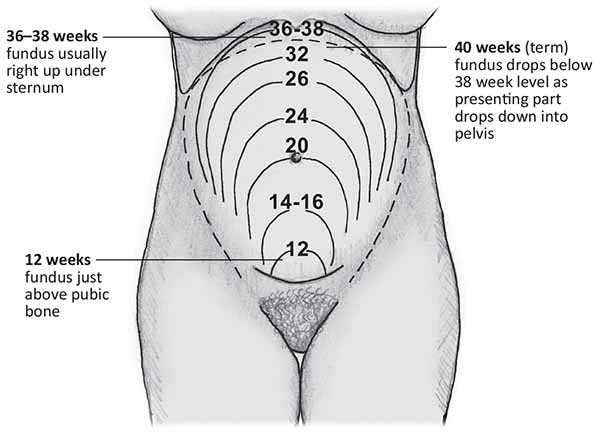
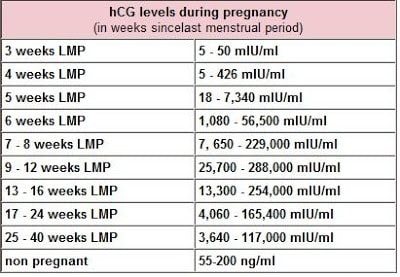
42yo G2P1001, who is 12-weeks gravid, presents to your office with concerns of public pain and a single episode of vaginal bleeding this morning. Physical examination reveals a gravid uterus with fundal height measured at the level of the umbilicus. Serum beta-hCG was found to be 745,223 mIU/mL. Ultrasound is below.
What are the important features of this case?
What is the condition that is present?
What is the next step in management?
Answer
The important features of this case are advanced maternal age (>35y), fundal height commensurate with a 20-week gestation, and a profoundly elevated beta hCG
2. The ultrasound video shows the classic “snow storm appearance” or “bunches of grapes” which is pathognomonic for hydatidiform mole, a type of gestational trophoblastic disease (GTD)
3. Initial management for GTD is methotrexate due to effectiveness, patient tolerance, and cost.
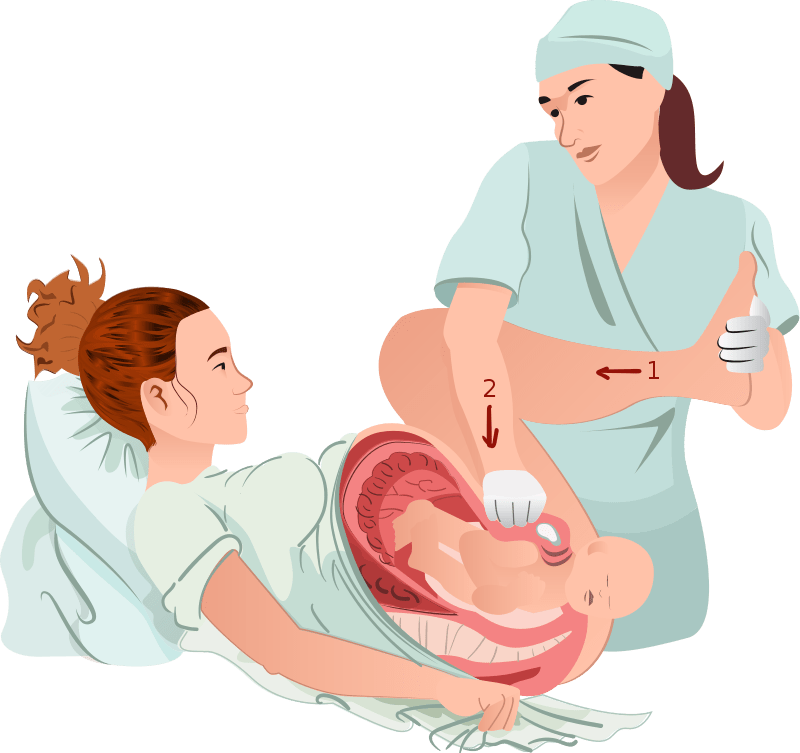
Definition – forced hyperflexion of the hips with applied suprapubic pressure during vaginal delivery
Clinical Significance – this is the primary maneuver to attempt to help relieve a shoulder dystocia during vaginal deliveries. Due to the hypermobilty of sacroilliac joint during pregnancy, this allows for rotation of the pelvis and facilitates releasing the stuck shoulder. It has been shown to have a success of close to 90%.
