE***
Epidemiology
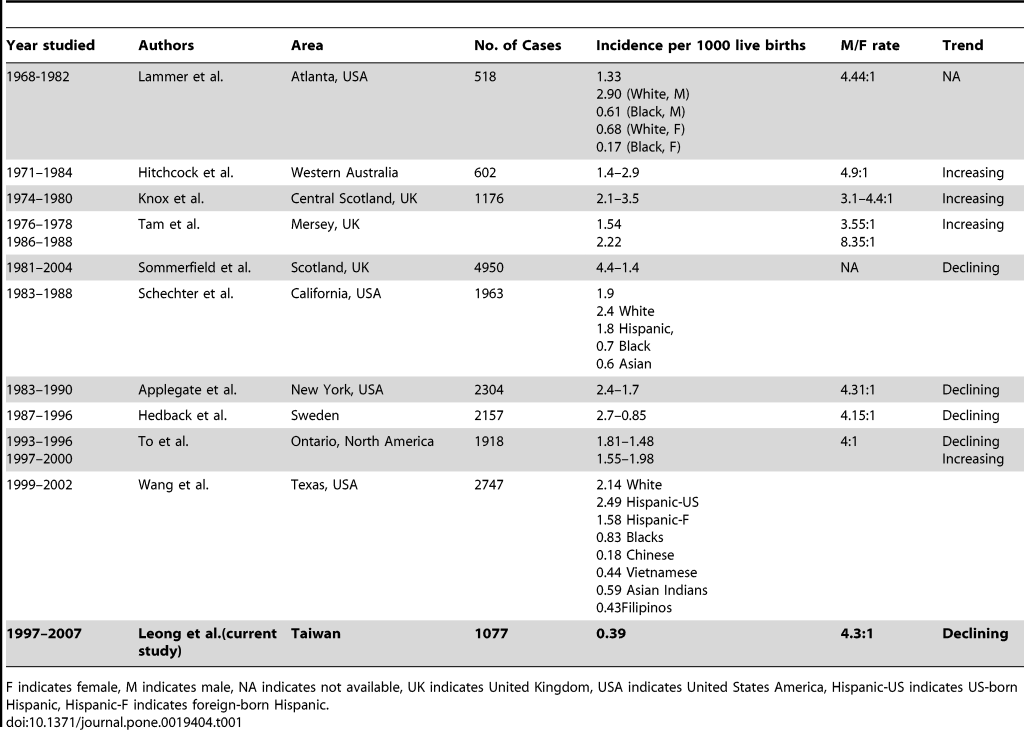
- 2-4 per 1000 live births worldwide and 20 per 10,000 live births in the US
- Higher male to female ratio (4-6:1)
- Higher incidence (1.5x) in first-born children
- Highest incidence in caucasian infants
- Less common in infants of older mothers
Risk Factors and Etiology
The exact mechanisms and etiologies are unclear, but it is hypothesized that it is multifactorial and is a result of both genetic predisposition and environmental triggers.
