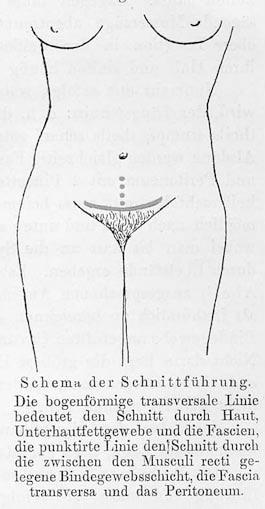
Definition – 8-10cm transverse (slightly arched) incision made 2-3cm cephalad to the pubic symphasis. The rectus sheath is then retracted cephalad and the rectus abdominis muscle bellies are divided longitudinally to enter the peritoneum
Clinical Significance – This is the primary incision for cesarean sections because it follows the Langer Lines and can achieve excellent cosmetic results. There are also decreased rates of postoperative pain, fascial dehiscence, and incisional hernias noted.
History – Named after Hans Hermann Johannes Pfannensteil (1862-1909), who was a German gynecologist and received his medical doctorate from the University of Berlin in 1885. He was an extraordinary surgeon and teacher and published extensively on many gynecological conditions. In 1900, he published an article describing the the advantages of his eponymous transverse fascial incision for gynecologic laparotomies. Dr. Pfannensteil unfortunately died from septicemia at the age of 47 after injuring his finger draining a tubo-ovarian abscess.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Pfannenstiel HJ. (On the advantages of the symphyseal transverse fascial incision for gynecological caliotomies as well as the contribution to the surgical indications). Samml Klin Vortr. 1900;268:1735-56
You have just assisted with a relatively uneventful spontaneous vaginal delivery of a 38-week newborn to a 29-year-old G1P0001 mother. During your immediate, postpartum maternal assessment, you notice a large amount of vaginal bleeding persisting.
Questions
What is the most common cause of this condition?
What are the two most important steps in managing this?
What are some of the other etiologies to think about?
Answers
The most common cause of post-partum hemorrhage is uterine atony and is responsible for up to 75% cases. The amount of bleeding can also be much greater than what is visible due to the flaccid and dilated uterus.
The two most important steps in managing uterine atony are:
Performing bi-manual uterine massage to stimulate contraction
Administration of uterotonics
ALL women get oxytocin either:
15 units in 250mL of LR
10 units IM
If still bleeding after oxytocin:
Carboprost tromethamine (Hemabate) 0.25mg IM every 15min up to a max dose of 8mg
Methergine 0.2mg IM every 2-4 hours
Misprostol 400mcg (SL/buccal/rectal)
Uterine atony is the most common cause of post-partum hemorrhage, but is responsive to uterotonics in most instances, so it is not the most common cause of massive transfusion. Other etiologies to think about are:
Retained placenta/membranes
Lacerations or rupture
HELLP syndrome
Abnormal placentation
References
Bateman BT, Berman MF, Riley LE, Leffert LR. The epidemiology of postpartum hemorrhage in a large, nationwide sample of deliveries. Anesthesia and analgesia. 2010; 110(5):1368-73. [pubmed]
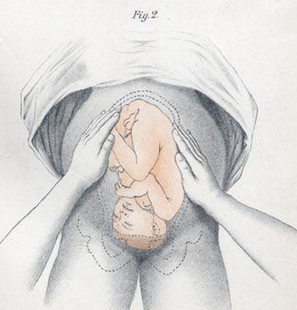
Definition – Series of four distinct actions to systematically determine the lie and position of the fetus in utero:
First Maneuver – Fundal Grip
used to locate fetal position (breech vs vertex)
Second Maneuver – Umbilical Grip
used to locate the back of the fetus
Third Maneuver – Second Pelvic Grip
used to determine pelvic inlet position
Fourth Maneuver – First Pelvic Grip
used to locate the fetal brow
Clinical Significance – These are now an antiquated way to determine fetal positioning to predict difficult deliveries or need for cesarean section. These have largely been replaced by obstetrical ultrasound.
