Question
This one is a quick one this week. When evaluating a patient with testicular pain (either acute or chronic), what are the specific physical examination techniques you can perform and what conditions do they help rule in/out?


Question
This one is a quick one this week. When evaluating a patient with testicular pain (either acute or chronic), what are the specific physical examination techniques you can perform and what conditions do they help rule in/out?

Fournier’s Gangrene
Other Known Aliases – none
Definition – necrotizing fasciitis of the external genitalia and/or perineum
Clinical Significance – this infection commonly affects older men and is associated with diabetes mellitus or a compromised immune system. Other risk factors include trauma or surgery to the perineal area, alcoholism, and childbirth. Pain, erythema, crepitus, and fever are common findings and treatment is aggressive surgical debridement and antibiotics to cover anaerobic and facultative pathogens.
History – Named after Jean Alfred Fournier (1832-1914), who was a French dermatologist and venereologist, and received his medical doctorate in 1860 while studying in Paris. He would begin his career as an understudy of Philippe Ricord at the Hôpital du Midi and would later become médecine des hôpitaux at the famed Hôtel-Dieu de Paris. It was in 1883 when he presented a case series of patients with gangrene of perineum and for which this eponym is attributed, although it was first described and published in 1764 by Baurienne. He is best known for his work with congenital syphilis (for which he has two additional eponyms) and advancing the study of venereal diseases and their connection to degenerative diseases.
References
Question
49yo woman, with a history of hypertension and GERD, presents to your clinic with a six month history of bilateral shoulder weakness that she first noticed when putting on sweaters and jackets and carrying in groceries. She denies any history of pain, repetitive trauma, or weakness in the hands. On physical examination, she has 3.5/5 strength in shoulder abduction and flexion, as well as the below rash. She reports the rash has been present for about the same time, but doesn’t really bother her.


Answer
Kienböck Disease
Other Known Aliases – none
Definition – avascular necrosis of the lunate

Clinical Significance – most often results from trauma with biomechanical and vascular abnormalities that lead to progressive bone death. Patients will report wrist pain with decreased range of motion and grip strength. MRI is best for early diagnosis and treatment depends on the stage of disease using the Lichtman Classification system.

History – Named after Robert Kienböck (1871-1953), who was an Austrian radiologist and received his medical doctorate from the University of Vienna in 1895. He would explore the new and blossoming field of radiology before becoming the head of the radiological department at Vienna General Hospital before becoming professor of radiology in 1926. He was a pioneer in the use of x-rays for medical diagnosis and would co-found the Vienna Radiology Society in 1923. He would publish his eponymous condition in 1910 in his treatise Über traumatische Malazie des Mondbeins und ihre Folgezustände (Traumatic malacia of the lunate and its consequences).

