Other known aliases – hepatopancreatic sphincter, Glisson’s sphincter
Definition – muscular ring surrounding the major duodenal papilla at the 2nd portion of the duodenum.
Clinical Significance – the sphincter of Oddi allows for drainage of the biliary and pancreatic systems and dysfunction (mainly spasming) can can cause pancreatitis. It is in a constant state of contraction unless relaxed by cholesytokinin released by vasoactive intestinal peptide. Opioids, specifically morphine, has been shown to increase the risk of sphincter of Oddi dysfunction.
History – Named after Ruggero Ferdinando Antonio Guiseppe Vincenzo Oddi (1864-1913), who was an Italian physiologist and anatomist from Perugia. He spent is formative years studying medicine at Perugia, Bologna, and Florence and was appointed head of the Physiology Institute at the University of Genoa in 1894. In 1887, at only 23 years old, he described his eponymous structure in his paper “D’une disposition a sphincter speciale de l’ouverture du canal choledoque”. His career, unfortunately, was derailed and cut short due to opioid addiction many believe was as a result of using morphine derivatives to study dysfunction of the sphincter.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Helm JF, Venu RP, Geenen JE, et al. Effects of morphine on the human sphincter of Oddi. Gut. 1988; 29(10):1402-7. [pubmed]
Behar J. Physiology and Pathophysiology of the Biliary Tract: the Gallbladder and Sphincter of Oddi – A Review. ISRN Physiology, vol. 2013, Article ID 837630, 15 pages, 2013. https://doi.org/10.1155/2013/837630
Oddi R. D’une disposition a sphincter speciale de l’ouverture du canal choledoque. Arch Ital Biol. 1887;8:317–322
Loukas M, Spentzouris G, Tubbs RS, Kapos T, Curry B. Ruggero Ferdinando Antonio Guiseppe Vincenzo Oddi. World journal of surgery. 2007; 31(11):2260-5. [pubmed]
