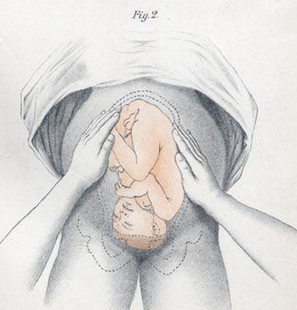
Definition – Series of four distinct actions to systematically determine the lie and position of the fetus in utero:
First Maneuver – Fundal Grip
used to locate fetal position (breech vs vertex)
Second Maneuver – Umbilical Grip
used to locate the back of the fetus
Third Maneuver – Second Pelvic Grip
used to determine pelvic inlet position
Fourth Maneuver – First Pelvic Grip
used to locate the fetal brow
Clinical Significance – These are now an antiquated way to determine fetal positioning to predict difficult deliveries or need for cesarean section. These have largely been replaced by obstetrical ultrasound.
History – Named after Christian Gerhard Leopold (1846-1911), who was a German gynecologist and received his medical doctorate from the University of Leipzig in 1870. He spent the early part of his career teaching midwifery at the Frauenklinik in Leipiz before taking a professorship at the University of Leipzig in 1883. Later that same year, he took over as the Director of the Dresden Royal Gynaecological Infirmary and by the end of his tenure developed it into a leading hospital in Germany. He published his eponymous maneuvers in several articles (first in 1894) in the journal Archiv für Gynäkologie, for which he was a co-editor.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
You have just assisted with a relatively uneventful spontaneous vaginal delivery of a 38-week newborn to a 29-year-old G1P0001 mother. During your immediate, postpartum maternal assessment, you notice a large amount of vaginal bleeding persisting.
Questions
What is the most common cause of this condition?
What are the two most important steps in managing this?
What are some of the other etiologies to think about?
Other Known Aliases – round ligament of the uterus, ligamentum teres uteri
Definition – These are the lateral attachments of the uterus that originate at the uterine horns and extend out immediately below and in front of the fallopian tubes. They also cross the external lliac vessels before entering the inguinal canal.
Clinical Significance – This ligament maintains uterine anteversion during pregnancy and can cause pain as they stretch
History –Named after William Hunter (1718-1783), who was a Scottish anatomist and obstetrician, and was the younger brother of John Hunter (an even more famous anatomist). He studied extensively on anatomy, with particular interests in obstetrical anatomy, and was also appointed as the chief physician to Queen Charlotte in 1764. His namesake ligaments come from his posthumously published textbook An Anatomical Description of the Human Gravid Uterus in 1794.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
32yo, G2P2002, who presents to your practice for her annual well-woman examination. She has recently moved and is establishing care. She can’t recall the last time she had a pap smear performed, but is “pretty sure” it was more than 3 years ago. She does not smoke, has no significant FH for GYN malignancies (cervical/ovarian/breast), and is otherwise healthy. Pap smear performed in the office was cytology negative, but HPV positive.
Answer
For women ≥ 30 years of age with a cytology (-), but HPV (+) pap, you really have two options depending on your access to testing:
Definition – Small fluid-filled sac in the ovary containing a maturing egg that develops after the first meiotic division has completed but before ovulation.
Clinical Significance – This follicle secretes estrogen and inhibin to aid in ovulation and promote implantation should fertilization occur by negatively feeding back to the pituitary to decrease LH and FSH.
History –Named after Regnier de Graaf (1641-1673), who was a Dutch physician and anatomist who made tremendous advancements in reproductive anatomy and physiology long before the invention of the microscope. He published his findings in 1668 and 1672, which was received with controversy by some of his contemporaries since several before him noticed these follicles but failed to recognize their significance in reproduction. The term Graafian follicle was given to him Albrecht von Haller who called it the ova Graafiana.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
32yo, G2P2002, who presents to your practice for her annual well-woman examination. She has recently moved and is establishing care. She can’t recall the last time she had a pap smear performed, but is “pretty sure” it was more than 3 years ago. She does not smoke, has no significant FH for GYN malignancies (cervical/ovarian/breast), and is otherwise healthy. Pap smear performed in the office was cytology negative, but HPV positive.
