59yo male, with a history 27-pack-year history of smoking, presents to your primary care clinic for follow-up after a motor vehicle accident. He was evaluated in the local ED and was found to have a two masses on his liver on abdominal CT. What is the most likely cause of these lesions?
Other Known Aliases – urine monoclonal globulin protein
Definition – immunoglobulin paraproteins produced by neoplastic plasma cells that are found in the urine due to decreased kidney filtration from acute kidney injury
Clinical Significance – Bence Jones proteins are classically associated with multiple myeloma and Waldenström’s macroglobulinemia and these proteins were detected by heating a urine specimen to promote precipitation of the protein, but now is seen on electrophoresis of concentrated urine. Newer serum free light chain assays have been shown to be more sensitive and superior to the urine studies and are coming into favor.
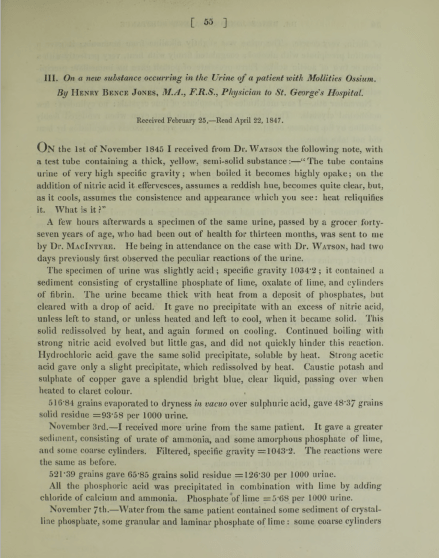
History – Named after Henry Bence Jones (1813-1873), who was an English physician and chemist and received his medical doctorate from St. George’s Hospital in 1840. His love for chemistry was sparked during his medical training and he simultaneously undertook private instruction in chemistry studies from professor Thomas Graham. After medical school, he went to Giessen, Germany to train under Justus von Liebig’s (the leading chemist of his time) at his animalistic chemistry school. He described his eponymous finding in 1847 in an article entitled “On a new substance occurring in the urine of a patient with Mollities Ossium”. His work on applying chemistry principles to human disease was so far ahead of his time that his work was not nearly as successful as it should have been due to the lack of knowledge of biochemistry and physiology of the time.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
57yo Caucasian male presents to his primary provider with a one-year history of joint pain, weakness, and fatigue. He has a past medical history significant for hypertension and hyperlipidemia, for which he is being treated and is controlled on medications. His wife reports his skin has become a little darker over the last year as well. The rest of his physical examination does not reveal any abnormalities. Routine chemistries show a glucose of 214 mg/dL, AST of 472 mg/dL, and ALT of 513 mg/dL. What two (2) laboratory studies should be ordered next?
Answer
Hemochromatosis is at the top of the differential in a patient with elevated transaminases, heart disease, arthropathy, and hyperpigmented skin changes. As part of the initial screening, iron studies should be performed and an elevated transferrin saturation and serum ferritin are both elevated in hemochromotosis.
References
Bacon BR, Adams PC, Kowdley KV, Powell LW, Tavill AS, . Diagnosis and management of hemochromatosis: 2011 practice guideline by the American Association for the Study of Liver Diseases. Hepatology (Baltimore, Md.). 2011; 54(1):328-43. [pubmed]
Definition – pain in the posterior leg (classically behind the knee) with forced dorsiflexion of the foot
Clinical Significance – this examination finding was used in patients with a suspected DVT and before D-Dimers and clinical ultrasound were readily available. It is clinically useless as it has been studied extensively and found to have a sensitivity of 10-54% and specificity of 29-89%, thus not ruling in or out the condition consistently.