Initial screening test for suspected celiac disease is a serum immunoglobulin A (IgA) anti-tissue transglutaminase (TTG). If positive, it is then followed up with an endoscopic duodenal biopsy.
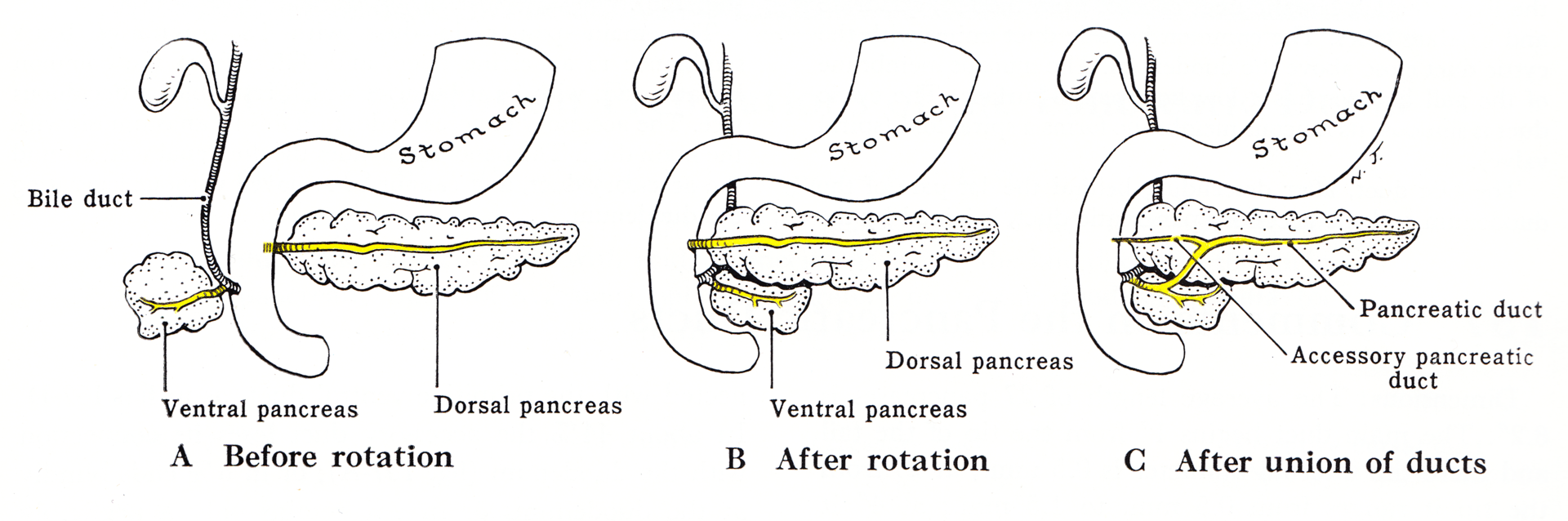
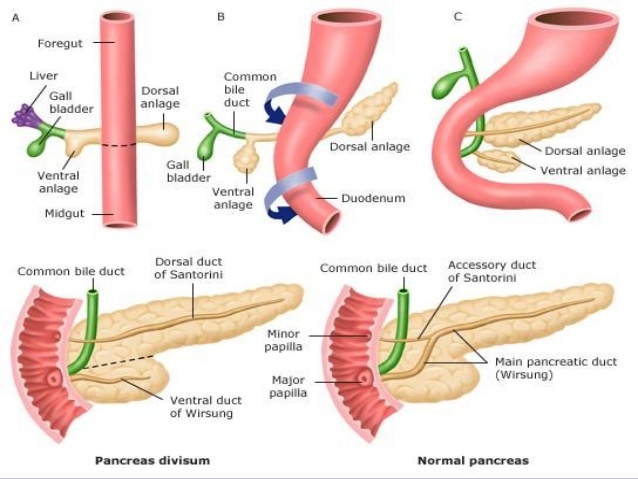
Definition – portion of the dorsal duct distal to the dorsal-ventral fusion point during embryonic development
Clinical Significance – 85% of the population have a single, main pancreatic duct and 15% can have an accessory duct that either drains into the duodenum by a separate ampulla (2/3), or drains into the main duct (1/3). These anatomical variants need to be explored prior to instrumentation for pancreatic pathology as it can occur with pancreas divisum, which makes the accessory duct the principle drainage duct for the pancreas.
History – Named after Giovanni Domenico Santorini (1681-1737), who was an Italian anatomist and son of an apothecary. He spent his formative years studying medicine throughout Bologna, Padua, and Pisa, where he received his medical doctorate in 1701. He performed anatomical dissection demonstration in Venice for 23 years, during which he published his most famous work entitled Observationes Anatomicae. This work was considered one of the most detailed and important anatomical texts of the time and gave way to descriptions of twelve different anatomic eponyms accredited to Santorini.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
The term “celiac” has Latin and Greek roots as Aretaeus of Cappadocia named this disease in the 1st century AD “koiliakos” meaning abdomen/abdominal in patients with chronic diarrhea. The first modern medical description of the disease was in 1888 by Samuel Gee in an paper entitled “On the Coeliac Affection”. The specific medical term for Celiac Disease is “gluten-sensitive enteropathy”. It was still relatively unexplained until Willem Dicke, a Dutch pediatrician, noted improvement in his patient’s abdominal symptoms during bread and grain shortages of World War II.
