Rovsign’s Sign
Other Known Aliases – none
Definition – palpation of the left lower quadrant causes perceived pain in the right lower quadrant
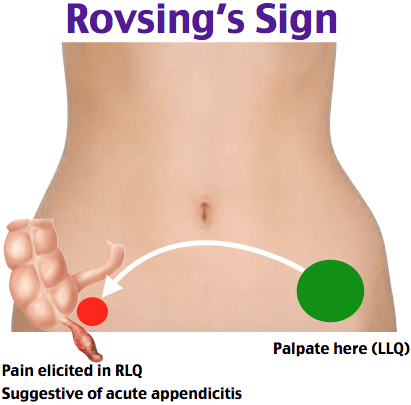
Clinical Significance – A positive Rovsing’s sign is suggestive of appendicitis. There are two mechanisms that illicit this response. First, palpation of the left lower quadrant stretch the peritoneal lining over the appendix and causes pain. Second, deep palpation of descending colon in the left lower quadrant causes the gas present to stretch the lumen of the colon and appendix causing pain.

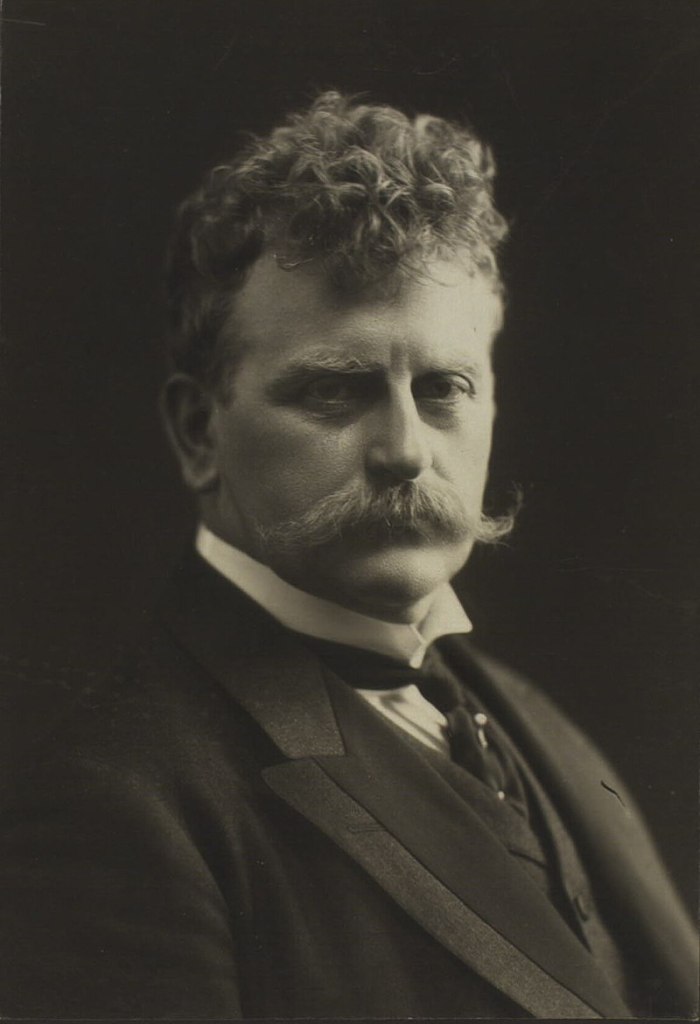
History – Named after Niels Thorkild Rovsing (1862-1927), who was a Danish surgeon and received his medical doctorate from the University of Copenhagen in 1885. He went on to become professor of operative surgery there in 1899, as well as chief surgeon at Louise-Børnehospital and Red Cross Hospital. He was a huge advocate for better surgical accommodations for patients, even going so far as to commission his own private surgical nursing home to care for his postoperative patients. He was international recognized as an accomplished abdominal surgeon, writing extensively on these surgical diseases. He first published his findings of his eponymous exam finding in 1907 in an article entitled “Indirect cause of typical pain at McBurney’s point”.
He also has several other surgical eponyms attributed to him including:
- Rovsing Operation I and II for horseshoe kidney
- Rovsing Syndrome
References
- Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
- Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
- Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
- Whonamedit – dictionary of medical eponyms. http://www.whonamedit.com
- Up To Date. www.uptodate.com
- N. T. Rovsing. Indirektes Hervorrufen des typischen Schmerzes an McBurney’s Punkt. Ein Beitrag zur diagnostik der Appendicitis und Typhlitis. Zentralblatt für Chirurgie, Leipzig, 1907, 34: 1257-1259.