History – Named after John Homans (1877-1954), who was an American surgeon and received his medical doctorate from Harvard Medical School. He worked with Harvey Cushing and Samuel Crowe early in career exploring the connection between the piuitary gland and the reproductive system. He first described his eponymous finding in 1944 in a NEJM article entitled “Diseases of the veins” and later published the first case report of a DVT occuring after prolonged sitting on a flight between Boston and Caracas in 1954. He was a founding member of the the Society for Vascular Surgery and the namesake of the John Homans Chair of Surgery position at Harvard Medical School and John Homans Fellowship in Vascular Surgery at the Brigham and Women’s Hospital.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
57yo Caucasian male presents to his primary provider with a one-year history of joint pain, weakness, and fatigue. He has a past medical history significant for hypertension and hyperlipidemia, for which he is being treated and is controlled on medications. His wife reports his skin has become a little darker over the last year as well. The rest of his physical examination does not reveal any abnormalities. Routine chemistries show a glucose of 214 mg/dL, AST of 472 mg/dL, and ALT of 513 mg/dL. What two (2) laboratory studies should be ordered next?
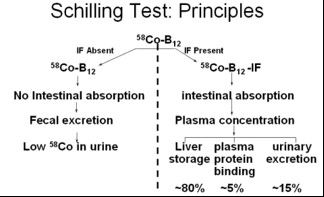
Definition – laboratory test for pernicious anemia (specifically intrinisic factor deficiency) that led to vitamin B12 (cobalamin) deficiency. It involved ingesting a oral dose of radiolabeled vitamin B12 (to test oral absorption), an IM injection of vitamin B12 (to saturate liver stores), and a 24hr urine collection to see how much was absorbed and excreted. If intestinal absorption was intact (intrinsic factor present), then > 10% of the radiolabeled vitamin B12 would be in the urine.
Clinical Significance – This was the first and only test at the time to be able to diagnose pernicious anemia, but is now largely a test of historical interest only as better diagnostic studies have been developed.
History – Named after Robert F. Schilling (1919-2014) an American physician and researcher who received his medical doctorate from the University of Wisconisn-Madison in 1943. Immediately after graduation, he joined the Pacific Front as a physician in the 3d Marine Division. After the war, he completed postgraduate training at Harvard before returning to Wisconsin to practice hematology. He studied extensively on the metabolism of vitamin B12 and the urinary excretion of radiolabeled vitamin B12 in pernicious anemia and in 1953, published a paper entitled “The effect of gastric juice on the urinary excretion of radioactivity after the oral administration of radioactive vitamin B12”, which would go on to be called the “Schilling Test”.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Schilling RF. Intrinsic factor studies. 2. The effect of gastric juice on the urinary excretion of radioactivity after the oral administration of radioactive vitamin B12. J Clin Lab Med. 1953;42;860-866
Polycystic ovarian syndrome (PCOS) can often be a clinical diagnosis due to the classic distinguishing features of hirsutism, obesity, menstrual irregularities, and infertility. What is the classic relationship between FSH and LH in a patient with PCOS?
Answer
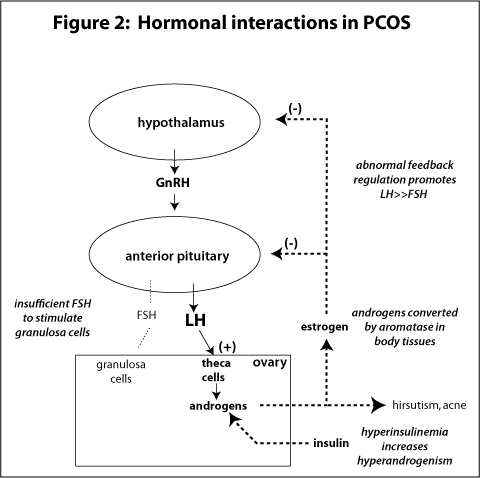
The classic relationship between LH and FSH in PCOS is > 2.5:1.
LH secretion is elevated, while FSH secretion is the same, or even decreased. LH stimulates theca cell proliferation and secretion of androgens, but there is insufficient FSH to stimulate granulosa cells. Although this is classically seen, LH:FSH is NOT used in any diagnostic criteria for PCOS.
Clinical Significance – Most commonly arising from a gastric adenocarcinoma, but can occur from any metastatic cancer. 80% are bilateral and commonly manifest as pelvic pain, bloating, ascites, or dysparunea. Occasionaly, these tumor can be hormone producing and cause abnormal menstrual bleeding, hirsuitism, or virilization.