Epidemiology
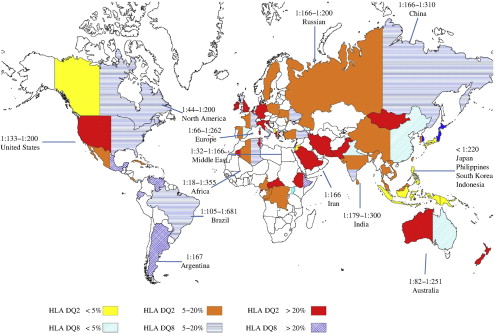
Primarily in northern European white
Prevalence is widely variable due to differing rates and types of population screening throughout the world
Pathophysiology
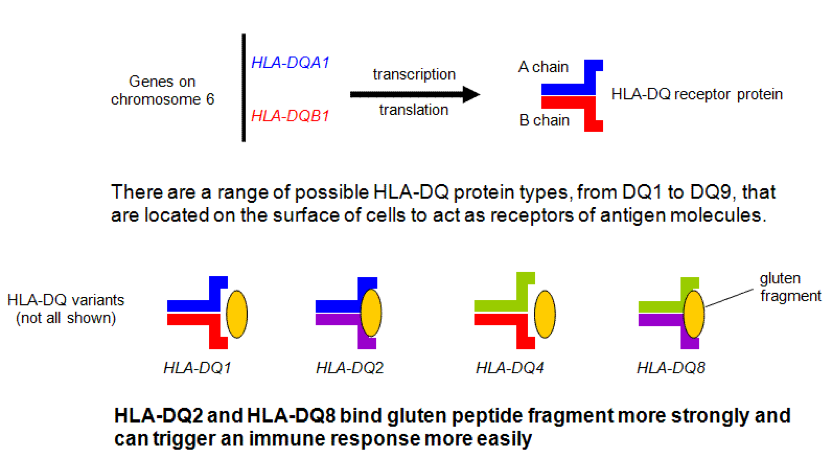
High association with genetic predisposition to gluten sensitivity, specifically HLA-DQ2 and/or DQ8, and because of these genetic changes, serum autoantibodies are produced that attack the endomysium of the enterocytes of the small bowel.
Signs and Symptoms
Originally thought to be a disease of infancy, it is being
diagnosed later and later in life, with adults first being diagnosed as late as
the fifth decade. Often, this is in the
setting of failure to thrive in an infant.
Common
Diarrhea
Steatorrhea
Malabsorption
Anemia (iron), weight loss,
metabolic bone disease (vitamin D and calcium), vitamin deficiencies (B-complex
vitamins)
Peripheral neuropathy, ataxia
Associated Clinical Findings
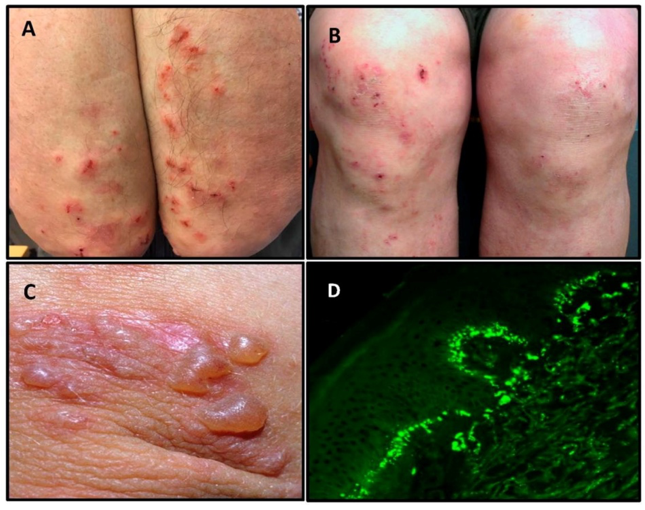
Dermatitis herpetifomis
Pruritic papules and grouped
vesicles on the elbows, forearms, knees, scalp, back, and buttock.
1:369 patients diagnosed with celiac
disease
Diagnosed with biopsy histologic
evidence of IgA deposition in basement membrane
Down Syndrome
As high as 16% association, which isa 20-fold increase compared with general public
Also associated with liver disease, diabetes, thyroid disease, inflammatory bowel disease
Screening and Diagnosis
Who should be screened?