History – Named after Christian Gerhard Leopold (1846-1911), who was a German gynecologist and received his medical doctorate from the University of Leipzig in 1870. He spent the early part of his career teaching midwifery at the Frauenklinik in Leipiz before taking a professorship at the University of Leipzig in 1883. Later that same year, he took over as the Director of the Dresden Royal Gynaecological Infirmary and by the end of his tenure developed it into a leading hospital in Germany. He published his eponymous maneuvers in several articles (first in 1894) in the journal Archiv für Gynäkologie, for which he was a co-editor.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
You have just assisted with a relatively uneventful spontaneous vaginal delivery of a 38-week newborn to a 29-year-old G1P0001 mother. During your immediate, postpartum maternal assessment, you notice a large amount of vaginal bleeding persisting.
Questions
What is the most common cause of this condition?
What are the two most important steps in managing this?
What are some of the other etiologies to think about?
Definition – systolic precordial crunching sound that occurs with each contraction of the heart that is best heard over precordium in the left lateral decubitus position
Clinical Significance – this is one of the classic physical examination findings in pneumomediastinum or pneumopericardium as a result of trauma to the bronchial tree, bleb rupture, or esophageal rupture.
History – Named after Louis Virgil Hamman (1877-1946), an American internists who received his medical doctorate from Johns Hopkins University in 1902. He was considered one of the great physicians of his era and made significant progress in the management of tuberculosis as the head of the Phipps Tuberculosis Clinic at Johns Hopkins. He described this finding in patients with spontaneous mediastinal emphysema in two separate articles, first in 1939 in The Bulletin of Hopkins Hospital, and then in JAMA in 1945.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
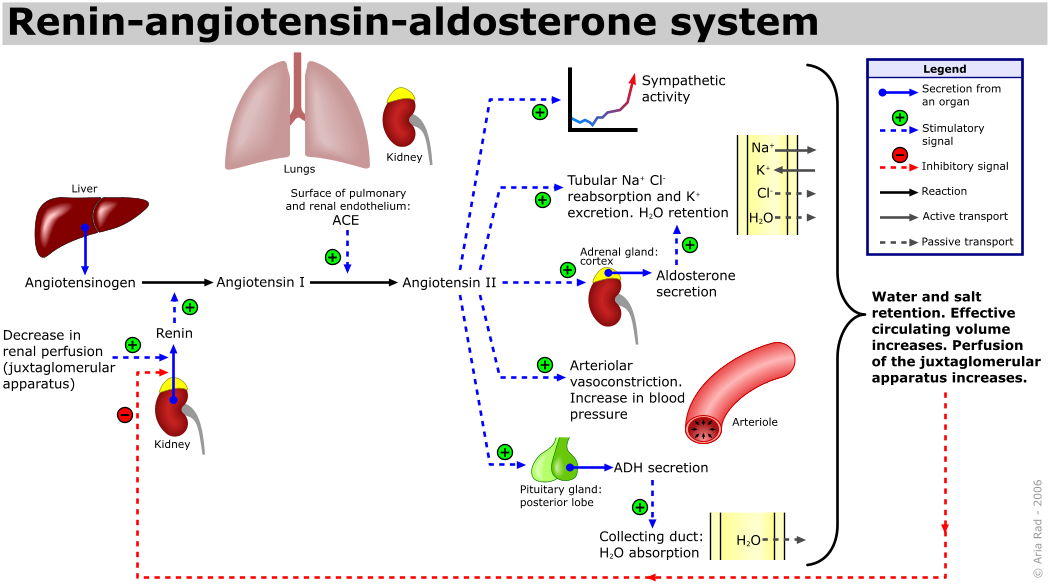
Angiotensin converting enzyme (ACE) inhibitors are one of the more common medications used in the management of primary hypertension. What are some potential adverse reactions from and contraindications to using ACE inhibitors?