History – Named after William McRoberts, Jr. (1914-2006), an American obstetrician who recieved his medical doctorate from the University of Pittsburgh in 1940. He would go on to have a modest career in obstetrics culminating in Professor and Chief of Obstetrics at the University of Texas Medical School and Hermann Memorial Hospital in Dallas, TX. It was here where he his reputation as a teacher flourished and where he taught his eponymous maneuver for shoulder dystocia for over 40 years. As a testament to his teaching and a gift on retirement in 1982, two of his residents published an article naming this maneuver after their teacher and mentor.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
42yo G2P1001, who is 12-weeks gravid, presents to your office with concerns of public pain and a single episode of vaginal bleeding this morning. Physical examination reveals a gravid uterus with fundal height measured at the level of the umbilicus. Serum beta-hCG was found to be 745,223 mIU/mL. Ultrasound is below.
Other Known Aliases – cephalic replacement, Gunn-Zavenelli-O’Leary Manuever
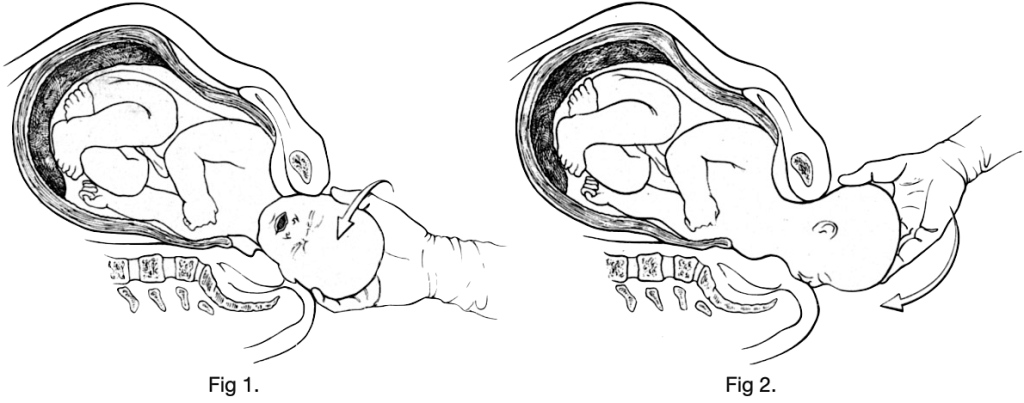
Definition – replacement of the fetal head back into the uterus followed by immediate cesarean delivery
Clinical Significance – this is a controversial, last resort maneuver to a shoulder dystocia and involves rotating the head back to an occiput anterior position, flexing the head , and pushing it as far cephalad as possible. The other hand can be used depress the perineum to relieve pressure on the umbilical cord. Although rarely used, single case reports do show a high rate of success.
History – Named after William Zavanelli (1926- ), an American obstetrician from California who received his medical doctorate from College of Osteopathic Physicians and Surgeons in Los Angeles in 1957. He would go on to have a modest career until 1978 when he performed his eponymous maneuver followed by a successful cesarean delivery. His partner wanted to publish the results immediately, but Zavanelli wanted to wait to see if there were any developmental issues with the child. After seven years, the case report was published. Of note, this manuever was performed 2 years prior by Gunn and his case report was published later in 1985 refuting the eponymous naming.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Sandberg EC. The Zavanelli maneuver: a potentially revolutionary method for the resolution of shoulder dystocia. Am J Obstet Gynecol. 1985;152(4):479-84 [link]
O’Leary J, Gunn D. Cephalic replacement for shoulder dystocia. Am J Obstet Gynecol. 1985; 153(5):592-3. [pubmed]
Special thanks to Morgan Bechtle, PA-S, 2nd year clinical student from the Drexel University PA Program, who did the leg work on this eponym
APGAR Score
Other Known Aliases – none
Definition – medical rating system used to evaluate the condition of a newborn immediately after birth.