History – Named after Friedrich Ernst Krukenberg (1871-1946), who was a German physician and received his medical doctorate from the University of Marburg. He was actually studying to become a ophthalmologist, when he happend to be spending time in the pathology lab under Felix Marchand. It was in this department that Krukenberg described a fibrosarcoma of the ovary (using sections from tumors Marchand had found in 1879) and published his findings in an article entitled “Über das Fibrosarcoma ovarii mucocellulare (carcinomatodes)” in 1896 at the age of 25 as part of his doctoral thesis. He spent the rest of career in his hometown of Halle, Germany practicing as a ophthalmologist.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
American College of Obstetrics and
Gynecology (ACOG) recommends:
All women should be offered
screening before 20 weeks
All women should have the option for
having a more invasive procedure instead of screening regardless of maternal
age
Amniocentesis
Chorionic villus sampling
Two major categories of screening
available
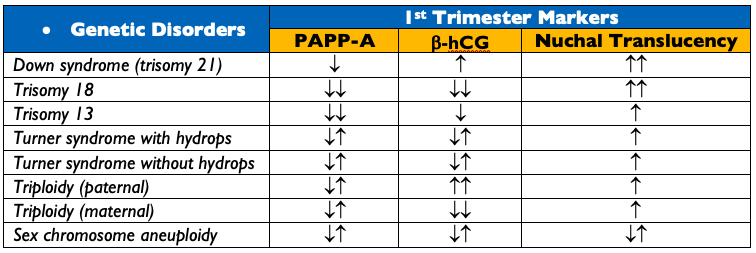
Specific maternal serum biomarkers
Primarily trisomy 21 and 18
Maternal circulation cell-free DNA
More sensitive
Assesses trisomy 21, 18, 13, and sex
chromosome aneuploidies
Carrier Screening
ACOG recommends:
All women should be offered carrier
screening for cystic fibrosis, spinal muscular dystrophy, thalassemias, and
hemoglobinopathies
Fragile X
All women with a family history of
intellectual disability, developmental delay, or autism
Each provider develop a screening
strategies for ethnic-specific and panethnic populations
If there is a (+) screening test in
the mother, then the reproductive partner should be offered screening
Standard Panel Laboratory Screening
ABO and Rh Screen
RhD(-) women should receive prophylactic anti(D)-immune globin at 28-weeks
Complete Blood Count and RBC Indices
1st Screen for anemia
Documentation of Rubella and Varicella Immunity
Rubella IgG
Varicella IgG
Urinalysis and Urine Culture
Urine Protein – establish baseline to compare if patient develops pre-eclampsia or eclampsia
Untreated, asymptomatic has higher rates of developing pyelonephritis, pre-term birth