Answer
Cough
10% of patient experience a dry, hacking cough
Hypotension
2% of patients can experience hypotension, weakness, or dizziness from excessive reduction in blood pressure
Reduction in GFR
2% of patients can see a doubling in creatinine due to decreased intrarenal perfusion as a result of increased efferent arteriole resistance
Hyperkalemia
3% of patients can have a potassium > 5.5 mEq/L by reducing urinary potassium excretion
Angioedema
0.3% of patients can experience potentially life-threatening angioedema
Pregnancy
Associated with cardiac malformations in the first trimester and renal malformations in the second/third trimesters
References
Israili ZH, Hall WD. Cough and angioneurotic edema associated with angiotensin-converting enzyme inhibitor therapy. A review of the literature and pathophysiology. Annals of internal medicine. 1992; 117(3):234-42. [pubmed]
Bangalore S, Kumar S, Messerli FH. Angiotensin-converting enzyme inhibitor associated cough: deceptive information from the Physicians’ Desk Reference. The American journal of medicine. 2010; 123(11):1016-30. [pubmed]
ONTARGET Investigators – Yusuf S, Teo KK, et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. The New England journal of medicine. 2008; 358(15):1547-59. [pubmed]
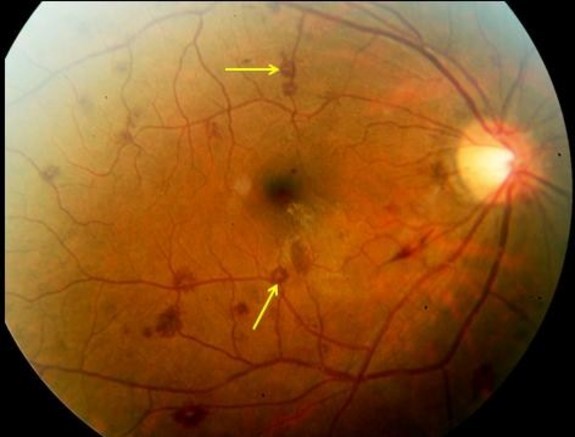
Definition – exudative, edematous hemorrhagic lesions of the retina with pale, white centers that can be composed of coagulated fibrin, platelets, infectious organisms, or neoplastic cells
Clinical Significance – one of the classic physical examination findings in bacterial endocarditis seen on fundoscopy. Further research and analysis has shown these can be present in leukemia, diabetes, and hypertensive retinopathy
History – named after Mortiz Roth (1839-1914), who was a Swiss pathologist and recieved his medical doctorate from University of Basel in 1864. He practiced all around Switzerland before returning to Basel as professor extraordinary of pathology in 1872, when he published his now eponymous findings in an article entitled “Uber Netzhauteffecstionen bei wundfiebren [Retinal Manifestations of wound fever]”. Dr. Roth, though, never described the classic appearance of the retinal red spot with a white center. Dr. Moritz Litten described this finding 6 years later and would coin the term we still use today.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Definition – sounds heard during auscultation of the brachial artery during blood pressure measurements
Clinical Significance – these sounds are generated as the sphygmomanometer cuff is slowly being deflated to the point that the maximal impulse of the pressure wave is more than cuff, but the cuff still occluded the artery at the nadir of the impulse. This pressure difference produces turbulence in the blood flow and the characteristic sound on auscultation. There are five phases to the Korotkov sounds with the initiation of Phase 1 as the systolic pressure and the end of Phase 4 as the diastolic pressure.
History – named after Nicholai Korotkov (1874-1920), who was a Russian surgeon and earned his medical degree from Moscow University in 1895. He had a prestigious career as a military physician and surgeon earning him an appointment as professor of surgery at the Military Medical Academy at St. Petersberg in 1903. He was preparing his doctoral thesis on vascular surgery when he described his now famous technique for measuring blood pressure in only a 281 word excerpt from a presentation to the Imperial Military Medical Academy entitled “Izvestie Imp. Voiennomedicinskoi Akademii” in 1905.