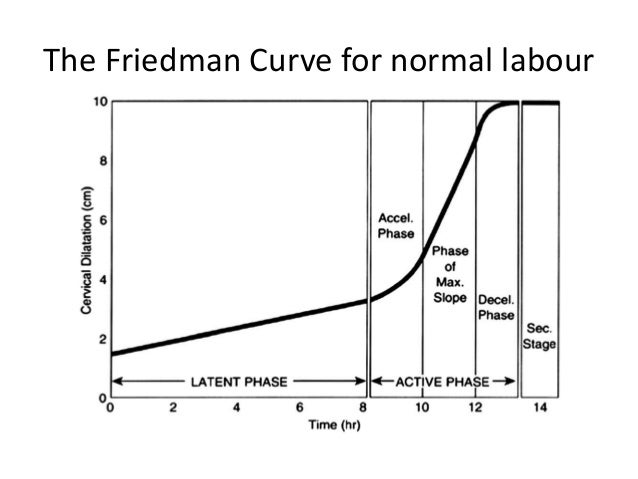
Definition – graphical representation of an “ideal” labor course based on cervical dilation measurements and progression from the latent and active phase of stage 1 labor to the onset of stage 2 labor
Clinical Significance – This was the first scientific and statistical representation of the progression of labor and allowed obstetricians to better assess laboring mothers.
History –Named after Emmanuel Friedman (1926-), who is an American obstetrician and received his medical doctorate from Columbia University’s College of Physician and Surgeons in 1951 after being drafted into the Navy during World War II. His seminal paper published in 1954 entitled “The Graphical Analysis of Labor” was born from disappointment and frustration by not being allowed to leave his call post when his wife went into labor with their first child at another hospital. Although it has been replaced by ACOG in 2016 as a reliable method for labor standards, it still stands a tremendous advancement in obstetrical medicine.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
The 1st trimester of pregnancy is from conception to week 12 gestation. It is important to note that most women do not even think about the possibility of pregnancy until 2-3 weeks post-conception and is typically after a week as passed without the initiation of a menstrual cycle. This can become even more difficult if a woman has baseline irregular menses, or the fact that early pregnancy bleeding is can occur in up to 10% of women.
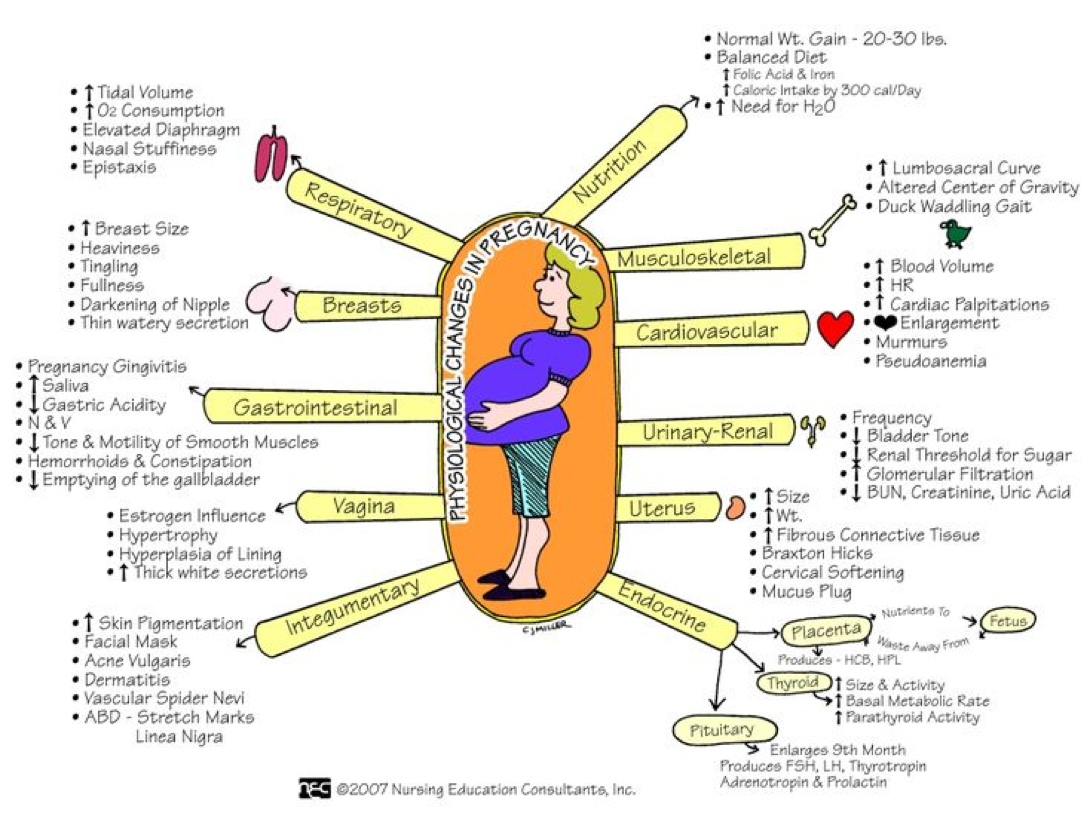
Physiological Changes of Pregnancy in 1st Trimester
Cardiovascular
Systemic vasodilation
Increased plasma volume > change in RBC mass
Increased resting heart rate
Pulmonary
Elevation of diaphragm
Decreased functional residual capacity
Increased ventilation and respiratory drive
Gastrointestinal
