Frégoli Delusion
Other Known Aliases – delusion of doubles
Definition – mistaken belief that some person currently present in the deluded person’s environment (typically a stranger) is a familiar person in disguise.
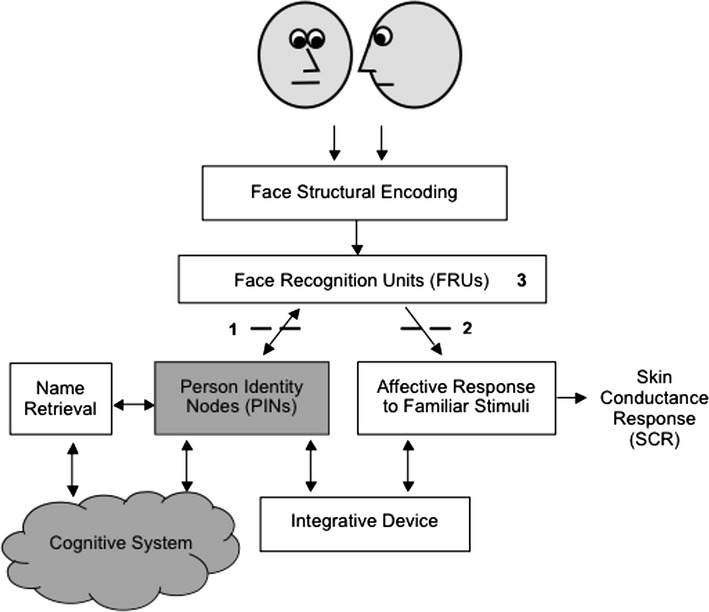
Clinical Significance – to the patient, the stranger is believed to be psychologically identical to this known person (who is not present) even though the deluded person perceives the physical appearance of the stranger as being different from the known person’s typical appearance. There are 4 subtypes:

History – this syndrome was first published in 1927 by Courbon and Fail who describe a case of a young woman who believed she was being pursued by two Parisian actresses in disguise. They named this delusional syndrome after Leopoldo Frégoli, who was an Italian stage actor with an extraordinary ability to impersonate and mimic others on stage.



References
- Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
- Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
- Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
- Whonamedit – dictionary of medical eponyms. http://www.whonamedit.com
- Up To Date. www.uptodate.com
- Langdon, R., Connaughton, E. and Coltheart, M. The Fregoli Delusion: A Disorder of Person Identification and Tracking. Top Cogn Sci. 2014;6:615-631.
- Courbon, P., & Fail, G. (1927). Syndrome d”‘illusion de Frégoli” et schizophrénie [Syndrome of the “illusion of Fregoli” and schizophrenia]. Bulletin de la Société Clinique de Médecine Mentale, 20, 121–125