Clinical Significance – first presented in 1952, it is a method for evaluating the status of a newborn and it’s response to resuscitation immediately after birth. It consists of five major criteria-heart rate, respiratory rate, muscle tone, reflex response, and color- which are observed and given a score of 0, 1, or 2 points. Today the test is performed at one minute and five minutes after birth. Neonates with a score of 7-10 generally require no further intervention, with lower scores indicating the possible need for assisted respiration.
History – Named after Virginia Apgar (1909-1974), who was a doctor at New York-Presbyterian and the first woman to become a full professor at Columbia University College of Physicians and Surgeons. She spent most of her career studying obstetrical anesthesia and its effect on the newborn. As a young doctor, Apgar was appalled by the treatment of premature, apneic babies. The practice at the time was to list apneic or malformed newborns as stillborn and place them out of sight to die. Outraged by this practice, Dr. Apgar developed a method that would ensure the observation and documentation of the true condition of each newborn during the first minute of life. The Apgar score was first published in 1953 in a paper titled “A Proposal for a New Method of Evaluation of the Newborn Infant” in which she highlighted the need for a “grading system of newborn infants [that can be used] as a basis for discussion and comparison of obstetric practices, types of maternal pain relief, and the effects resuscitation”. Later, her research went on to show that lower Apgar scores are associated with higher neonatal morbidity and mortality.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Other Known Aliases – Polycystic Ovarian Syndrome (PCOS)
Definition – clinical syndrome of hyperandrogenism, oligoanovulation, and polycystic ovaries.
Clinical Significance – PCOS is the most common cause of female infertility and should be investigated in women as part of the infertility workup. Women with PCOS can also have acne, hirsutism, menstrual irregularity, virilization, obesity, insulin-resistance, and metabolic syndrome. It is typically diagnosed in adolescents due to the phenotypic syndromic features.
History – Named after Irving F. Stein, Sr. (1887-1976) and Michael L. Leventhal (1901-1971) and both received their medical doctorates from Rush Medical College in 1912 and 1924 respectively. Both met while practicing at Michael Reese Hospital in early to mid-1900s. They presented a case report of 7 cases of amenorrhea, hirsutism, obesity, and enlarged polycystic ovarias in 1934 at the Central Association of Obstetrics and Gynecologists. They published these findings one year later in 1935 in an article entitled “Amenorrhea associated with bilateral polycystic ovaries” in the Americal Journal of Obstetrics and Gynecology. It should be noted that Russian gynecologist S.K. Lesnoy first described polycystic ovaries in 1928, but not the complete syndrome.
Stein
Leventhal
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
31yo, G0P000, is being evaluated in your clinic for infertility. She and her partner have been trying for 3 years to conceive and have not been successful. She report her partner has already had a semen analysis performed and was within normal limits. She reports a regular menstrual cycle, with little to no variability, and normal flow. She has not been on any form of contraception for 3 years. The rest of her past medical history and family history is benign.
What are types of studies that can be used in her infertility work-up?
Answer
Assessment of Ovulatory Function
Mid-luteal phase serum progesterone typically drawn seven days prior to the start of her menstrual cycle
> 3 ng/mL = recent ovulation
Assessment of Ovarian Reserve
Anti-müllerian hormone (AMH) reflects the size of the follicle pool
Clomiphene citrate challenge test (CCCT)
100mg clomiphene on day 5-9 and measurement of day 3 and day 10 FSH and day 3 estradiol
Assessment of Fallopian Tube Patency
Hysterosalpingogram
Assessment of Uterine Cavity
can be assessed via HSG, but can also be assessed with a saline-infusions sonohysterography or hysteroscopy
Definition – estimation of delivery assuming a 280 day gestation period and is calculated from the FIRST day of the last menstrual cycle by adding 1 year, subtracting 3 months, and adding 7 days.
