

***LISTEN TO THE PODCAST HERE***
Anatomy
- 4 anatomic areas of gall bladder
- Fundus
- Rounded, blind end that extends 1-2 cm beyond the liver margin
- Contains most of the smooth muscle
- Body
- Main storage area
- Contains the elastic tissue allowing for distention
- Normally holds 30-50mL and can stretch to 300mL
- Infundibulum (Hartmann’s Pouch)
- Mucosal outpouching at the junction of the neck and cystic duct
- Neck
- Lies in the deepest part of the fossa
- Fundus

- Cystic Artery
- Branch of the right hepatic artery
- Found in the cystohepatic triangle
- Cystic duct, common hepatic duct, superior/inferior margin of liver
- Triangle of Calot
- Cystic duct, common hepatic duct, cystic artery
- Lymph node can be found in near the insertion of the cystic artery
- Calot’s node (Lund’s or Mascagni’s)

- Cystic duct
- Spiral valves of Heister
- Mucosal folds in the proximal cystic duct that make cannulation difficult
- Joins the common hepatic duct to form the common bile duct
- Highly variable anatomy
- Spiral valves of Heister
Physiology
- 80% of bile is stored in the gall bladder
- Infundibulum secretes glycoproteins to protect mucosa
- Cholecystokinin released from neuroendocrine cells of the duodenum during meal
- Stimulates release of bile from gallbladder
- 50-70% over 30-40 minutes
- Causes relaxation of Sphincter of Oddi
- Stimulates release of bile from gallbladder
- Vagal stimulation causes contraction of gallbladder
Stone Formation
- Major solutes in bile are bilirubin, bile salts, phospholipids (lecithin), and cholesterol
- 80% are cholesterol
- Supersaturation of bile with cholesterol exceeds the ability of phospholipids and bile salts to maintain solubility
Pathogenesis of Cholecystitis
- Phospholipid A (secreted by the gall bladder mucosa) released in response to gall bladder trauma (stone)
- Catalyzes conversation of lecithin to lysolecithin
- Leads to mucosal and luminal irritation and inflammation
- Catalyzes conversation of lecithin to lysolecithin
Epidemiology and Risk Factors
- 90-95% of patients with cholecystitis have stones
- Only 20% of patients with stones with develop cholecystitis
- 10-15% of patients have stones on autopsy
- Risk Factors
- High fat diet
- Older age
- Female > male
- Higher BMI
- Rapid weight loss
- Pregnancy
- Previous surgeries
- Terminal ileum resection, gastric/duodenal surgery
Signs and Symptoms
- History
- Right upper quadrant abdominal pain
- Steady, “boring” pain lasting hours
- Worsened by fatty foods
- Right scapular pain (Boas’ sign)
- Hyperesthesia between 9th-11th rib