Hypomotility of bowel and gastroparesis
Renal
GFR increases
BUN/Cr decreases
Signs and Symptoms of Early Pregnancy
60% of women may experience these symptoms within 6 weeks of conception and 90% will experience by 8 weeks:
Amenorrhea
Nausea and vomiting
Breast enlargement and tenderness
Increased frequency of urination without dysuria
Fatigue
Abdominal bloating
Shortness of breath
Lightheadedness
Back pain
Physical Examination
The uterus remains a pelvic organ until around 12 weeks gestation
Cervix may soften (Goodell’s sign) and have a bluish color from vascular congestion (Chadwick’s sign)
Breast become fuller, tender, and hyperpigmentation of the areola may occur
Fetal cardiac activity can be picked up by transvaginal ultrasound as early as 6 weeks, but fetal heart tones won’t be heard until 10-12 weeks by handheld doppler
Diagnosis of Pregnancy
There are 2 ways to diagnosis pregnancy:
Laboratory
Detection of human chorionic gonadotropin (hCG)
Urine (threshold – 20-50 milli-IU/mL)
Can be detected as early as 2 weeks from fertilization
Blood (threshold – 2-10 millil-IU/mL)
Significantly more sensitive than urine and can be positive with a negative urine test
Radiographically by ultrasound
Gestational sac or intrauterine fluid collection may be visible at 4-5 weeks gestation
Yolk sac appears at 5-6 weeks gestation and remains until 10 weeks
Fetal pole with cardiac activity can be detected at 5-6 weeks (if transvaginal, closer to 6-7 weeks if transabdominal)
Errors in Laboratory Testing
False Negatives
Testing too soon after conception
Hook effect
Extremely high hCG and not diluted by lab
False Positive
Biochemical pregnancy
Early fetal loss with elevated circulating hCG
hCG from trophoblastic disease
Goals of Prenatal Care
The initial visit should occur in the 1st trimester (ideally by 10 weeks), but only 60-75% of women achieve this.