HIV Screen
ACOG recommends “opt-out” approach
Hepatitis B
HBsAg regardless of immunization status
Chlamydia
Nucelic Acid Amplification Test (NAAT) of endocervical/vaginal swab or urine
Syphilis
Can screen with either a non-treponemal or treponemal test, but a (+) screening test is confirmed with a treponemal test
Selective Screening in 1st
Trimester
Thyroid Function – TSH only
Overt diabetes screening
Obtain HgbA1C if BMI > 25 (23 in Asian Americans) AND at least one of the
following:
Gestational diabetes in previous pregnancy
HgbA1C > 5.7%, impaired glucose
tolerance, or impaired fasting glucose on previous testing
1st degree relative with
diabetes
African-American, Latino, Native
American, Asian American, Pacific Islander
History of cardiovascular disease
Hypertension (> 140/90 or on
medication)
Age > 40yr
HDL cholesterol < 35 mg/dL or
triglyceride > 250 mg/dL
PCOS
Physical inactivity
Other insulin resistance conditions
If HgbA1C > 6.5%, then treat as
overt diabetes
If HgbA1C (-), then screen again at
24-28 weeks
Infections
Gonorrhea
NAAT from endocervical/vaginal swab
Hepatitis C
High risk patient should be screened
with anti-HCV antibody or HCV RNA
Tuberculosis
Screen with tuberculin skin test or
interferon-gamma release assay (IGRA) only if:
Suspicion for recent TB infection
Immunocompromised
Others
Toxoplasmosis, trichomonas, herpes
simplex, cytomegalovirus, Zika, and Chagas are available for at risk patients
or in endemic regions
Lead
Women with symptoms of lead exposure
or risk factors
15-24 Weeks
These are not universal and are
options available to mothers
Quadruple Test
Maternal serum alpha-fetoprotein
level
Unconjugated estriol
Human chorionic gonadotropin
Inhibin A
Fetal ultrasound
Can be used to screen for neural
tube defects and other fetal anomalies, as well as screen the mother for a
short cervical length (< 25mm) that can increased her risk of spontaneous
preterm birth
24-28 Weeks
Gestational Diabetes Screening
Two-Step Approach
Step One – Screening
50g, one-hour glucose challenge test REGARDLESS of time of day or last meal
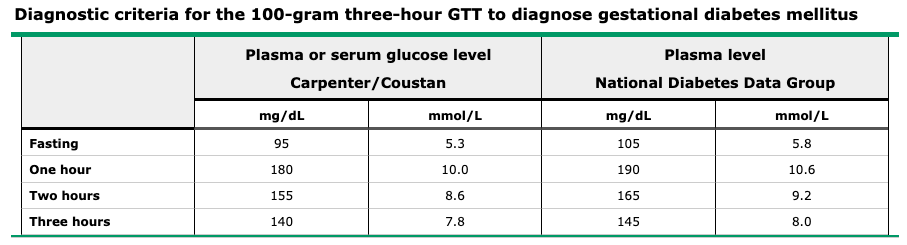
Step Two – Diagnostic