References
***LISTEN TO THE PODCAST HERE***

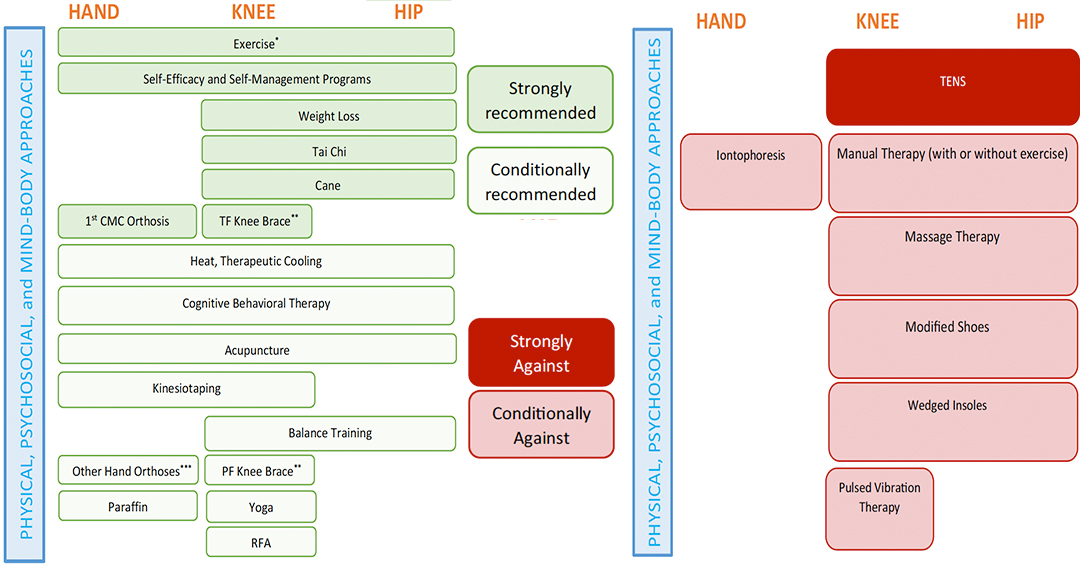
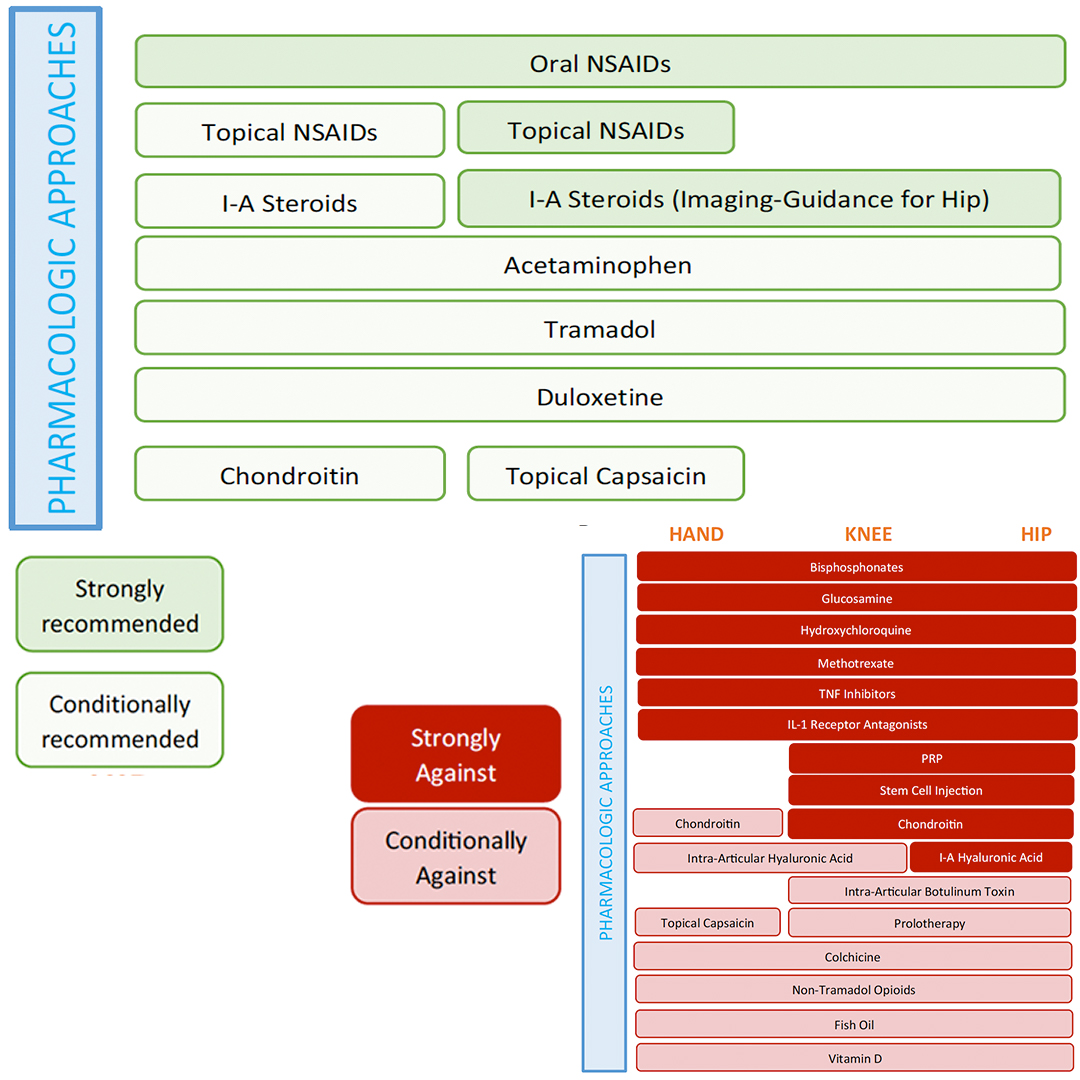
2019 updated guidelines from American College of Rheumatology and American Arthritis Foundation
Question
43yo woman, with a history of hypertension and GERD, presents to your clinic with a six month history of bilateral shoulder weakness that she first noticed when putting on sweaters and jackets and carrying in groceries. She denies any history of pain, repetitive trauma, or weakness in the hands. On physical examination, she has 3.5/5 strength in shoulder abduction and flexion, as well as the below rash. She reports the rash has been present for about the same time, but doesn’t really bother her.
Monteggia Fracture
Other Known Aliases – none
Definition – proximal 1/3 ulnar fracture with radial head dislocation

