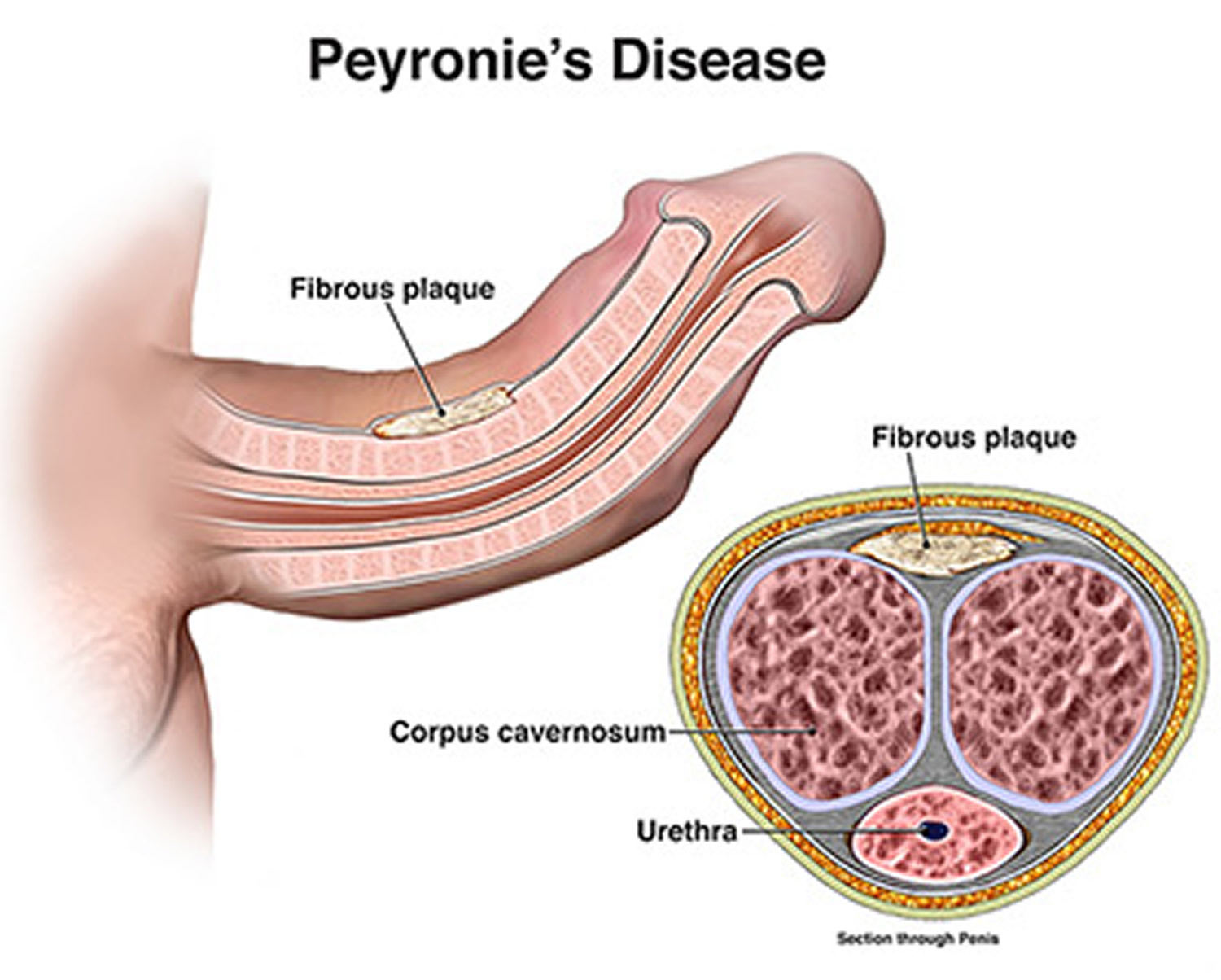
Definition – an acquired, localized fibrotic disorder of the tunica albuginea where thick, fibrous plaques compress the corpora cavernosa
Clinical Significance – The pathogenesis of Peyronie’s disease is unknown and is postulated to be multifactorial. Patients experience pain, penile deformity, and sexual dysfunction
History –Named after François de la Peyronie (1678-1747), who was a French surgeon and received his medical training as a barber-surgeon in Montpellier in 1695. He continued his academic career teaching and practicing surgery and anatomy throughout France. In 1736, he was appointed first-surgeon to King Louis XV and was instrumental in organizing formal training in the surgical arts and was a major force in the creation of the 1743 law that banned barbers from practicing surgery. Also in 1743, he first described the eponymous disease in a book on ejaculation dysfunction where described “indurations of the cavernous bodies like rosary beads” leading to penile curvature. His last name, lapeyronie, means litter stone because his father was a stone cutter. Its a shame he didn’t pursue management of kidney stones as his claim to fame.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
These questions stemmed from an email I got from a former student about electrolyte questions they are getting in the clinical year. These are a quick and basic overview of common electrolyte questions and issues students may see on clinical rotations