- Environmental Factors
- Maternal smoking (up to 2x increased risk)
- Bottle feeding
- Bottle feeding during first 4 months increased risk by 4x
- Didn’t delineate formula vs breastmilk
- Bottle feeding during first 4 months increased risk by 4x
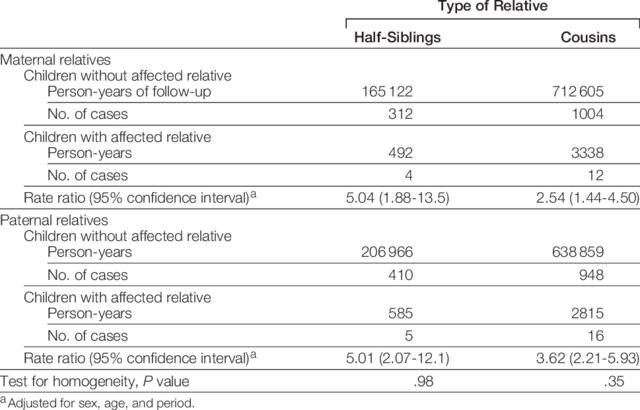
- Genetic Factors
- Reports of familial aggregation, but there is no clear research association
- Apolipoprotein A1 (APOA1) gene cluster
- Hypothesized low plasma cholesterol at birth and increased risk

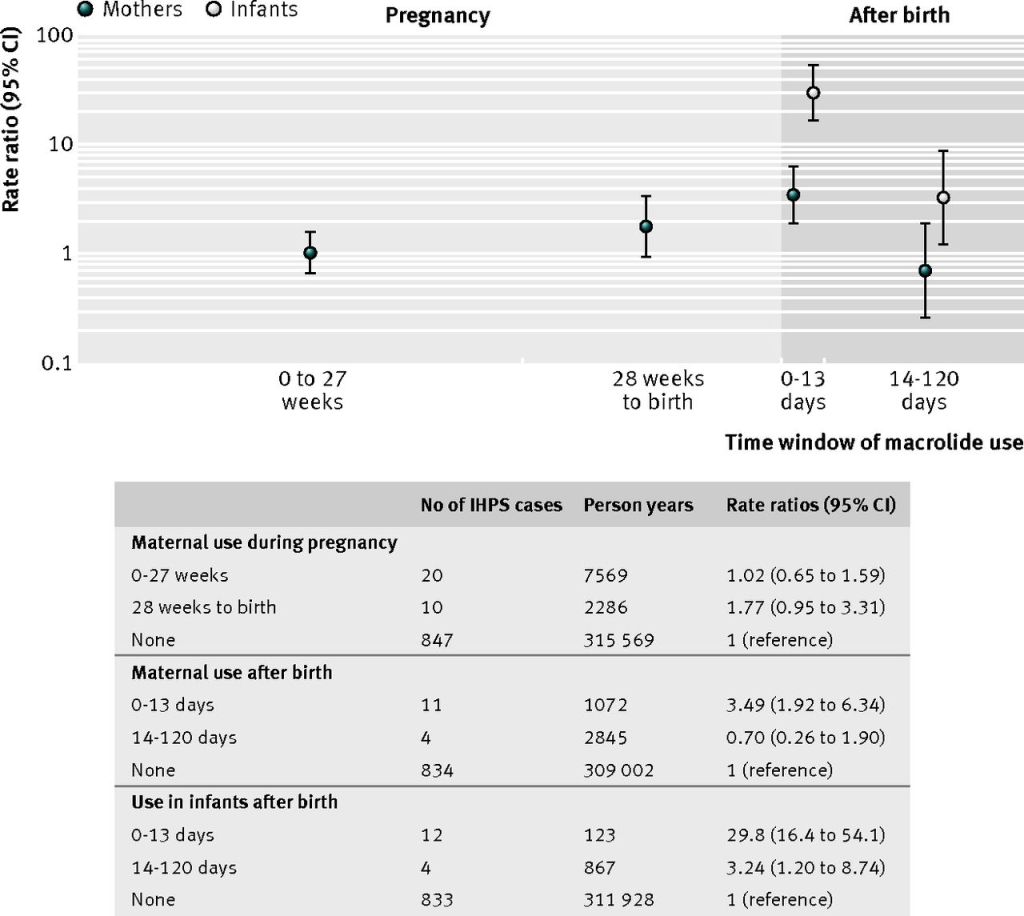
- Macrolide Antibiotics
- Increased risk if given to infants < 2 weeks old
- Treatment/prophylaxis for pertussis
- Association with maternal use during first two weeks of life
- Increased risk if given to infants < 2 weeks old
- Icteropyloric syndrome
- Unconjugated hyperbilirubinemia
- Most commonly from early Gilbert’s Syndrome
- Unconjugated hyperbilirubinemia
History and Physical Examination
- Class presentation for PANCE
- < 6 week old with post-prandial, non-bilious projectile vomiting around 10 minutes after cessation of feeding
- Ravenous feeder even after vomiting
- May be emaciated and/or dehydrated
- Though we are diagnosing earlier and infants tend to be healthier
- Palpable mass in the epigastrium (50-90%)
- This is also less commonly seen due to healthier infants and ease of obtaining radiologic students
- 73% in the 1970s to only 30% now
- Felt as a firm mass at the lateral edge of the rectus abdominis muscle in the RUQ
- Peristaltic waves may also be observed
- Ideally, immediately after vomiting and while the infant is calm
- This is also less commonly seen due to healthier infants and ease of obtaining radiologic students

- Other important assessments
- Height/weight
- Mucous membranes and skin turgor
- Skin and sclerae
- Genitalia
- Ambiguous genitalia raises suspicion for congenital adrenal hyperplasia and adrenal crisis
Diagnostic Studies
- Laboratory
- Hypochloremic metabolic alkalosis
- 88% PPV if pH > 7.45, chloride < 98, and base excess > +3
- Assess for dehydration
- BUN/creatinine > 20:1
- Liver Function Tests