Clinical Significance – this is a quick and easy estimation of the delivery date for planning purposes and is used in most apps and delivery wheels. In the age of ease of ultrasound, direct measurement is becoming the standard, but this is still a very important calculation to remember.
History – Named after Franz Karl Naegele (1778-1851), who was a German obstetrician and received his medical doctorate from the the University of Bamberg. He had a very successful practice in Barmen, Germany, before he went on to become full professor of obstetrics in 1810 at the University of Heidelberg. He first mentioned his rule, and credited Hermann Boerhaave who first mentioned it in 1744, in a manuscript in 1812, but was given the eponym by Gunning Bedford, professor of obstetrics and diseases of Women and Children at the University of New York, in 1872.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Affects 6-12% of US women ( or 1 in 10) of reproductive age
Increases life-time risk of developing:
Obesity
DMII
Cardiovascular disease
Breast and endometrial cancers
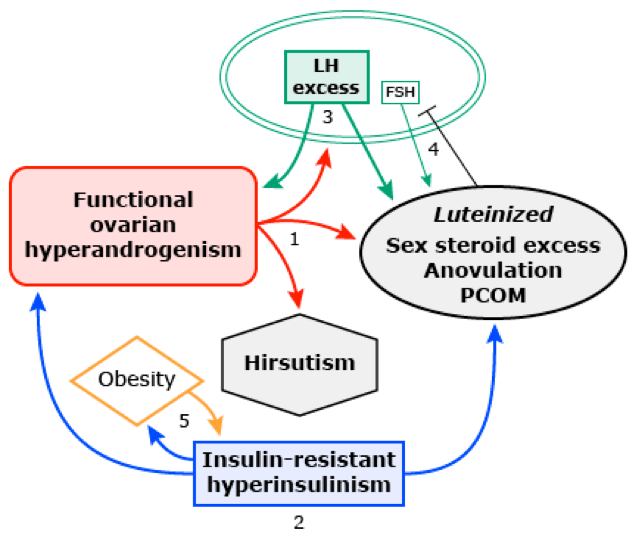
Pathophysiology
Two-Hit Hypothesis
First – genetic predisposition
Heritable traits and gene variations affecting ovarian function, insulin resistance, obesity, and DMII
25% of patients with PCOS have a mother with PCOS
Congenital virilization
Congenital adrenal hyperplasia
Disturbed fetal nutrition
Second – provocative trigger
Insulin-resistant hyperinsulinemia
Puberty
This then leads to the classic pathology of:
Functional ovarian hyperandrogenism
Hyperinsulinism and obesity
Luteinizing hormone (LH) excess
Up-to-Date
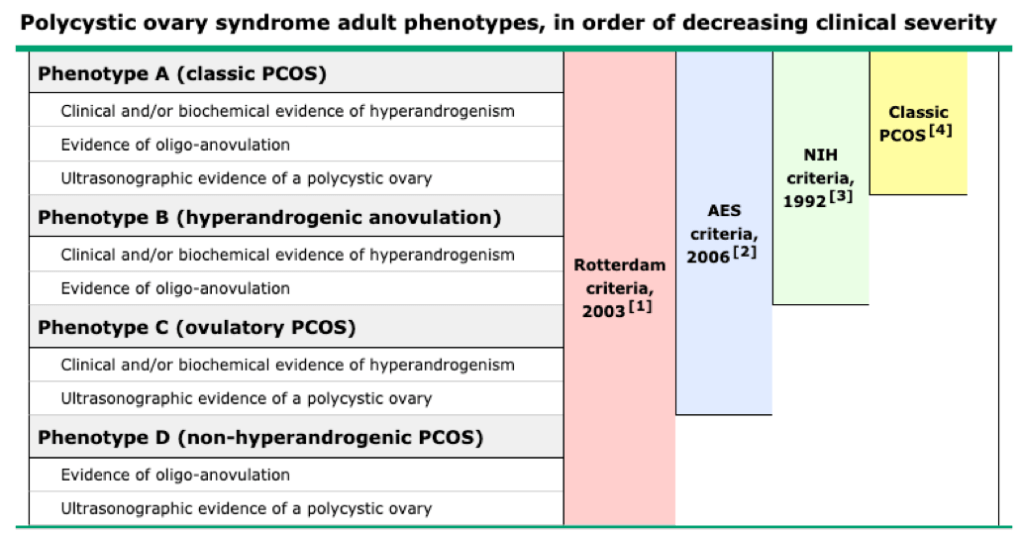
Definition and Diagnostic Criteria
Adults
Rotterdam Criteria
2 of 3 following criteria:
Anovulation
Hyperandrogenism
Polycystic ovaries
Up-to-Date
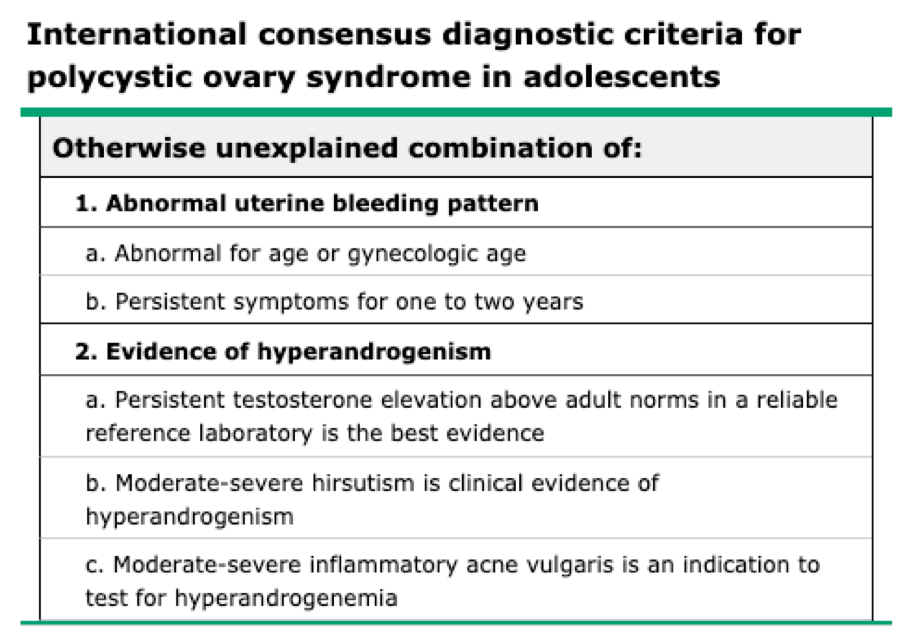
Adolescents