Clinical Significance – This type of injury pattern is most commonly seen with FOOSH injuries and is more common in children than adults with a peak incidence of 4-10 years of age. There are four different classifications depending on the injury pattern. There is also high incidence of neurovascular compromise and a good bedside exam is paramount prior to surgical repair.

History – Named after Giovanni Battista Monteggia (1762-1815), who was an Italian surgeon and received his medical doctorate from the University of Pavia in 1789 at the age of seventeen. He would begin his career as a surgery apprentice at the Great Hospital in Milano in 1790 culminating in professor of anatomy and surgery in 1795. His knowledge of anatomy and skill as a surgeon impressed his a very famous colleague at the University of Pavia, one Antonio Scarpa. He published his eponymous injury in 1814 in his textbook entitled “Institziono Chirurgiche”. Of note, the first radiograph was not taken until 1895.


References
Question
57yo woman comes into clinic complaining of a six-month history of right shoulder pain. She states that the pain is worse with overhead activities of the shoulder and when she is lifting and pulling with that arm. She has been more playing more tennis with her husband during this time as well, but has never had any other issues with this shoulder or arm before. She also reports painful arc of shoulder rotation with clicking that she feels on the anterior part of her shoulder. On physical examination, she has a negative drop arm and empty can test with no significant pain on resisted external rotation.
Answer
Given the history and negative findings on rotator cuff maneuvers, the next two maneuvers shoulder be the Yergason and Speed tests. If the patient has pain with either of these then it suggests biceps tendonitis as the cause of their shoulder pain. Anatomically, the origin of the long head of the biceps is near the insertion of the supraspinatus tendon. This is why you always assess biceps tendonopathy in patient presenting with shoulder pain.

De Quervain Tenosynovitis
Other Known Aliases – BlackBerry thumb, mother’s wrist, washerwoman’s sprain
Definition – inflammation of the abductor pollicis longus and extensor pollicis brevis tendons in the first extensor compartment at the styloid process of the radius.


Clinical Significance – The pathogenesis is not well understood, but is most accepted to be caused by repetitive activities that maintain the thumb in extension and abduction. Treatment is graded from thumb spica splinting, NSAIDs, corticosteroid injections, up to surgical release of the first extensor compartment.
History – Named after Fritz de Quervain (1868-1940), who was a Swiss surgeon and received his medical doctorate from the University of Bern in 1892. He would start his career training under Hugo Kronecker, Theodor Langhans, and Theodor Kocher, before becoming director of the surgical department at the La Chaux-de-fonds in Neuchâtel in 1897, and culminating in professor of surgery and director of the Inselspital at the University of Bern in 1918. He was a strong proponent of the generalist approach to patient care rather than the specialization of physicians and surgeons. He would describe his eponymous findings in his classic textbook series Spezielle chirurgische Diagnostik (Special Surgical Diagnosis) in 1907.


References
Question
57yo woman comes into clinic complaining of a six-month history of right shoulder pain. She states that the pain is worse with overhead activities of the shoulder and when she is lifting and pulling with that arm. She has been more playing more tennis with her husband during this time as well, but has never had any other issues with this shoulder or arm before. She also reports painful arc of shoulder rotation with clicking that she feels on the anterior part of her shoulder. On physical examination, she has a negative drop arm and empty can test with no significant pain on resisted external rotation.