- Bilirubin breakdown, AST/ALT, GGT, and ALP
- Hypochloremic metabolic alkalosis

- Radiography
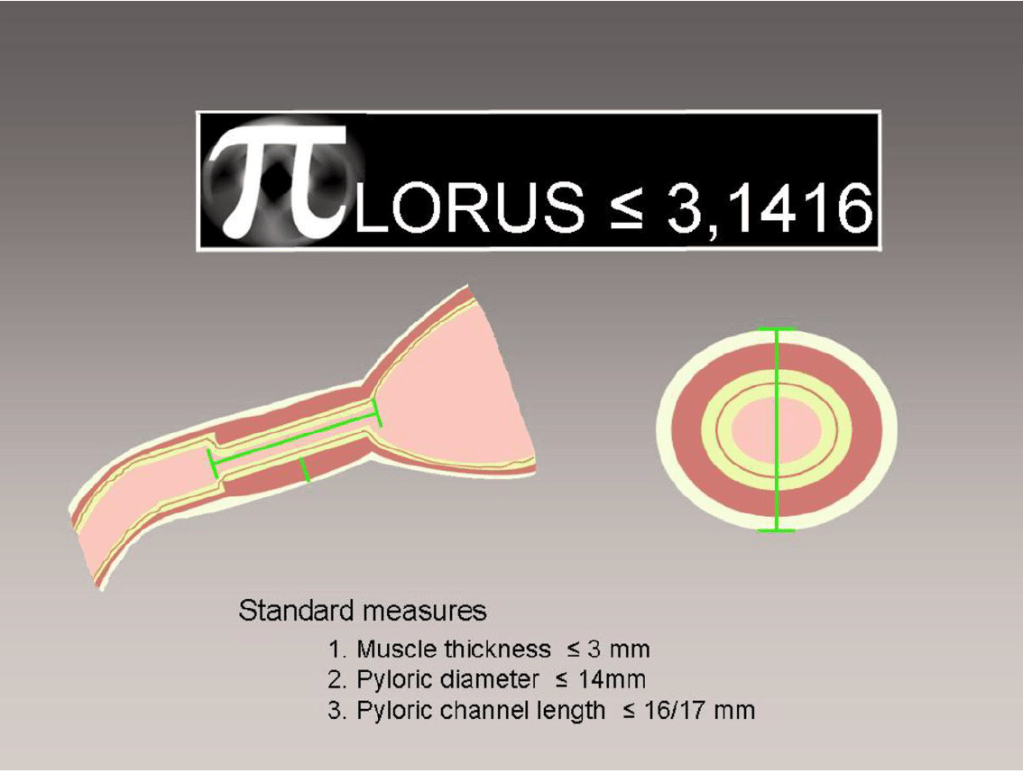
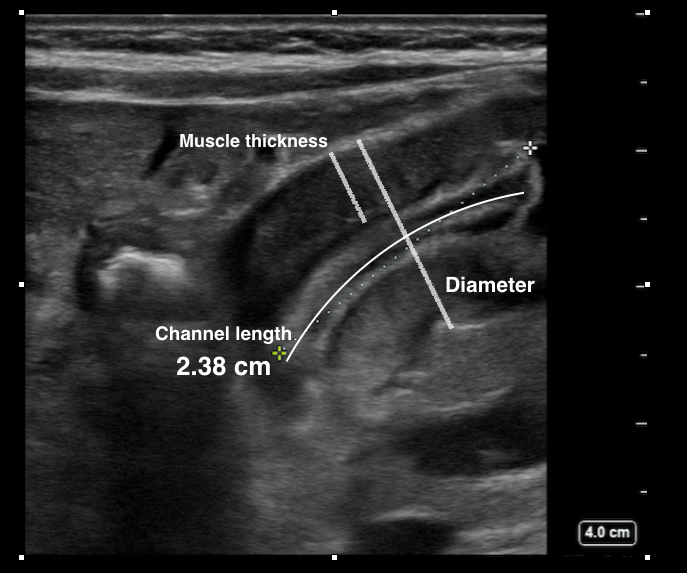
- Ultrasound is the test of choice
- Accuracy is operator dependent, but can reach > 95% sensitivity/specificity
- “Target” sign on transverse view
- Normal Measurements (vary with age and used together)
- Pyloric Muscle Thickness
- < 3mm
- Pyloric Muscle Length
- < 14mm
- Pyloric Channel Length
- < 16mm
- Pyloric Muscle Thickness
- Ultrasound is the test of choice



- Fluoroscopic Upper Gastrointestinal Series
- Used if ultrasound is nondiagnostic
- Classic findings :
- “string” sign from an elongated pyloric canal
- “double-track” sign from two thin tracks of barium along the pyloric canal created by compressed pyloric mucosa
- “beak”sign from a tapered point at the pyloric ending
- “shoulder” sign from a prepyloric bulge of barium

Differential Diagnosis
Although pyloric stenosis has a classic presentation, you must entertain the other important causes of vomiting in infancy.

Treatment
- Definitive management is surgery
- Timing of surgery depends on the clinical status of the infant
- If healthy, surgery can be performed on the day of diagnosis
- If ill, then resuscitation and feeding need to be performed to limit perioperative complications.
- Technique
- Ramstedt Pyloromyotomy
- Longitudinal incision of the pylorus with blunt dissection down to the submucosa
- Ramstedt Pyloromyotomy
- Open vs Laparoscopic
- No difference in operating time, time to full feeding, or length of stay
- Laparoscopic had lower incidence of emesis and better pain control, but higher incidence of incomplete surgical release
- Postoperative Management
- Feeding
- Resumed within a few hours after surgery
- Regurgitation is common, but should not delay/stop feedings
- Breathing
- Monitor for apnea at least for 24 hours
- Complications
- Mucosal perforation (rare)
- Feeding
Follow-Up
- Surgery is curative in the majority of patients
- Once normal feeds occur, only routine pediatric care and follow-up is needed