Patients with chronic diarrhea,
malabsorption, weight loss, or abdominal distension and bloating
Patients without other explanations
for extraintestinal diseases such as anemia, elevated transaminases, peripheral
neuropathy, ataxia, etc.
Patients with type 1 DM and signs or
symptoms of celiac disease
Asymptomatic first-degree relatives
of patients with confirmed celiac disease
Immunoglobulin A (IgA) anti-tissue
transglutaminase (TTG) is the initial screening test of choice
If positive, then proceed with
duodenal biopsy via endoscopy
If negative, HLA-DQ2/DQ8 testing is
performed to evaluate for nonceliac gluten sensitivity
If negative, then celiac is
ruled-out
If positive, then slow introduction
of gluten-containing foods is started
If unable to tolerate, then proceed
with biopsy
If serology changes to positive,
then celiac disease is confirmed
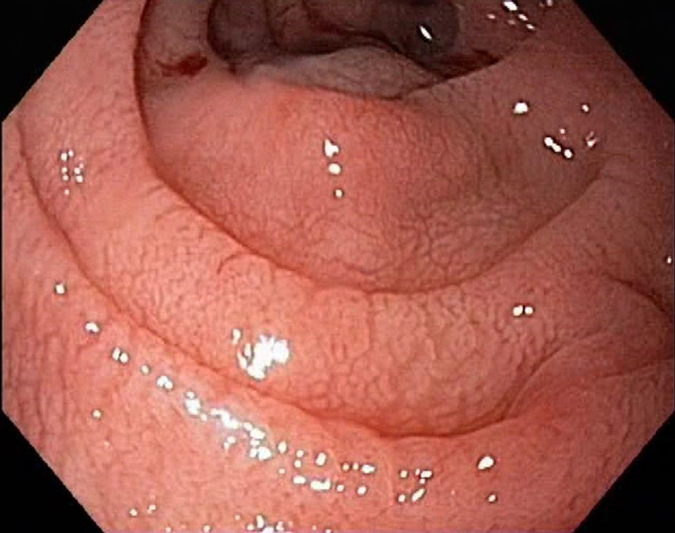
Endoscopic biopsy is the confirmatory
test of choice in patients with positive serologic screening and high
probability of celiac disease.
Duodenal mucosa may appear atrophic
with loss of folds, visible fissures, nodular folds, and/or scalloped
appearance
Histologic features of small bowel
biopsy include increased intraepithelial lymphocytes, flat mucosa with complete
loss of villi and atrophy, and/or crypt hyperplasia
Classification
Celiac disease can present as a spectrum of signs and
symptoms and thus, have different classifications.
Classic Disease
3 key features
Villous atrophy
Symptoms of malabsorption
Steatorrhea, weight loss, nutrient
deficiencies
Improvement in symptoms with
withdrawal of gluten-containing foods
Atypical Disease
Minor gastrointestinal complaints
Anemia, osteoporosis, tooth enamel
issues,
Severe mucosal damage is present on
endoscopy
Asymptomatic (Silent) Disease
Incidental finding on screening
without symptoms
Management
Six key elements of successful management of celiac disease
and it has a nice acronym:
Consultation with a skilled dietician
Education about the disease
Lifelong adherence to a gluten-free diet
Identification and treatment of nutritional deficiencies
Access to an advocacy group
Continuous long-term follow-up by a multidisciplinary team
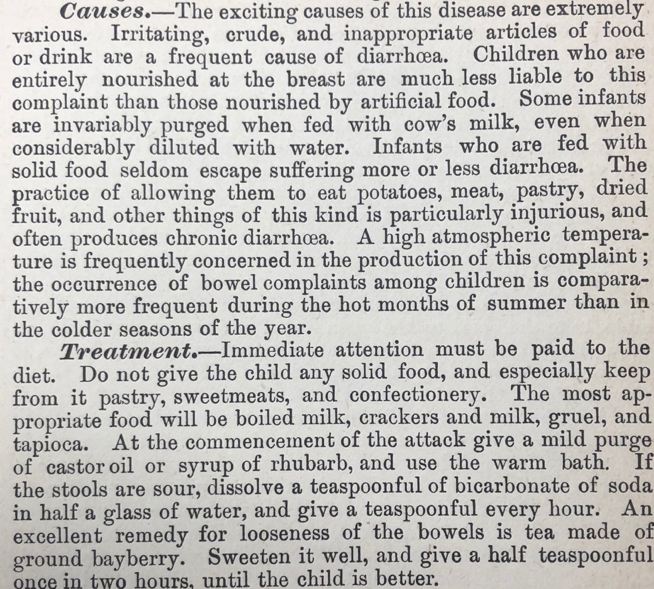
Cottage Physician
This is an excerpt from the pediatric disease section on diarrhea:
References