Developed in 2015 and consist of otherwise unexplained persistent hyperandrogenic oligo-anovulatory menstrual abnormality based on age and stage appropriate standards
Up-to-Date
Clinical Features
Cutaneous Hyperandrogenism
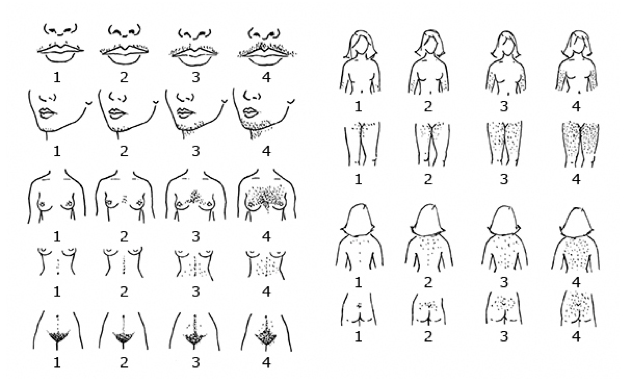
Hirsutism
Graded by Ferriman-Gallwey scoring system, which quantitates the extent of hair growth in androgen sensitive areas
Hirsutism is defined as a score ≥ 8
Acne
Moderate comedonal acne or severe inflammatory acne suggests hyperandrogenemia
Ovarian Findings
Menstrual
Primary Amenorrhea
Lack of menarch by 15 years of age or > 3 years after onset of breast development
Secondary Amenorrhea
> 90 days without a menstrual cycle after previously menstruating
Oligomenorrhea
During the first five years after menarache:
Year 1 – < 4 cycles in the year
Year 2 – < 6 cycles in the year
Year 3-5 – < 8 cycles in the year
Missing ≥ 4 cycles in the year
Year 6+ – < 9 cycles in the year
Missing ≥ 3 ycles in the year
Excessive uterine bleeding
More frequently than every 21 days or excessive bleeding
PCOS is the most common cause of excessive uterine bleeding in adolescents
Polycystic ovaries
Obesity
Chief complaint in up to 20% of PCOS patients
Sleep apnea or
Nonalcoholic fatty liver
Manifestations of insulin resistance
Acanthosis nigricans
Metabolic syndrome
Up to 25% of PCOS patient
Diagnostic Work-Up
Need to be performed at a lab with highly sensitive assay capability
If using hormonal OCP, need to be stopped 2-3 months before testing
Due to suppression of testosterone
Testosterone (1st step)
Should be early morning as testosterone levels fall by the afternoon
Serum total testosterone
Normal – 40-60 ng/dL
> 150 ng/dL is diagnostic
Serum free testosterone
More sensitive than total, but are less standardized
Only reliable if calculated from the total testosterone
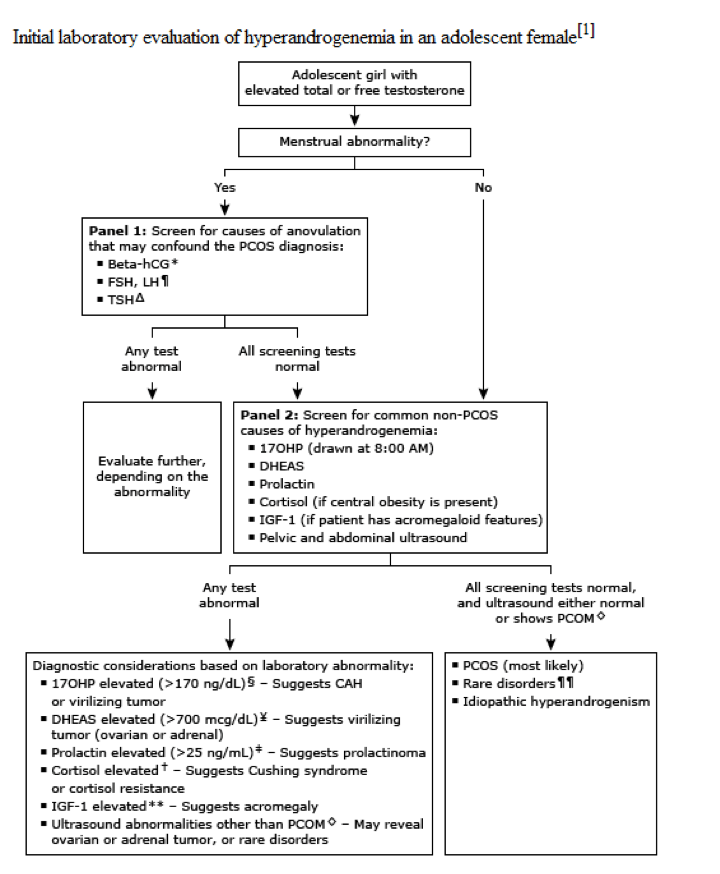
Endocrine Screening Panel (2nd step if elevated testosterone)
Beta-hCG
FSH/LH
Slightly elevated LH with a slightly decreased FSH is characteristic of PCOS