- Reflux is common and managed conservatively
The Cottage Physician (1893)


References
- Kapoor R, Kancherla V, Cao Y, et al. Prevalence and descriptive epidemiology of infantile hypertrophic pyloric stenosis in the United States: A multistate, population-based retrospective study, 1999-2010. Birth defects research. 2019; 111(3):159-169. [pubmed]
- To T, Wajja A, Wales PW, Langer JC. Population demographic indicators associated with incidence of pyloric stenosis. Archives of pediatrics & adolescent medicine. 2005; 159(6):520-5. [pubmed]
- Krogh C, Fischer TK, Skotte L, et al. Familial aggregation and heritability of pyloric stenosis. JAMA. 2010; 303(23):2393-9. [pubmed]
- Krogh C, Gørtz S, Wohlfahrt J, Biggar RJ, Melbye M, Fischer TK. Pre- and perinatal risk factors for pyloric stenosis and their influence on the male predominance. American journal of epidemiology. 2012; 176(1):24-31. [pubmed]
- Svenningsson A, Svensson T, Akre O, Nordenskjöld A. Maternal and pregnancy characteristics and risk of infantile hypertrophic pyloric stenosis. Journal of pediatric surgery. 2014; 49(8):1226-31. [pubmed]
- Zhu J, Zhu T, Lin Z, Qu Y, Mu D. Perinatal risk factors for infantile hypertrophic pyloric stenosis: A meta-analysis. Journal of pediatric surgery. 2017; 52(9):1389-1397. [pubmed]
- McAteer JP, Ledbetter DJ, Goldin AB. Role of bottle feeding in the etiology of hypertrophic pyloric stenosis. JAMA pediatrics. 2013; 167(12):1143-9. [pubmed]
- Sørensen HT, Nørgård B, Pedersen L, Larsen H, Johnsen SP. Maternal smoking and risk of hypertrophic infantile pyloric stenosis: 10 year population based cohort study. BMJ (Clinical research ed.). 2002; 325(7371):1011-2. [pubmed]
- Feenstra B, Geller F, Carstensen L, et al. Plasma lipids, genetic variants near APOA1, and the risk of infantile hypertrophic pyloric stenosis. JAMA. 2013; 310(7):714-21. [pubmed]
- Eberly MD, Eide MB, Thompson JL, Nylund CM. Azithromycin in early infancy and pyloric stenosis. Pediatrics. 2015; 135(3):483-8. [pubmed]