Impact – A Publication of the University of Chicago Celiac Disease Center. 2007;7(3):1-3. [article]
Yan D, Holt PR. Willem Dicke. Brilliant clinical observer and translational investigator. Discoverer of the toxic cause ofceliac disease. Clinical and translational science. 2009; 2(6):446-8. [pubmed]
Schuppan D. Current concepts of celiac disease pathogenesis. Gastroenterology. 2000; 119(1):234-42. [pubmed]
Kagnoff MF. Celiac disease. A gastrointestinal disease with environmental, genetic, and immunologic components.Gastroenterology clinics of North America. 1992; 21(2):405-25. [pubmed]
Dieterich W, Laag E, Schöpper H, et al.Autoantibodies to tissue transglutaminase as predictors of celiac disease.Gastroenterology. 1998; 115(6):1317-21. [pubmed]
Bibbins-DomingoK, Grossman DC, et al. Screening for Celiac Disease: US Preventive Services Task Force Recommendation Statement. JAMA. 2017; 317(12):1252-1257. [pubmed]
CarlssonA, Axelsson I, Borulf S, et al. Prevalence of IgA-antigliadin antibodies and IgA-antiendomysium antibodies related to celiac disease in children with Down syndrome. Pediatrics. 1998; 101(2):272-5. [pubmed]
Rubio-TapiaA, Hill ID, Kelly CP, Calderwood AH, Murray JA, . ACG clinical guidelines:diagnosis and management of celiac disease. The American journal of gastroenterology. 2013; 108(5):656-76; quiz 677. [pubmed]
ShahVH, Rotterdam H, Kotler DP, Fasano A, Green PH. All that scallops is not celiac disease. Gastrointestinal endoscopy. 2000; 51(6):717-20. [pubmed]
OberhuberG, Granditsch G, Vogelsang H. The histopathology of coeliac disease: time for astandardized report scheme for pathologists. European journal of gastroenterology & hepatology. 1999; 11(10):1185-94. [pubmed]
National Institutes of Health Consensus Development Conference Statement on Celiac Disease, June 28-30, 2004.Gastroenterology. 2005; 128(4 Suppl 1):S1-9. [pubmed]
Definition – This is the main pancreatic duct that joins the pancreas to the common bile prior to the ampulla of Vater before emptying into the second portion of the duodenum
Clinical Significance – Having a single, major pancreatic duct is the most common anatomic variant for pancreatic anatomy, but some individuals may have an accessory duct that could be functional. The issue with this, of course, is management of pancreatic pathology so imaging may be required prior to instrumentation or surgical management.