Markedly elevated FSH = primary hypogonadism
Markedly decreased LH = secondary hypogonadism
TSH
Screening for Common non-PCOS causes of hyperandrogenism (3rd step if endocrine screening is normal)
17-hydroxyprogesterone (17OHP)
Drawn at 0800 and with the patient either amenorrheic or within the fist 10 days after the start of her menstrual cycle
> 170 ng/dL suggests CAH
DHEAS
> 700 mcg/dL suggests adrenal tumor
Prolactin
Hyperprolactinemia can causes gonadotropin deficiency
> 25 ng/m: suggests prolactinoma
Serum cortisol
< 10 mcg/dL rules out Cushing syndrome
Insulin-like grown factor (IGF-1)
Rule out acromegaly
Other tests
Chronic disease panel
CBC, ESR/CRP, CMP
Lipid Panel (for adults)
LDL, HDL, triglycerides
Transvaginal ultrasound of ovaries
Increased overall size
Increased number of distinct follicles
≥ 6 is diagnostic
Treatment
Adolescents
Antiandrogen
Estrogen-progestin combination OCPs
Can also use GnRH agonist (leuprolide)
Targeted antiandrogen therapy (if no improvement after 6 months)
Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, Yildiz BO. The prevalence and features of the polycystic ovary syndrome in an unselected population. The Journal of clinical endocrinology and metabolism. 2004; 89(6):2745-9. [pubmed]
Franks S, Stark J, Hardy K. Follicle dynamics and anovulation in polycystic ovary syndrome. Human reproduction update. ; 14(4):367-78. [pubmed]
Barthelmess EK, Naz RK. Polycystic ovary syndrome: current status and future perspective. Frontiers in bioscience (Elite edition). 2014; 6:104-19. [pubmed]
Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertility and sterility. 2004; 81(1):19-25. [pubmed]
Azziz R, Carmina E, Dewailly D, et al. The Androgen Excess and PCOS Society criteria for the polycystic ovary syndrome: the complete task force report. Fertility and sterility. 2009; 91(2):456-88. [pubmed]
Rosenfield RL. The Diagnosis of Polycystic Ovary Syndrome in Adolescents. Pediatrics. 2015; 136(6):1154-65. [pubmed]
