These
studies are conducted at the Ottawa Hospital Research Institute and University
of Ottawa starting in 1992 and the main researcher behind these is Ian Stiell.
They
are international recognized and have been validated multiple times to decrease
unnecessary radiographic testing and decrease healthcare costs
Disclaimer for Using Clinical Decision Instruments
Your
clinical judgement should ALWAYS trump using any CDI
Distracting
injuries
Intoxication
Inability
to fully examine
Gestalt
Ottawa Rules of the Foot and Ankle
The
Numbers
Ankle
xrays are the second most commonly ordered film in the ED
<
15% fracture incidence rate
The
study
Published
in 1992, validated in 1995
7
months long
750
patients
21
EM physicians looking at 32 clinical variables
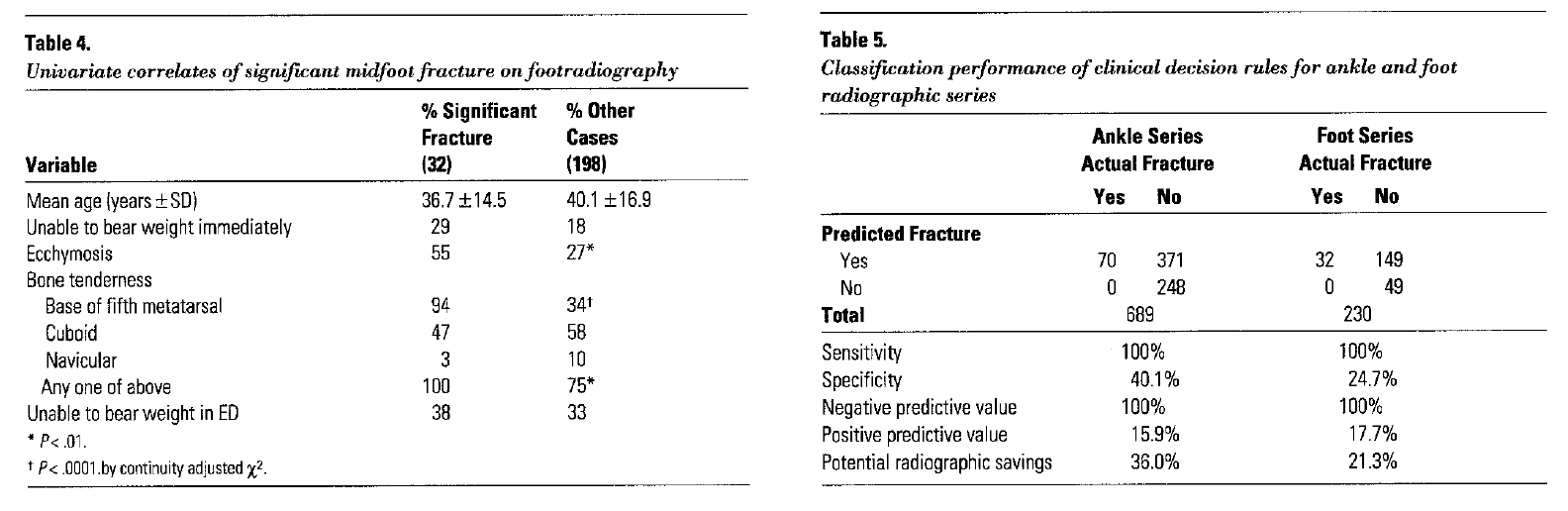
Variables
Lateral
malleolus tenderness
Medial
malleolus tenderness
Base
of 5th metatarsal tenderness
Navicular
tenderness
Inability
to bear weight immediately and in the emergency department for four steps
Limping
counts
Outcomes
Identified
100% of clinically significant fractures
Decreased
ankle imaging 36% and foot imaging 21%
Clinical
Pearls
Be
sure to palpate the entire 6cm of the distal tibia and fibula
Do
not confuse soft tissue tenderness for bony tenderness
Ottawa Rules of the Knee
The
Numbers
>600,000
patients annually present to ED with knee complaints
80%
of these patients have radiography
Majority
have soft tissue injuries
The
study
Published
in 1995, validated in 1996
14
months long
1,047
patients
33
EM physicians looking at 23 clinical variables
Variables
>
55 years of age
Isolated
patella tenderness
Fibular
head tenderness
Inability
to flex knee to 90o
Inability
to bear weight immediately and in the emergency department for four steps
Limping
counts
Outcomes
Identified
100% of clinically significant fractures
Decreased
knee imaging by 28%
Clinical
Pearls
Use
only for injuries < 7 days old
Patella
tenderness only significant if an isolated finding
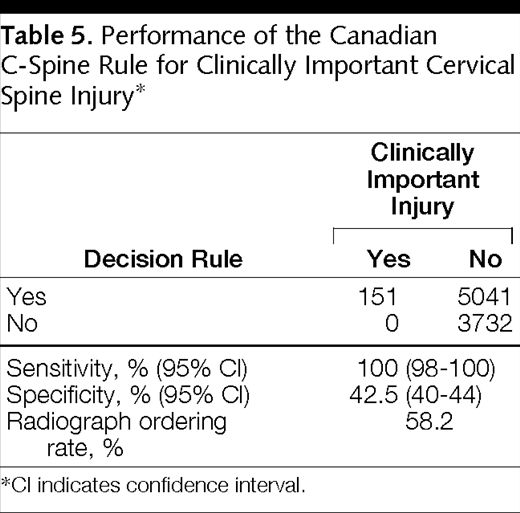
Ottawa Rules of the Cervical Spine
The
Numbers
C-spine
series is the most common radiograph for trauma
>