Nicolai KorotkovKorotkov’s personal sphygmomanomter
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Shevchenko YL, Tsitlik JE. 90th Anniversary of the development by Nikolai S. Korotkoff of the auscultatory method of measuring blood pressure. Circulation. 1996; 94(2):116-8. [pubmed]
Complex clinical syndrome resulting
from conditions that affect the structure and/or function of the heart
culminating in reduced systemic perfusion that is inadequate to meet the
metabolic demands of the body
Main effect is decreased cardiac
output
No more “congestive”
Epidemiology
5.7 million adults in US
550,000 new cases each year
1.4 million are under 60 years of
age
Annual incidence is 10 per 1,000
population AFTER 65 years of age
287,000 deaths per year
1 in 9 deaths included heart failure
as contributing causes
Most common diagnosis in hospital
patients over 65 years of age
Responsible for 11 million office
visits each year in the US and more hospitalizations than all cancers COMBINED
50% of adults who develop heart
failure die within 5 years
Cost to US is ~$30 billion/year
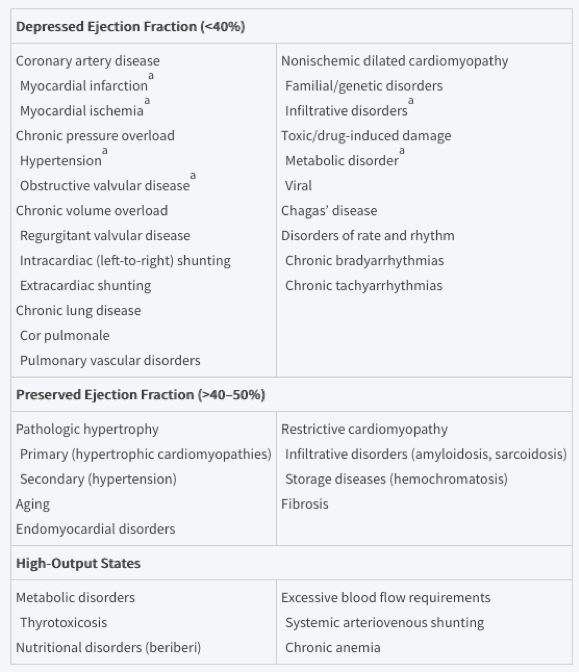
Causes and Pathophysiology
Any
condition that leads to alteration in left ventricular structure or function
can cause heart failure and the specific causes depends on the preservation of
ejection fraction. There is considerable
overlap between these with coronary artery disease and hypertension causes the
majority of cases.
The
problem is that the rest of the body feel the effects of the decreased cardiac
output and activate the neurohormonal systems to compensate. The issue is that this makes the heart
failure worse and it is a vicious cycle until it can be broken.
Signs and Symptoms
History
Reduced
cardiac output
Fatigue,
weakness
Excessive
fluid accumulation
Dyspnea,
orthopnea, paroxysmal nocturnal dyspnea, leg swelling, abdominal discomfort,
palpitations
Physical
Examination
Appearance
and Vital Signs
Resting
sinus tachycardia
Narrow
pulse pressure
Cool,
pale skin (peripheral vasoconstriction)
Volume
Assessment
Pulmonary
congestion
Rales
on auscultation
AUDIO
Peripheral
edema
Leg
swelling, hepatic congestion, ascites, scrotal edema
Elevated
jugular venous pressure
Hepatojugular
reflux
Cardiac
S3 with gallop (if systolic failure)
S4 (if diastolic failure)
Displaced PMI past midclavicular line and below the 5th intercostal space
Pulsus alternans
Evenly spaced alternating strong and weak peripheral pulses
Pulsus Alternans
Framingham Clinical Criteria for Heart Failure
Clinical Decision Rule for Heart Failure
Age
<
60 = 0 points
60-70
= 4 point
71-80
= 7 points
>
80 = 10 points
History
of coronary disease = 15 points
AMI,
CABG, PCI
Loop
diuretic = 10 points
Displaced
PMI = 20 points
Rales
= 14 points