#1 – Clinical Repletion of Electrolytes and Monitoring
Not every electrolyte on the chemistry panel needs to be repleted when low…but you need to know which ones can cause problems. The problem children are:
Potassium
Calcium
Magnesium
Phosphorus
Why? These four can all cause cardiac dysrhythmias when low and why all these should be on telemetry, or at least some basic monitoring, when repleting.
Your first step should ALWAYS ALWAYS ALWAYS be to make sure you know why it is low. Yes, we can keep repleting electrolytes to normal levels, but you will be doing this in perpetuity unless you fix the problem causing it in the first place. Let’s review the major points for each:
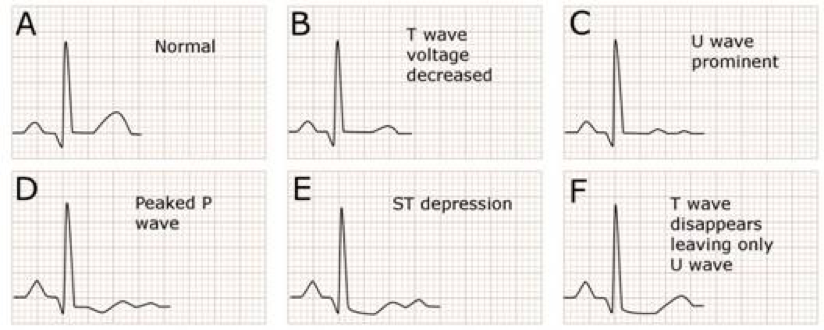
Hypokalemia
Major Cause – Diuretics, GI losses
EKG Changes – Flat T-waves, U-wave. ST-depression
Repletion Pearls
Asymptomatic
Oral replacement – KCl 10-40 mEq 2-4 times per day
Major Causes – Hyperparathyroidism, Refeeding Syndrome, Hungry Bone Syndrome
Major Sequelae – ATP depletion, hemolysis
Repletion Pearls
Asymptomatic
Oral sodium/potassium phosphate 30-80 mmol/day
Symptomatic
IV sodium/potassium phosphate 10-40 mmol/day
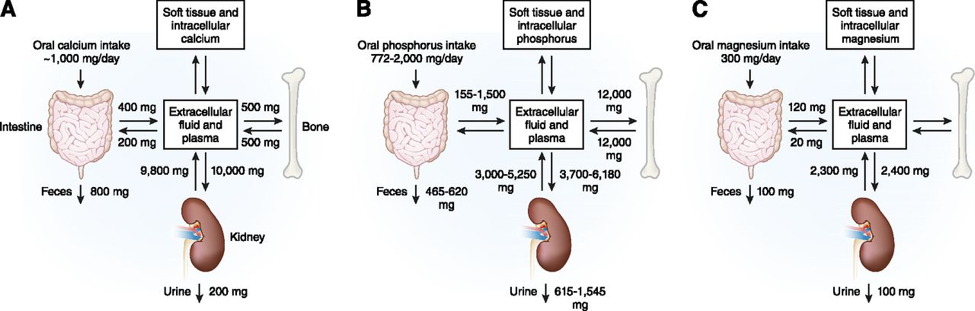
#2 – Calcium/Magnesium/Phosphorus Relationship
You must have a good understanding of this relationship when managing electrolyte deficiencies because you may not be able to make any headway on one if you don’t fix the other.