Witchel SF, Oberfield S, Rosenfield RL, et al. The Diagnosis of Polycystic Ovary Syndrome during Adolescence. Hormone research in paediatrics. 2015; [pubmed]
Martin KA, Anderson RR, Chang RJ, et al. Evaluation and Treatment of Hirsutism in Premenopausal Women: An Endocrine Society Clinical Practice Guideline. The Journal of clinical endocrinology and metabolism. 2018; 103(4):1233-1257. [pubmed]
Maslyanskaya S, Talib HJ, Northridge JL, Jacobs AM, Coble C, Coupey SM. Polycystic Ovary Syndrome: An Under-recognized Cause of Abnormal Uterine Bleeding in Adolescents Admitted to a Children’s Hospital. Journal of pediatric and adolescent gynecology. 2017; 30(3):349-355. [pubmed]
Helvaci N, Karabulut E, Demir AU, Yildiz BO. Polycystic ovary syndrome and the risk of obstructive sleep apnea: a meta-analysis and review of the literature. Endocrine connections. 2017; 6(7):437-445. [pubmed]
Elhassan YS, Idkowiak J, Smith K, et al. Causes, Patterns, and Severity of Androgen Excess in 1205 Consecutively Recruited Women. The Journal of clinical endocrinology and metabolism. 2018; 103(3):1214-1223. [pubmed]
Pau CT, Keefe C, Duran J, Welt CK. Metformin improves glucose effectiveness, not insulin sensitivity: predicting treatment response in women with polycystic ovary syndrome in an open-label, interventional study. The Journal of clinical endocrinology and metabolism. 2014; 99(5):1870-8. [pubmed]
31yo, G0P000, is being evaluated in your clinic for infertility. She and her partner have been trying for 3 years to conceive and have not been successful. She report her partner has already had a semen analysis performed and was within normal limits. She reports a regular menstrual cycle, with little to no variability, and normal flow. She has not been on any form of contraception for 3 years. The rest of her past medical history and family history is benign.
What are types of studies that can be used in her infertility work-up?