1,000,000 series performed annually
>
98% being negative
The
study
Published
in 2001, validated in 2003
3
years long
8,924
patients
Blunt
trauma only
Stable
vital signs
GCS
of 15
Looked
at 20 clinical variables
Variables
≥ 65 years of age
Dangerous
mechanism
Fall from height
> 3 feet or 5 stairs
Axial load
High speed (>
60mph) MVC, rollover, or ejection
Motorized
recreational vehicle accident
Pedestrian or
cyclist versus automobile accident
Immediate pain
Non-ambulatory at
scene
Inability to
rotate neck
Outcomes
Identified
100% of clinically significant fractures
Decreased
cervical spine imaging by 42%
Clinical
Pearls
Not
applicable if:
Non-trauma
GCS
< 15
Unstable
vital signs
Age
< 16 years of age
Acute
paralysis
Known
vertebral disease
Previous
cervical spine history
Canadian Head CT Rule
The
Numbers
>
2 million ED visits annually for minor head trauma
Average
cost of CT scan ~ $1200
Average
annual cost > $900 million
<
3% incidence of clinically significant intracranial injuries
The
study
Published
in 2001, validated in 2005
3
years long
3,121
patients
Blunt
trauma only
GCS
between 13-15
<
24 hours on presentations
Must
have loss of consciousness, altered mental status, or amnesia
Across
10 academic hospitals
Looked
at 22 clinical variables
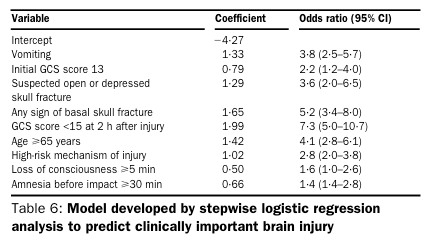
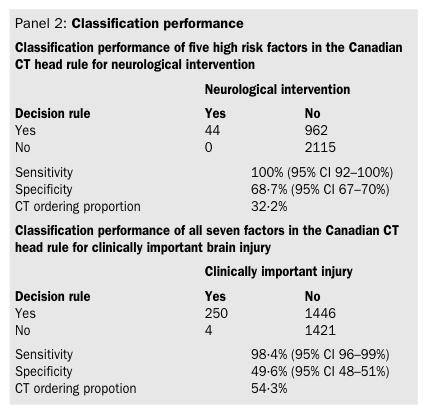
Variables
High risk variables (need for neurosurgical intervention)
GCS < 15 at 2 hour after injury
Suspected open/depressed skull fracture
Signs of basilar skull fracture
≥ 2 episodes of vomiting
≥ 65 years of age
Variables
Medium risk variables (predicting clinically important brain injury)
Retrograde amnesia ≥ 30 minutes
Dangerous mechanism
Pedestrian versus auto
MVC ejection
Fall from height > 3 feet or > 5 stairs
Outcomes
Identified
100% of high risk patients and 98.4% of medium risk patients
Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Worthington JR. A study to develop clinical decision rules for the use of radiography in acute ankle injuries. Annals of emergency medicine. 1992; 21(4):384-90. [pubmed]