Magnesium and Calcium/Potassium
Hypomagnesemia causes functional hypoparathyroidism by inducing PTH resistance and decreasing calcium secretion and increasing calcium excretion.
Hypomagnesemia also causes cellular expression of ROMK channels in the nephron which increase potassium excretion
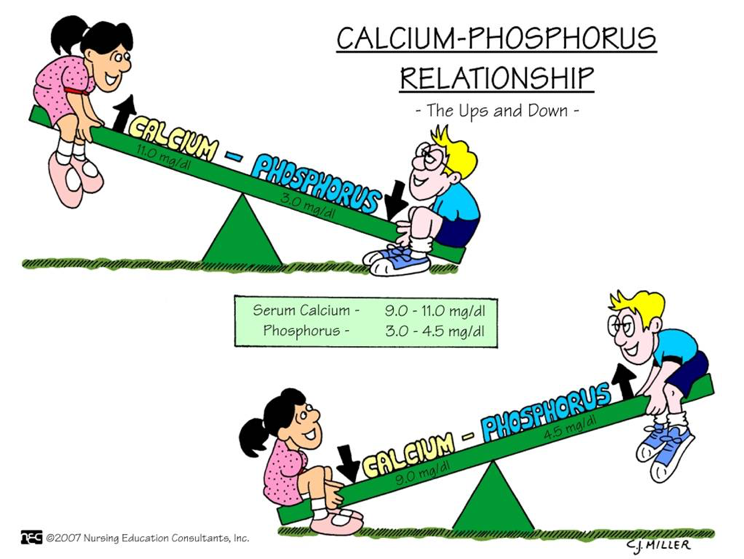
Calcium and Phosphorus
There is an inverse relationship between calcium and phosphorus because of PTH. As PTH increases (seen as a response to hypocalcemia), there is an increase in phosphorus excretion
#4 – Hyponatremia Pearls
Hyponatremia is actually really easy to work up. If you find you patient has a low sodium, check a serum osmolarity, urine osmolarity, and urine sodium.
References
Maday KR. Understanding electrolytes: important diagnostic clues to patient status. JAAPA. 2013; 26(1):26-31. [pubmed]
The prostate begins to enlarge in the 4th decade of life with a significant jump in the 6th decade of life. Mean prostate weight in normal men < 30yo is around 20g and steadily increases after this. Volume of the prostate also steadily increases after the 4th decade with symptoms typically starting to manifest once it reaches 30cc3.
Up-To-Date. 2016
Risk Factors
Race
African Americans are at higher risk of requiring surgery
Asians have the lowest risk of requiring surgery
Prostatitis
Associated with increased risk of BPH
Pathogenesis of BPH
The main areas of the prostate that contribute to BPH are the periurethral (transitional zone) of the prostate and the hyperplastic nodules that develop are primarily comprised of stromal cells. The specific pathogenesis of BPH is still not completely understood and only 2 variables that have been identified as essential for BPH development: age and functioning Leydig Cells of the testes. Androgens, estrogens, inflammation, genetics, and stromal growth factors have all been studied and have variable results.
De Marzo. 2007.