- Honein MA, Paulozzi LJ, Himelright IM, et al. Infantile hypertrophic pyloric stenosis after pertussis prophylaxis with erythromcyin: a case review and cohort study. Lancet (London, England). ; 354(9196):2101-5. [pubmed]
- Lund M, Pasternak B, Davidsen RB, et al. Use of macrolides in mother and child and risk of infantile hypertrophic pyloric stenosis: nationwide cohort study. BMJ (Clinical research ed.). 2014; 348:g1908. [pubmed]
- Touloukian RJ, Higgins E. The spectrum of serum electrolytes in hypertrophic pyloric stenosis. Journal of pediatric surgery. 1983; 18(4):394-7. [pubmed]
- Bakal U, Sarac M, Aydin M, Tartar T, Kazez A. Recent changes in the features of hypertrophic pyloric stenosis. Pediatrics international : official journal of the Japan Pediatric Society. 2016; 58(5):369-71. [pubmed]
- Sivitz AB, Tejani C, Cohen SG. Evaluation of hypertrophic pyloric stenosis by pediatric emergency physician sonography. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2013; 20(7):646-51. [pubmed]
- Niedzielski J, Kobielski A, Sokal J, Krakós M. Accuracy of sonographic criteria in the decision for surgical treatment in infantile hypertrophic pyloric stenosis. Archives of medical science : AMS. 2011; 7(3):508-11. [pubmed]
- Hernanz-Schulman M. Pyloric stenosis: role of imaging. Pediatric radiology. 2009; 39 Suppl 2:S134-9. [pubmed]
- Said M, Shaul DB, Fujimoto M, Radner G, Sydorak RM, Applebaum H. Ultrasound measurements in hypertrophic pyloric stenosis: don’t let the numbers fool you. The Permanente journal. 2012; 16(3):25-7. [pubmed]
- Iqbal CW, Rivard DC, Mortellaro VE, Sharp SW, St Peter SD. Evaluation of ultrasonographic parameters in the diagnosis of pyloric stenosis relative to patient age and size. Journal of pediatric surgery. 2012; 47(8):1542-7. [pubmed]
- St Peter SD, Holcomb GW, Calkins CM, et al. Open versus laparoscopic pyloromyotomy for pyloric stenosis: a prospective, randomized trial. Annals of surgery. 2006; 244(3):363-70. [pubmed]
- Hall NJ, Pacilli M, Eaton S, et al. Recovery after open versus laparoscopic pyloromyotomy for pyloric stenosis: a double-blind multicentre randomised controlled trial. Lancet (London, England). 2009; 373(9661):390-8. [pubmed]