100g, three-hour oral glucose tolerance test
Traditionally diagnostic after 2 elevated values, but newer data suggests that one may be OK
75g, two-hour oral glucose tolerance test
Diagnostic after a single elevated value, but patient must be fasting
Up-To-DateUp-To-Date
Complete Blood Count with iron and
folate studies
2nd anemia screening
28-36 Weeks
Sexually Transmitted Infection
Screening
HIV, syphilis, chlamydia, gonorrhea,
hepatitis B and C
Based on either previous (+) result
or evidence of risk factors
Up-To-Date
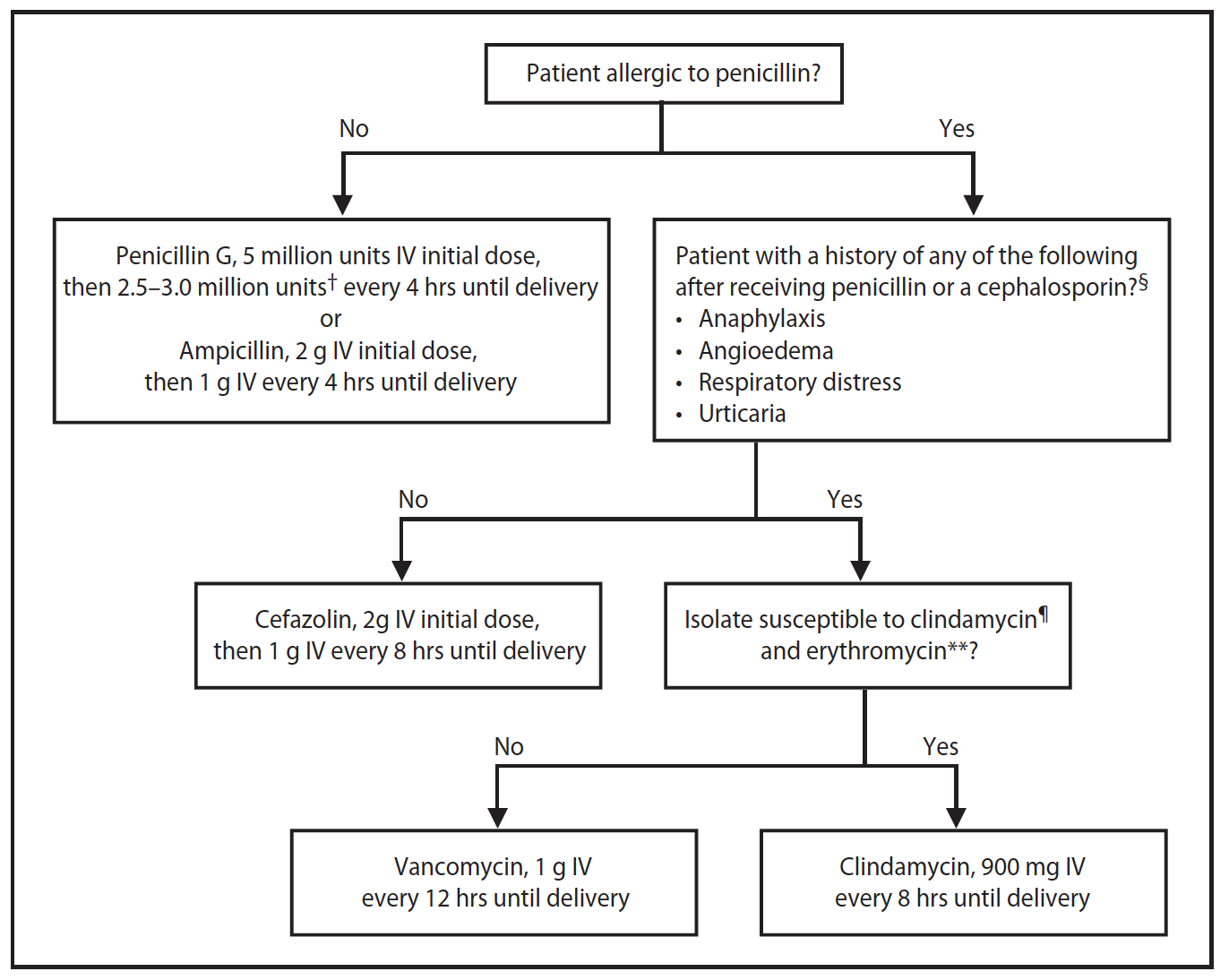
Screen for group B beta-hemolytic
streptococcus
Vaginal and rectal swabs
(+) results treated with intrapartum
prophylaxis
CDC – GBS Prophylactic Antibiotic Algorithm
Screen for Fetal Growth Restrictions
(<10th percentile weight for gestational age)
Indicated in third trimester in
pregnancies at high risk
ACOG Practice Bulletin No. 77: screening for fetal chromosomal abnormalities. Obstetrics and gynecology. 2007; 109(1):217-27. [pubmed]
ACOG Practice Bulletin No. 88, December 2007. Invasive prenatal testing for aneuploidy. Obstetrics and gynecology. 2007; 110(6):1459-67. [pubmed]
ACOG Committee Opinion No. 752: Prenatal and Perinatal Human Immunodeficiency Virus Testing. Obstetrics and gynecology. 2018; 132(3):e138-e142. [pubmed]
Roberts SW, Sheffield JS, McIntire DD, Alexander JM. Urine screening for Chlamydia trachomatis during pregnancy. Obstetrics and gynecology. 2011; 117(4):883-5. [pubmed]
Hughes BL, Page CM, Kuller JA. Hepatitis C in pregnancy: screening, treatment, and management. American journal of obstetrics and gynecology. 2017; 217(5):B2-B12. [pubmed]
ACOG Practice Bulletin No. 190: Gestational Diabetes Mellitus. Obstetrics and gynecology. 2018; 131(2):e49-e64. [pubmed]
Bricker L, Medley N, Pratt JJ. Routine ultrasound in late pregnancy (after 24 weeks’ gestation). The Cochrane database of systematic reviews. 2015; [pubmed]
Polycystic ovarian syndrome (PCOS) can often be a clinical diagnosis due to the classic distinguishing features of hirsutism, obesity, menstrual irregularities, and infertility. What is the classic relationship between FSH and LH in a patient with PCOS?