Clinical Manifestations of BPH
The signs of symptoms of BPH can be broken down into 3 main categories:
Storage Symptoms
Urgency
Daytime frequency
Nocturia
Urgency incontinence
Voiding Symptoms
Slow, urinary stream
Splitting or spraying of the urinary stream
Intermittent urinary stream
Urinary hesitancy
Straining to void
Terminal dribbling
Post-micturition Symptoms
Incomplete bladder voiding
Post micturition dribble
Differential Diagnosis of BPH Symptoms
Urethral stricture or bladder neck contracture
Previous history of catheterization or instrumentation
Urethral trauma
Urethritis
Neurogenic bladder
Other signs and symptoms of neurologic disease
Bladder calculi
History of nephrolithiasis
Carcinoma of the bladder or prostate
Hematuria
Previous history of cancer
Urinary tract infection and prostatitis
Dysuria
Fever
Medications
Antcholinergics (decreases bladder function)
Sympathomimetics (increases outflow resistance)
International Prostate Symptom Score
The original AUA score was developed in 1992 and is used to assess the severity of symptoms of BPH, BUT NOT FOR DIFFERENTIAL DIAGNOSIS. This is a seven-part questionnaire that evaluates symptoms on a 0-5 scale and then calculates the symptoms as mild, moderate, or severe. An eight question was added to evaluate quality of life.
International Prostate Symptom Score
Work-Up
Physical Exam
Digital Rectal Exam (DRE) should be performed to assess size, contour, regularity, and nodularity
Laboratory Testing
Urinalysis
Initial test to evaluate for microscopic hematuria and infection
Basic Metabolic Profile
BUN/Creatinine
Evaluate baseline renal function
Serum Prostate Specific Antigen (PSA)
PSA and prostate volume have a log-linear relationship
DOES NOT CORRELATE WITH CANCER
Uroflowmetry Study
Optional testing per AUA
Can evaluate maximal urinary flow rate
Patient voids with a full bladder (> 150cc)
< 15ml/s = outflow obstruction
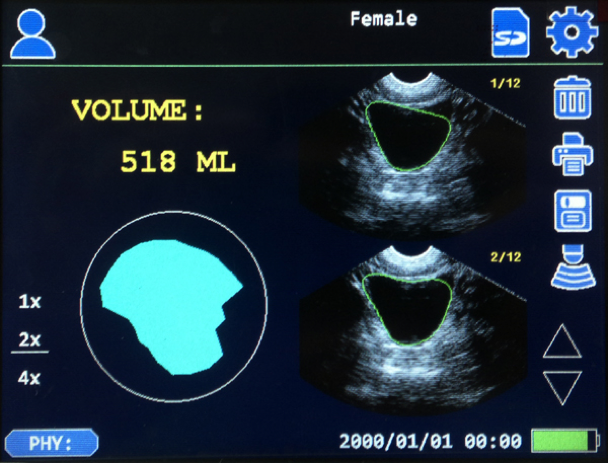
Post-void Residual Urine Volume
Bladder scan is least invasive and most common
Normal men have < 12mL of residual urine post-void
Management
BPH can be managed by PCP if the patient has mild symptoms (low IPSS ≤ 7) and no complications.