- Fever, nausea, vomiting, anorexia
- Right upper quadrant abdominal pain
- Physical Examination
- Fever, tachycardia
- Peritoneal signs
- Pain with movement and percussion
- Voluntary and involuntary guarding
- +/- jaundice
- Inspiratory arrest on deep RUQ palpation (Murphy’s sign)
Diagnostic Studies
- Laboratory Studies
- Leukocytosis with neutrophilic shift
- LFTs generally normal, but may show:
- Elevated direct (conjugated) bilirubin
- Elevated alkaline phosphatase
- Elevated GGT
- Ultrasound is the initial test of choice
- Length > 10 cm
- Wall thickness > 3mm
- Pericholecystic fluid
- Sludge
- Cholescintigraphy using 99m Tc-hepatic iminodiacetic acid (HIDA) Scan
- Used if ultrasound is inconclusive
- Intravenous injection of HIDA and visualization of dye in gallbladder, bile ducts, and small bowel within 30-60min
- If not visualized after 1 hour, morphine can be given and waiting 3-4 hours
- If no visualization = cholecystitis
- If not visualized after 1 hour, morphine can be given and waiting 3-4 hours
- Magnetic Resonance Cholangiopancreatography (MRCP)
- Used if evidence of choledocolithiasis or elevated LFTs
Management
- Admission
- IV fluids
- NSAIDs
- Ketorolac 30-60mg IV/IM
- Opioids
- Meperidine NOT superior to morphine
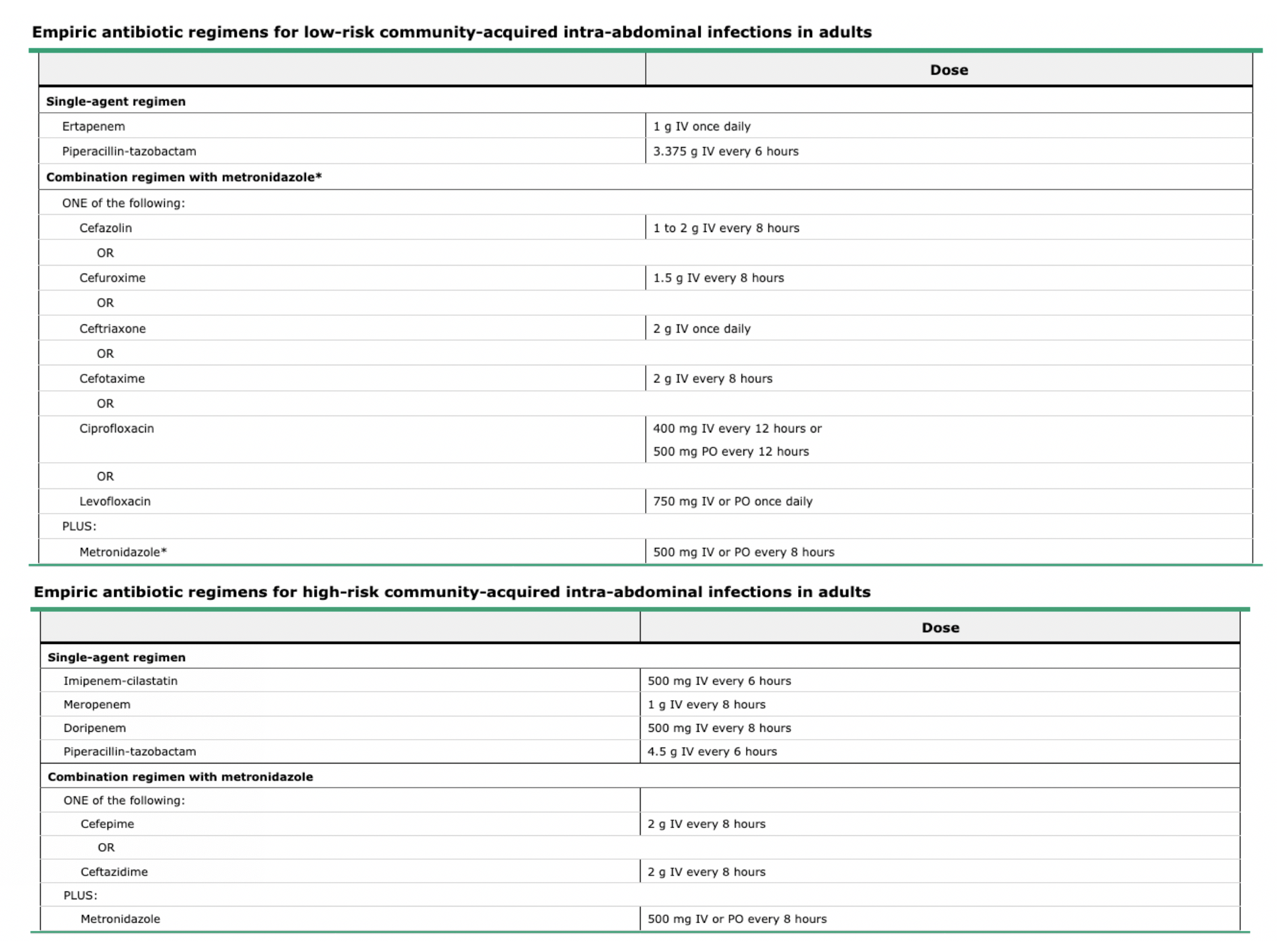
- Antibiotics
- Low Risk
- High Risk
- Indication for Emergent Cholecystectomy
- Necrosis
- Perforation
- Emphysematous cholecystitis
- High fever
- Hemodynamic instability
- Interval Cholecystectomy (low risk)
- Within 3 days of admission after therapies above and clinical improvement
- Most can be discharged in 1-2 days postop
- Gall bladder drainage (high risk)
- Percutaneous cholecystostomy
- Critically ill or septic
- > 72 hours from symptom onset
- Failure of antibiotic therapy
- No coagulopathy
- Endoscopic transpapillary/transmural drainage
- Liver disease
- Ascites
- Coagulopathy
- If improvement within 72 hours, proceed with laparoscopic cholecystectomy
- If not, may need emergent open cholecystectomy
- Percutaneous cholecystostomy
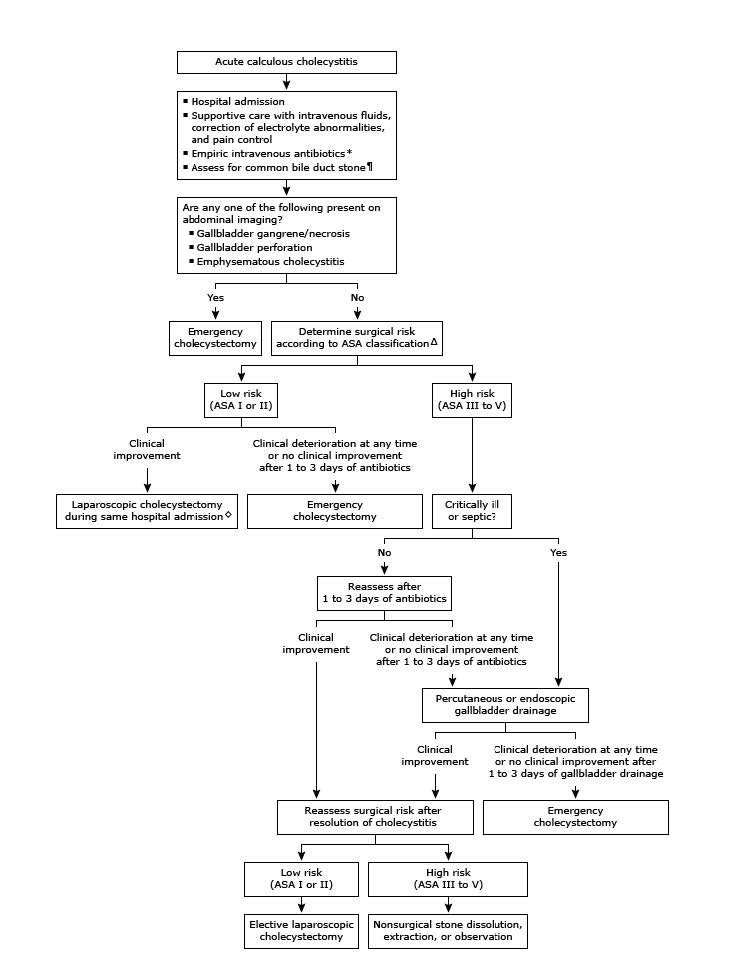
Management Algorithm
Steps of Laparoscopic Cholecystectomy
- Dissect peritoneum overlying the cystic duct and artery
- Division and clipping of cystic duct close to gallbladder
- Perform intraoperative cholangiogram to evaluate CBD
- If clear, then two clips close to common bile duct and ligate
- Dissect cystic artery, one clip close distal and two clips proximal, and ligate
- Dissection of gall bladder from liver bed
- Cauterize, irrigate, suction, and obtain hemostasis of liver bed
- Remove gall bladder