Clinical/Provider
Early, accurate estimation of gestational age
Identification of high risk mothers
Ongoing evaluation of maternal and fetal health status
Meah VL, Cockcroft JR, Backx K, Shave R, Stöhr EJ. Cardiac output and related haemodynamics during pregnancy: a series of meta-analyses. Heart. 2016; 102(7):518-26. [pubmed]
Harville EW, Wilcox AJ, Baird DD, Weinberg CR. Vaginal bleeding in very early pregnancy. Human reproduction (Oxford, England). 2003; 18(9):1944-7. [pubmed]
Foxcroft KF, Callaway LK, Byrne NM, Webster J. Development and validation of a pregnancy symptoms inventory. BMC pregnancy and childbirth. 2013; 13:3. [pubmed]
Lohstroh P, Dong H, Chen J, Gee N, Xu X, Lasley B. Daily immunoactive and bioactive human chorionic gonadotropin profiles in periimplantation urine samples. Biology of reproduction. 2006; 75(1):24-33. [pubmed]
Furtado LV, Lehman CM, Thompson C, Grenache DG. Should the qualitative serum pregnancy test be considered obsolete? American journal of clinical pathology. 2012; 137(2):194-202. [pubmed]
Downe S, Finlayson K, Tunçalp Ӧ, Metin Gülmezoglu A. What matters to women: a systematic scoping review to identify the processes and outcomes of antenatal care provision that are important to healthy pregnant women. BJOG. 2016; 123(4):529-39. [pubmed]
ACOG Committee Opinion No. 343: psychosocial risk factors: perinatal screening and intervention. Obstetrics and gynecology. 2006; 108(2):469-77. [pubmed]
ACOG Practice Bulletin No. 88, December 2007. Invasive prenatal testing for aneuploidy. Obstetrics and gynecology. 2007; 110(6):1459-67. [pubmed]
ACOG Practice Bulletin No. 77: screening for fetal chromosomal abnormalities. Obstetrics and gynecology. 2007; 109(1):217-27. [pubmed]
Deutchman M, Tubay AT, Turok D. First trimester bleeding. American family physician. 2009; 79(11):985-94. [pubmed]
Martonffy AI, Rindfleisch K, Lozeau AM, Potter B. First trimester complications. Primary care. 2012; 39(1):71-82. [pubmed]
Doubilet PM, Benson CB, Bourne T. Diagnostic criteria for nonviable pregnancy early in the first trimester. NEJM. 2013; 369(15):1443-51. [pubmed]
ACOG. Practice Bulletin No. 175: Ultrasound in Pregnancy. Obstetrics and gynecology. 2016; 128(6):e241-e256. [pubmed]
What the anatomic landmarks for estimation of gestational age based on fundal height measurements?
Answer
Measuring fundal height is a skill PA students must acquire on their OBGYN rotation. Using a rolled tape measure, the distance is measured (in cm) from the pubic symphasis to the highest part of the uterus. Note that it may not be mid-line and you will need to do some palpation to find the apex.
Anatomic landmarks can help estimate gestational age based on fundal height measurements:
12 weeks – just above the pubic symphasis
16 weeks – halfway between pubic symphasis and umbilicus
20 weeks – at the level of the umbilicus
After 20 weeks, gestational age is estimated at 1 cm per week…..that is to say 25 weeks gestational should have a fundal height measurement of 25 cm (+/- 2 cm).
Definition – Blue-red passive hyperemia of cervix that may appear after the 6th week of pregnancy
Clinical Significance – This is one of the earliest physical exam findings of pregnancy and is a result of increased uterine blood flow to support the newly implanted embryo.
History – Named after James Reed Chadwick (1844-1905), who was an American gynecologist and received his medical doctorate from Harvard in 1871. He published in 1887 describing this finding, but gave due credit of the initial discovery to Étienne Joseph Jacquemin (1796-1872) who first noted it 1836.
He also help found the American Gynaecological Society and Boston Medical Library, and is also well known as being a noted librarian and scholar. He was also a fervent advocate of women in the practice medicine and published extensively in support of this endeavor.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Chadwick JR. The value of the bluish discoloration of the vaginal entrance as a sign of pregnancy. Transactions of the American Gynecological Society. 1877;11:399–418.
Gleichert JE. Etienne Joseph Jacquemin, discoverer of ‘Chadwick’s sign’. Journal of the history of medicine and allied sciences. 1971; 26(1):75-80. [pubmed]
Chadwick JR. The Study and Practice of Medicine by Women. 1879. [Link]
Chadwick JR. Admission of Women to the Massachusetts Medical Society. 1882. [Link]