Irregularly
irregular pulse = 11 points
Heart
murmur = 10 points
Pulse
Rate = (HR-60)/3 points
Elevated
jugular venous pressure = 12 points
NT-proBNP
(pg/mL)
<
100 = 0 points
100-200
= 8 points
200-400
= 16 points
400-800
= 24 points
800-1600
= 32 points
1600-3200
= 40 points
>
3200 = 48 points
Interpretation
<
13 points = < 10% probability of heart failure
>
54 points = > 70% probability of heart failure
Diagnostic Studies
Electrocardiogram
Not
really diagnostic, but can evaluate for current ischemia, past infarction, low
voltage, dysrhythmias
A
normal EKG makes systolic dysfunction unlikely (98% NPV)
Laboratory
studies
Brain
natriuretic peptide (BNP) and N-terminal proBNP (NT-proBNP)
Released
from ventricles when stretched
<
100 pg/mL = very high NPV and rule out heart failure
Cardiac
enzymes
CBC
CMP
Chest
Radiography
Increased
cardiothoracic ratio
Cephalization
of pulmonary vessels
Kerley
B-lines
Pleural
effusions
Echocardiography
Recommended for all patient with dyspnea and suspicion of heart failure
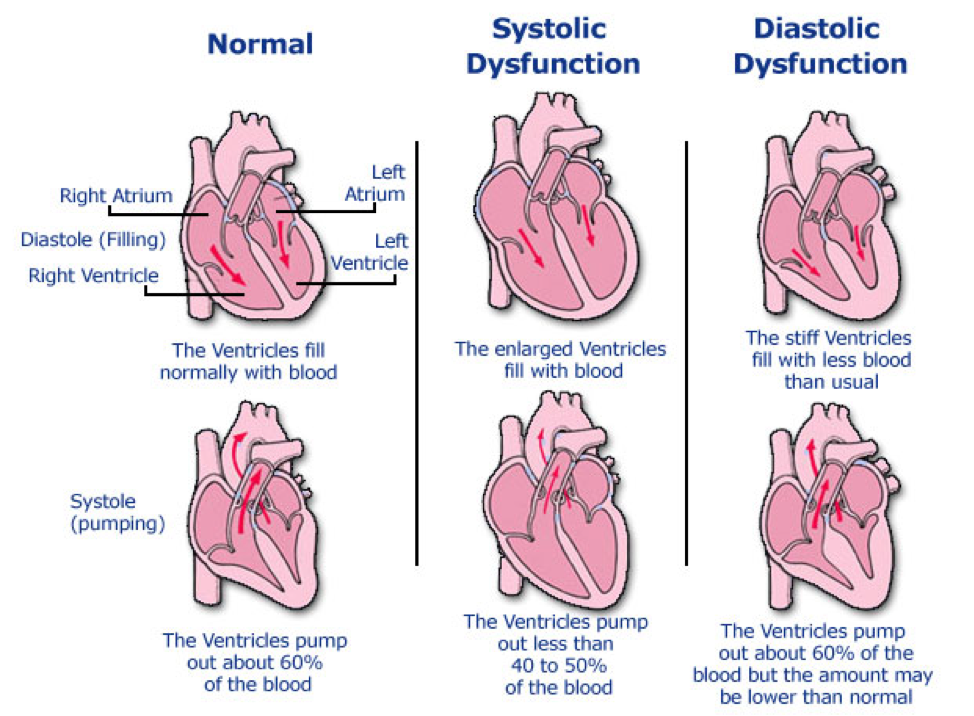
Provides vital information on:
Ejection fraction
< 40% = reduced = systolic
> 50% = preserved = diastolic
Valvular disease
Aortic and mitral regurgitation/insufficiency
Atrial and Ventricular size and function
Enlarged left ventricle = systolic
Left atrial enlargement with normal/small left ventricle = diastolic
Left ventricular wall size
Thin = systolic
Thick = diastolic
Exercise/Stress
Testing
Evaluate
for underlying coronary disease, as well as potential candidates for
transplantation
Patients
with a peak oxygen uptake (VO2) < 14 mL/kg/min have better outcomes with
transplanted
Coronary
angiography
Not
strongly recommended as part of the work-up, but can be useful to evaluate for
underlying coronary disease and get an accurate ejection fraction
Classification and Grading
Current Nomenclature
Heart failure with reduced ejection fraction (HFrEF)
Systolic
< 40% EF
Heart failure with preserved ejection fraction (HFpEF)
Diastolic
> 50% EF
Management
Heart failure with reduced ejection
fraction (HFrEF)
Lifestyle Modifications
Smoking cessation
Restrict sodium to < 3g/day
Restrict fluid to < 2L/day
Pharmacotherapy
Loop diuretic (if overload is
present)
Furosemide, bumetanide, torsemide
ACE inhibitors
Lisinopril, enalapril
Angiotension receptor-neprilysin
inhibitor (ARNI)
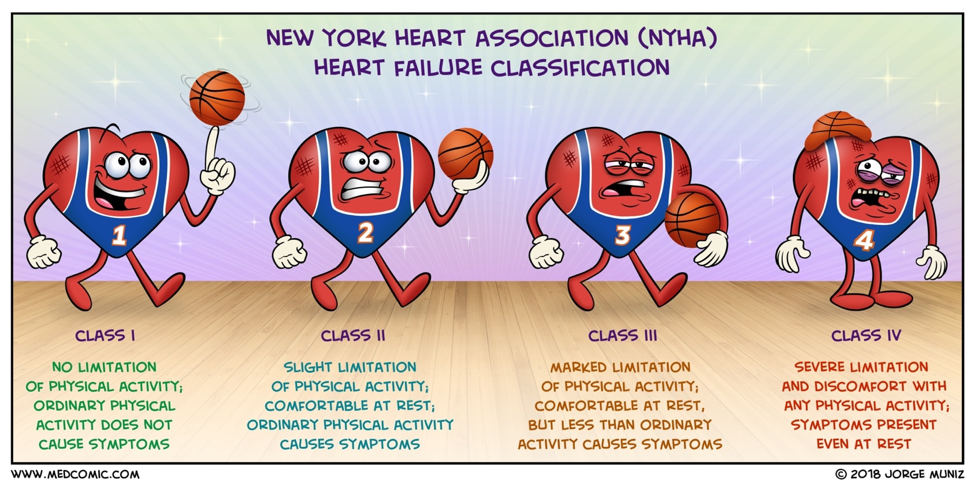
NYHA II or III and:
BNP > 150 ng/mL or hospitalized
with last 12 months
SBP > 100 mmHg
GFR > 30 mL/min
No history of angioedema
ARB
Candesartan, valsartan
Beta blockers
Carvedilol, metoprolol, bisoprolol
Mineralcorticoid receptor antagonist
(MRA)
Spironolactone, eplerenone
Selective sinus node inhibitor
Ivabradine
Need a resting HR > 70 bpm on