Cottage Physician (1898)

References
- Blackbourne LH. Surgical Recall. 6th Edition. 2012.
- Halpin V. Acute cholecystitis. BMJ Clin Evid. 2014; 2014:. [PDF]
- Haisley KR, Hunter JG. Gallbladder and the Extrahepatic Biliary System. In: Brunicardi F, Andersen DK, Billiar TR, Dunn DL, Kao LS, Hunter JG, Matthews JB, Pollock RE. eds. Schwartz’s Principles of Surgery, 11e. McGraw-Hill; Accessed June 14, 2020. https://accessmedicine-mhmedical-com.ezproxy.uthsc.edu/content.aspx?bookid=2576§ionid=216215815
- Haubrich WS. Calot of the triangle of Calot. Gastroenterology. 2002; 123(5):1440. [pubmed]
- Singer AJ, McCracken G, Henry MC, Thode HC Jr, Cabahug CJ. Correlation among clinical, laboratory, and hepatobiliary scanning findings in patients with suspected acute cholecystitis. Ann Emerg Med. 1996; 28(3):267-72. [pubmed]
- Shea JA, Berlin JA, Escarce JJ, et al. Revised estimates of diagnostic test sensitivity and specificity in suspected biliary tract disease. Arch Intern Med. 1994; 154(22):2573-81. [pubmed]
- Park MS, Yu JS, Kim YH, et al. Acute cholecystitis: comparison of MR cholangiography and US. Radiology. 1998; 209(3):781-5. [pubmed]
- Thompson DR. Narcotic analgesic effects on the sphincter of Oddi: a review of the data and therapeutic implications in treating pancreatitis. Am J Gastroenterol. 2001; 96(4):1266-72. [pubmed]
- Okamoto K, Suzuki K, Takada T, et al. Tokyo Guidelines 2018: flowchart for the management of acute cholecystitis. J Hepatobiliary Pancreat Sci. 2018; 25(1):55-72. [pubmed]
- Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis. 2010; 50(2):133-64. [pubmed]
- Hatzidakis AA, Prassopoulos P, Petinarakis I, et al. Acute cholecystitis in high-risk patients: percutaneous cholecystostomy vs conservative treatment. Eur Radiol. 2002; 12(7):1778-84. [pubmed]