Indications for urology referral are:
Symptoms with autonomic or peripheral neuropathy
Symptoms following invasive treatment of the urethra or prostate
Age < 45yo
Abnormality of prostate on DRE
Presence of hematuria in the absence of infection
Incontinence
Severe symptoms (IPSS ≥ 20)
Treatment
Medical
Alpha-1-adrenergic antagonists
Mechanism of Action
Relax smooth muscle of bladder neck, prostate capsule, and prostatic urethra
Side effects
Hypotension
Drugs
Terazosin (need to titrate)
Doxazosin (need to titrate)
Tamsulosin
5-alpha-reductase inhibitors
Used if patients can’t tolerate hypotension of alpha-1-adrenergic antagonists
Need 6-12 months of treatment to see effects
Mechanism of Action
Reduce prostate size by preventing the conversion of testosterone to the more potent dihydrotestosterone
Drugs (no difference due to EPICS trial)
Finasteride
Dutasteride
Combination Alpha-1/5-Alpha Therapy
Indications
Severe symptoms (IPSS ≥ 20)
Large prostate (> 40cc)
Inadequate response to maximal monotherapy
Drugs
Doxazosin/finasteride
Tamsulosin/dutasteride
Surgical
Indications
Moderate/severe symptoms (IPSS ≥ 8) with high quality of life score (≥ 4)
Hyponatremia as a result of the systemic absorption of the hypotonic irrigation solution
Sexual Dysfunction
Ejaculatory Dysfunction
Erectile Dysfunction
Urethral Stricture
Urinary Incontinence
Cottage Physician
References
Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. The Journal of Urology. 1984;132(3):474-9. [pubmed]
Bosch JL, Hop WC, Kirkels WJ, Schröder FH. Natural history of benign prostatic hyperplasia: appropriate case definition and estimation of its prevalence in the community. Urology. 1995;46(3 Suppl A):34-40. [pubmed]
Sidney S, Quesenberry CP, Sadler MC, Guess HA, Lydick EG, Cattolica EV. Incidence of surgically treated benign prostatic hypertrophy and of prostate cancer among blacks and whites in a prepaid health care plan. American Journal of Epidemiology. 1991;134(8):825-9. [pubmed]
Kang D, Andriole GL, Van De Vooren RC. Risk behaviours and benign prostatic hyperplasia. BJU International. 2004;93(9):1241-5. [pubmed]
St Sauver JL, Jacobson DJ, McGree ME, Girman CJ, Lieber MM, Jacobsen SJ. Longitudinal association between prostatitis and development of benign prostatic hyperplasia. Urology. 2008;71(3):475-9; discussion 479. [pubmed]
Rohr HP, Bartsch G. Human benign prostatic hyperplasia: a stromal disease? New perspectives by quantitative morphology. Urology. 1980;16(6):625-33. [pubmed]
De Marzo AM, Platz EA, Sutcliffe S. Inflammation in prostate carcinogenesis. Nature Reviews. Cancer. 2007;7(4):256-69. [pubmed]
Jones C, Hill J, Chapple C, . Management of lower urinary tract symptoms in men: summary of NICE guidance. BMJ (Clinical research ed.). 2010;340:c2354. [pubmed]
Barry MJ, Fowler FJ, O’Leary MP. The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. The Journal of Urology. 1992;148(5):1549-57; discussion 1564. [pubmed]
McVary KT, Roehrborn CG, Avins AL. Update on AUA guideline on the management of benign prostatic hyperplasia. The Journal of Urology. 2011;185(5):1793-803. [pubmed]
Roehrborn CG. The utility of serum prostatic-specific antigen in the management of men with benign prostatic hyperplasia. International Journal of Impotence Research. 2008;20 Suppl 3:S19-26. [pubmed]
Oelke M, Bachmann A, Descazeaud A. EAU guidelines on the treatment and follow-up of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. European Urology. 2013;64(1):118-40. [pubmed]
Chapple CR. Pharmacological therapy of benign prostatic hyperplasia/lower urinary tract symptoms: an overview for the practicing clinician. BJU International. 2004;94(5):738-44. [pubmed]
McVary KT, Roehrborn CG, Avins AL. Update on AUA guideline on the management of benign prostatic hyperplasia. The Journal of Urology. 2011;185(5):1793-803. [pubmed]
Nickel JC, Gilling P, Tammela TL, Morrill B, Wilson TH, Rittmaster RS. Comparison of dutasteride and finasteride for treating benign prostatic hyperplasia: the Enlarged Prostate International Comparator Study (EPICS). BJU International. 2011;108(3):388-94. [pubmed]
McConnell JD, Roehrborn CG, Bautista OM. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. NEJM. 2003;349(25):2387-98. [pubmed]
Roehrborn CG, Siami P, Barkin J. The effects of combination therapy with dutasteride and tamsulosin on clinical outcomes in men with symptomatic benign prostatic hyperplasia: 4-year results from the CombAT study. European Urology. 2010;57(1):123-31. [pubmed]
The Urology Book. urologybook.com. Accessed September 12, 2016.