Stiell IG, Greenberg GH, McKnight RD, et al. Decision rules for the use of radiography in acute ankle injuries. Refinement and prospective validation. JAMA. 1993; 269(9):1127-32. [pubmed]
Stiell IG, McKnight RD, Greenberg GH, et al. Implementation of the Ottawa ankle rules. JAMA. 1994; 271(11):827-32. [pubmed]
Stiell I, Wells G, Laupacis A, et al. Multicentre trial to introduce the Ottawa ankle rules for use of radiography in acute ankle injuries. Multicentre Ankle Rule Study Group. BMJ (Clinical research ed.). 1995; 311(7005):594-7. [pubmed]
Stiell IG, Greenberg GH, Wells GA, et al. Derivation of a decision rule for the use of radiography in acute knee injuries. Annals of emergency medicine. 1995; 26(4):405-13. [pubmed]
Stiell IG, Greenberg GH, Wells GA, et al. Prospective validation of a decision rule for the use of radiography in acute knee injuries. JAMA. 1996; 275(8):611-5. [pubmed]
Stiell IG, Wells GA, Hoag RH, et al. Implementation of the Ottawa Knee Rule for the use of radiography in acute knee injuries. JAMA. 1997; 278(23):2075-9. [pubmed]
Stiell IG, Wells GA, Vandemheen KL, et al. The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA. 2001; 286(15):1841-8. [pubmed]
Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. The New England journal of medicine. 2003; 349(26):2510-8. [pubmed]
Stiell IG, Wells GA, Vandemheen K, et al. The Canadian CT Head Rule for patients with minor head injury. Lancet (London, England). 2001; 357(9266):1391-6. [pubmed]
Stiell IG, Clement CM, Rowe BH, et al. Comparison of the Canadian CT Head Rule and the New Orleans Criteria in patients with minor head injury. JAMA. 2005; 294(12):1511-8. [pubmed]
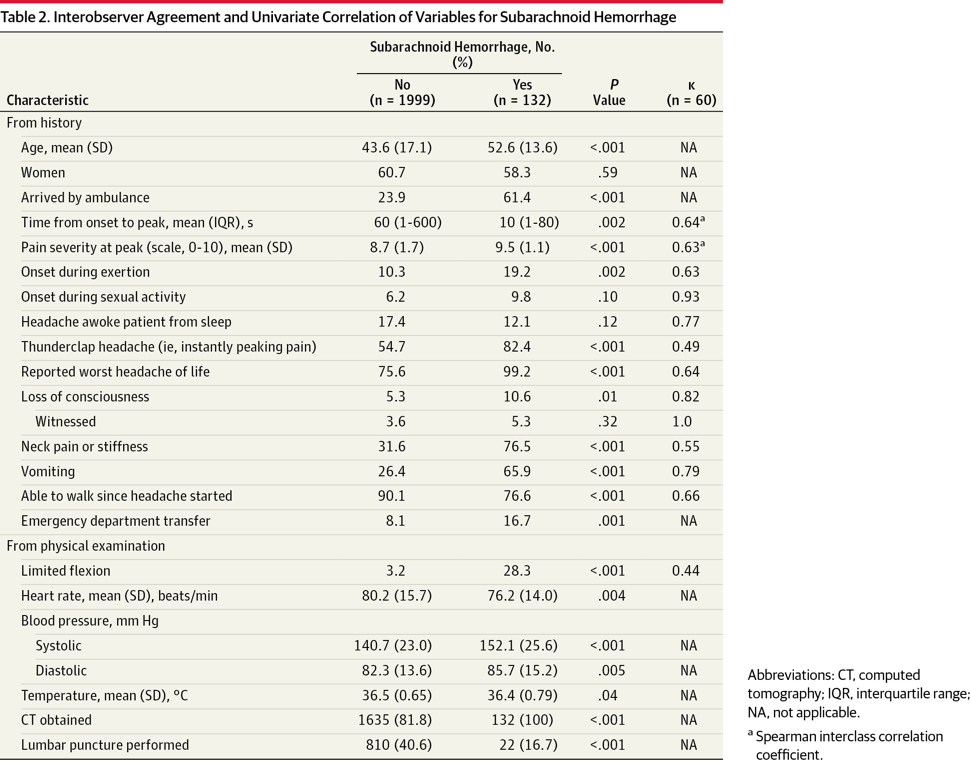
Perry JJ, Stiell IG, Sivilotti ML, et al. High risk clinical characteristics for subarachnoid haemorrhage in patients with acute headache: prospective cohort study. BMJ (Clinical research ed.). 2010; 341:c5204. [pubmed]
Perry JJ, Stiell IG, Sivilotti ML, et al. Clinical decision rules to rule out subarachnoid hemorrhage for acute headache. JAMA. 2013; 310(12):1248-55. [pubmed]






















Pingback: #66 – How to be a Good Student on Emergency Medicine Rotation | PAINE Podcast and Medical Blog