maximum BB therapy
Ischemic heart disease
Increase coronary perfusion
Decrease myocardial demand
Hyperlipidemia
High-intensity statin
Cardiac rehabilitation
Heart failure with preserved
ejection fraction (HFpEF)
Differences with HFrEF
ACEI/ARB not as useful
MRA used more often
Diuretics OK but be careful for volume
depletion
Don’t use BB unless compelling
indication
References
Tan LB, Williams SG, Tan DK, Cohen-Solal A. So many definitions of heart failure: are they all universally valid? A critical appraisal. Expert review of cardiovascular therapy. 2010; 8(2):217-28. [pubmed]
Davie AP, Francis CM, Caruana L, Sutherland GR, McMurray JJ. Assessing diagnosis in heart failure: which features are any use? QJM : monthly journal of the Association of Physicians. 1997; 90(5):335-9. [pubmed]
Kelder JC, Cramer MJ, van Wijngaarden J, et al. The diagnostic value of physical examination and additional testing in primary care patients with suspected heart failure. Circulation. 2011; 124(25):2865-73. [pubmed]
Davie AP, Francis CM, Love MP, et al. Value of the electrocardiogram in identifying heart failure due to left ventricular systolic dysfunction. BMJ (Clinical research ed.). 1996; 312(7025):222. [pubmed]
Maisel A. B-type natriuretic peptide levels: diagnostic and prognostic in congestive heart failure: what’s next? Circulation. 2002; 105(20):2328-31. [pubmed]
Knudsen CW, Omland T, Clopton P, et al. Diagnostic value of B-Type natriuretic peptide and chest radiographic findings in patients with acute dyspnea. The American journal of medicine. 2004; 116(6):363-8. [pubmed]
Badgett RG, Mulrow CD, Otto PM, Ramírez G. How well can the chest radiograph diagnose left ventricular dysfunction? Journal of general internal medicine. 1996; 11(10):625-34. [pubmed]
Bart BA, Shaw LK, McCants CB, et al. Clinical determinants of mortality in patients with angiographically diagnosed ischemic or nonischemic cardiomyopathy. Journal of the American College of Cardiology. 1997; 30(4):1002-8. [pubmed]
Ho KK, Pinsky JL, Kannel WB, Levy D. The epidemiology of heart failure: the Framingham Study. Journal of the American College of Cardiology. 1993; 22(4 Suppl A):6A-13A. [pubmed]
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013; 128(16):1810-52. [pubmed]
Yancy CW, Jessup M, et al. 2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure: An Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. Circulation. 2016; 134(13):e282-93. [pubmed]
Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. European heart journal. 2016; 37(27):2129-2200. [pubmed]
Parch J, Powell C. No longer failing to treat heart failure: A guideline update review. JAAPA : official journal of the American Academy of Physician Assistants. 2019; 32(1):11-15. [pubmed]