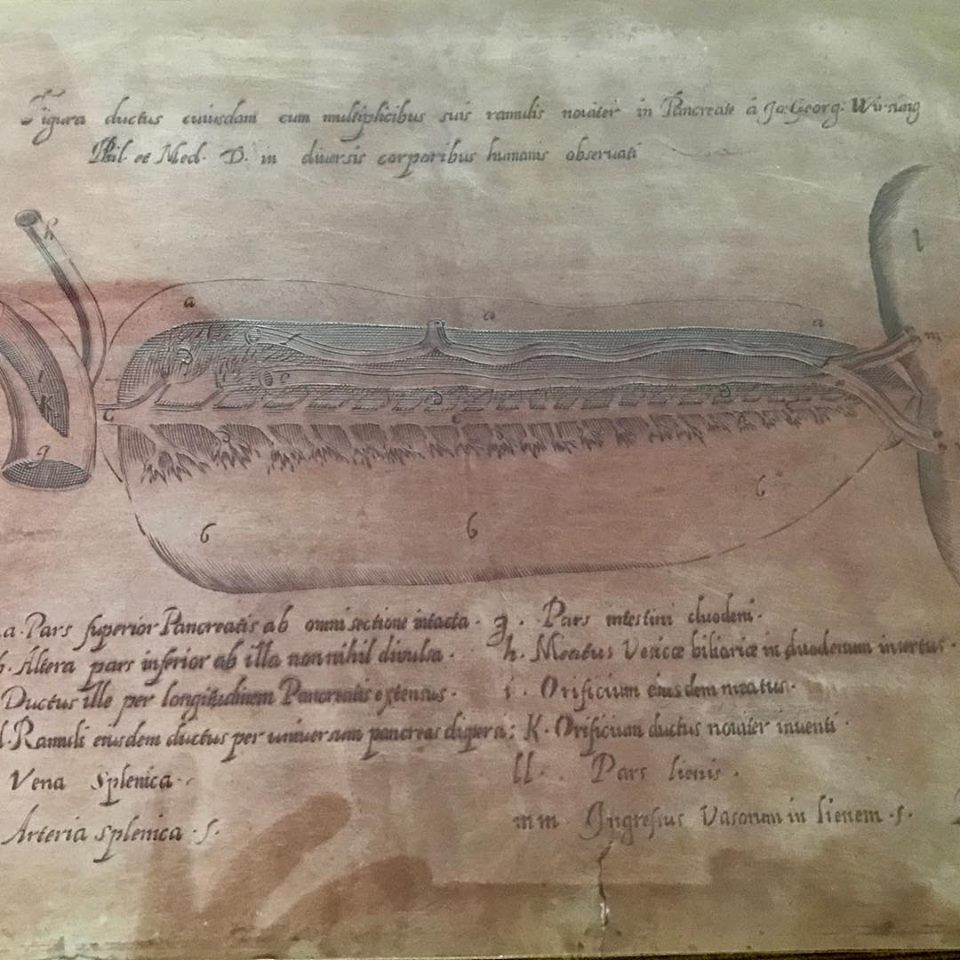
History – Named after Johann Georg Wirsung (1589-1643), who was a German anatomist from Padua. He made this discovery while dissecting a criminal (Zuane Viaro) who was recently hanged for murder in 1642. Instead of formally publishing his findings, he engraved the sketch on a copper plate so numerous casting could be made and sent to the leading anatomists of the time. This finding is not without controversy. One year after this discovery, Wirsung was murdered in his house late at night by a Belgian student named Giacomo Cambier over a quarrel of first discovered this duct. In a cruel twist of fate, 5 years after his death, one of Wirsung’s students who was assisting in the dissection, Moritz Hoffman, claimed it was he who discovered this duct in a turkey rooster a year before Wirsung.
Original copper plate etchingPainting of the murder of Wirsung
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Howard JM, Hess W, Traverso W. Johann Georg Wirsüng (1589-1643) and the pancreatic duct: the prosector of Padua, Italy. Journal of the American College of Surgeons. 1998; 187(2):201-11. [pubmed]
What vitamins have a higher potential for causing toxicity and why?
Answer
Fat soluble vitamins can be stored in the adipose tissue instead of excreted if in excess. As a result, vitamins A, D, E, and K can cause toxicity if patients take too much (in this order of incidence as well).
Hypervitamintosis A can result in ataxia, hepatotoxicity, visual impairments, and orange skin.
Hypervitamintosis D can result in hyperphosphatemia and hypercalcemia.