Gómez Sancha F, Bachmann A, Choi BB, Tabatabaei S, Muir GH. Photoselective vaporization of the prostate (GreenLight PV): lessons learnt after 3500 procedures. Prostate Cancer and Prostatic Diseases. 2007;10(4):316-22. [pubmed]
22yo male presents to emergency department with a 2-hour history of increasingly intense testicular pain. He reports being sexually active with multiple partners and intermittent condom use. He is a very active person and completed a triathlon the day before presentation. He denies dysuria, urethral discharge, or flank pain, but did have an episode of vomiting prior to arrival. He is in visible distress and can not seem to get comfortable. Evaluation of the scrotum reveals a tender, swollen left testicle.
What are some bedside maneuvers you can perform to help with the differential?
Epididymitis
Point tenderness over the superior aspect of the testicle
(+) Prehn Sign
Manual elevation of the testicle improves pain
Testicular Torsion
High-riding and/or horizontal lie of testicle (“Bell Clapper Deformity)
Absent cremesteric reflex
Normal = pinching/stroking the thigh causes ipsilateral elevation of testicle
(-) Prehn Sign
Torsion of Appendix Testes
More common in children
(+) Blue Dot Sign
What should be the initial management of this patient?
If suspected epididymitis:
Urinalysis, urine culture, and gonorrhea/chlamydia testing
Antibiotics are directed towards:
C. trachomatis or N. gonorrhoeae
Ceftriaxone 250mg IM and doxycycline 100mg PO BID x 10 days
Gram-negative enteric pathogens
Levofloxacin 500mg PO daily x 10 days
If suspected testicular torsion:
Manual detorsion may be attempted
2/3 torse medially and detorsion is performed by rotating testicle outwards laterally
Ultrasound may be performed if immediately available (this should not delay surgical consult or evaluation)
Surgical evaluation and management is the preferred initial management of patients with suspected testicular torsion
If suspected torsion of appendix testes:
Ultrasound is performed to rule-out other pathologies.
Management is conservative with rest, ice, and NSAIDs.
Surgical removal may be required if pain does not improve with conservative management.
References
Tracy CR, Steers WD, Costabile R. Diagnosis and management of epididymitis. The Urologic Clinics of North America. 35(1):101-8; vii. 2008. [pubmed]
Galejs LE. Diagnosis and treatment of the acute scrotum. American Family Physician. 59(4):817-24. 1999. [pubmed]
Workowski KA, Bolan GA, . Sexually transmitted diseases treatment guidelines, 2015. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports / Centers for Disease Control. 64(RR-03):1-137. 2015. [pubmed]
Sessions AE, Rabinowitz R, Hulbert WC, Goldstein MM, Mevorach RA. Testicular torsion: direction, degree, duration and disinformation. The Journal of Urology. 169(2):663-5. 2003. [pubmed]
Palestro CJ, Manor EP, Kim CK, Goldsmith SJ. Torsion of a testicular appendage in an adult male. Clinical Nuclear Medicine. 15(7):515-6. 1990. [pubmed]
22yo male presents to emergency department with a 2-hour history of increasingly intense testicular pain. He reports being sexually active with multiple partners and intermittent condom use. He is a very active person and completed a triathlon the day before presentation. He denies dysuria, urethral discharge, or flank pain, but did have an episode of vomiting prior to arrival. He is in visible distress and can not seem to get comfortable. Evaluation of the scrotum reveals a tender, swollen left testicle.
What are some bedside maneuvers you can perform to help with the differential?
What should be the initial management of this patient?