Hypervitamintosis E can block vitamin K absorption and leads to easy bleeding and bruising
Hypervitamintosis K is very rare and really only seen in infants receiving newborn injections after birth.
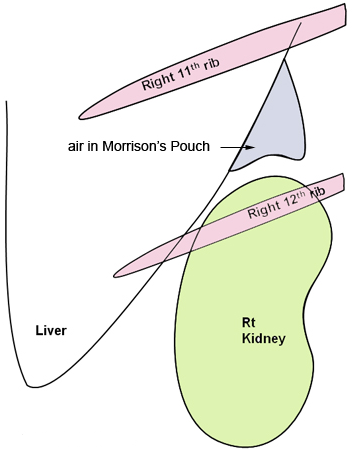
Other known aliases – hepatorenal recess/fossa, right posterior subhepatic space
Definition – a potential space between the liver and the right kidney
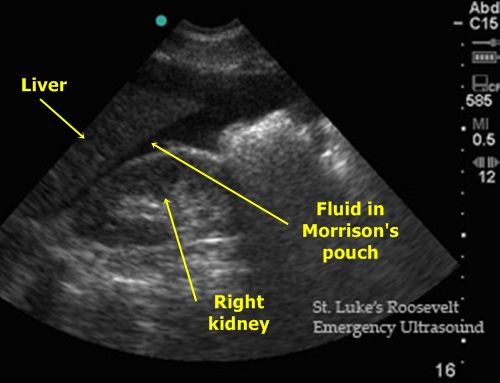
Clinical Significance – This a space where fluid can accumulate in the setting of ascites or abdominal trauma and be seen on CT or ultrasound. It is one of the view of a Focused Assessment of Sonography in Trauma (FAST) exam. Typically, 30-40mL of fluid needs to be present to be visualized.
Ultrasound
Computed Tomography
History – Named after James Rutherford Morison (1853-1939), a British surgeon who received his medical degree from the University of Edinburgh in 1874. He was also an assistant and “surgical dresser” for Joseph Lister early in his career and later founded a school of surgery at the University of Durham where he made his name as a prolific instructor of surgery. He is well known as a pioneer of modern surgery with several of his contemporaries noting he was twenty years ahead of his time and was a driving force of he surgical arts in Great Britain at the turn of the 20th century.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Definition – sac-like outpouching of the mucosa and submucosa through Killian’s triangle, which is the area of structural weakness between the cricopharyngeus and lower inferior constrictor muscles.
Clinical Significance – There are actually three different types of diverticulae that can form in this region and are based on anatomic location:
Zenker’s – immediately above the upper esophageal sphincter
Traction – near midpoint of the esophagus
Epiphrenic – immediately above the lower esophageal sphincter
Signs and symptoms of a Zenker’s diverticulum are pretty awful and include dysphagia, pulmonary aspiration, and halitosis from partially rotting food in the outpoaching. It is diagnosed via barium swallow under flouroscopy. The majority of the patients are male and present after the age of 60. Management is surgical resection.
History – Named after Friedrich Albert von Zenker (1825-1898), who was German physician and pathologist and received his medical doctorate at Leipzig in 1851. He held numerous teaching posts including chief prosector and professor of general pathology and anatomy at Dresden city hospital. Dr. Zenker, along with Hugo Wilhelm von Ziemssen, published a case series and literature review on his eponymous diverticulum in 1867 entitled “Krankheiten des Oesophagus”. He also was the first to document and describe trichinosis in a girl who died in 1860, proving that the once thought harmless parasite could cause severe disease.
Friedrich Albert von Zenker
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
F. A. Zenker and Hugo Wilhelm von Ziemssen: Krankheiten des Oesophagus. Leipzig, 1867
Ueber die Trichinenkrankheit des Menschen. Virchows Archiv für pathologische Anatomie und Physiologie und für klinische Medizin, Berlin, 1860, 18: 561-572.