What are the 5 main life-threatening causes of chest pain?



What are the 5 main life-threatening causes of chest pain?

Other Known Aliases – Inguinal triangle, medial inguinal fossa
Definition – Anatomical region of the abdominal wall outlined by the boundaries of the lateral margin of the rectus sheath, the inferior epigastric vessels, and the inguinal ligament.

Clinical Significance – The area is where direct hernias protrude through the abdominal wall.

History – Named after Franz Kasper Hesselbach (1759-1816), who was a German physician, surgeon, and anatomist in Hammelburg, Germany. He had a prolific career surgical assistant and prosector under Karl Kasper von Siebold at The Juliusspital in Würberg, before obtaining his doctor of medicine there. He is best known for his contributions to the surgery of hernias and has several other eponyms as well: Hesselbach’s fascia (cribriform fascia) and Hesselbach’s ligament (interfoveolar ligament.
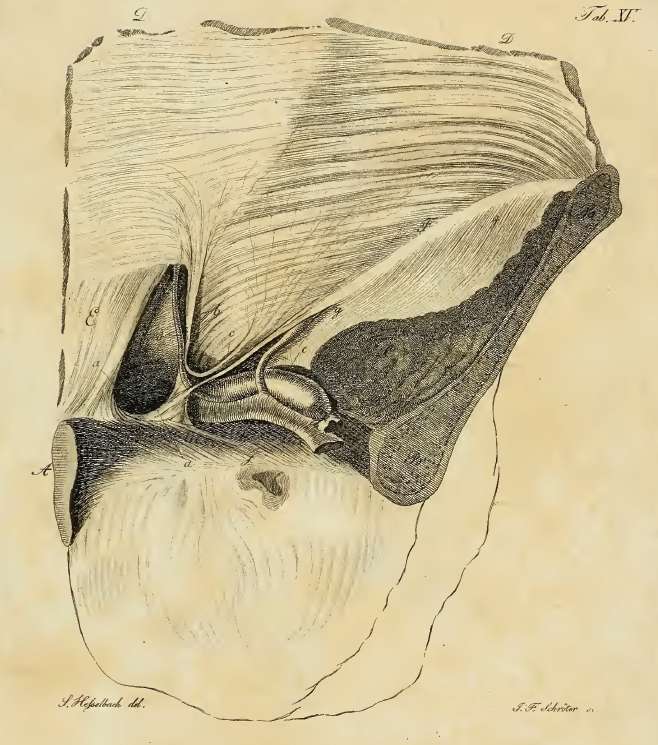
From his 1806 manuscript
References
What are the some of the pancreatitis scoring systems that are commonly used to estimate severity and mortality?
There are several scoring systems for estimating severity and mortality in pancreatitis.
References
Other Known Aliases – Moynihan’s Method (using just the thumb with patient supine)
Definition – Inspiratory arrest with deep palpation in the right upper quadrant
Clinical Significance – As the patient exhales, the abdominal organs move cephalad and under the diaphragm. After full exhalation and during inspration, the organs move caudal back into the abdominal cavity. When there is inflammation of the gallbladder, the patient will stop inhaling as the inflammed gallbladder touches the practitioner’s fingers during deep palpation of the right upper quadrant.
History – Named after John Benjamin Murphy (1857-1916), who was an American surgeon and early pioneer for many different surgical operations and techniques. In fact, William James Mayo (co-founder of The Mayo Clinic) called him “the surgical genius of our generation”.
In 1889, he advocated for and popularized early appendectomy in all suspected appendicitis cases and had over 200 successful cases to begin convincing his colleagues of the benefits of early surgery. Dr. Murphy also pioneered treatment of tuberculosis with iatrogenic pneumothoraces and was the first surgeon to re-anastomose a transected femoral artery from a gunshot wound. He was also a distinguished teacher and developed “wet clinics” at Mercy Hospital, where he operated and lectured to an audience of learners in a traditional operative theater.

Dr. Murphy also attended to Theodore Roosevelt after an assassination attempt and was one of the founding members of the American College of Surgeons. He is also the author of one of the more famous quotes pertaining to patient-centered care.

References
What are the some of the pancreatitis scoring systems that are commonly used to estimate severity and mortality?
Definitions
Epidemiology
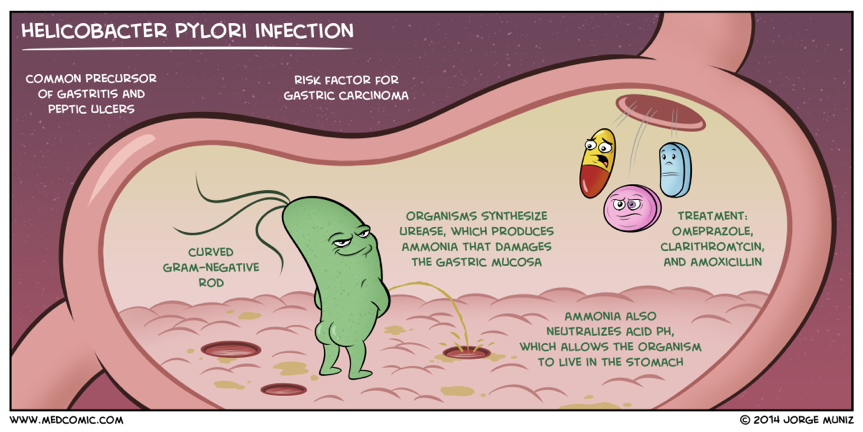
Etiologies
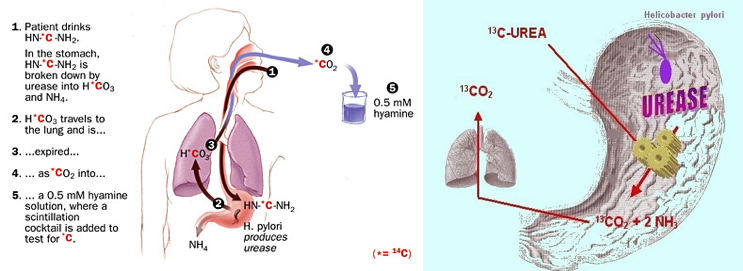
There are numerous causes of PUD and include infections, stress, medications, alcohol, cirrhosis, neoplasms, etc. The two main causes in developed countries are:

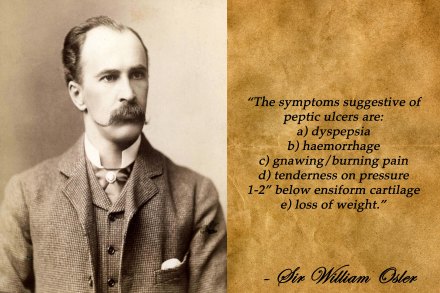
Clinical Manifestations

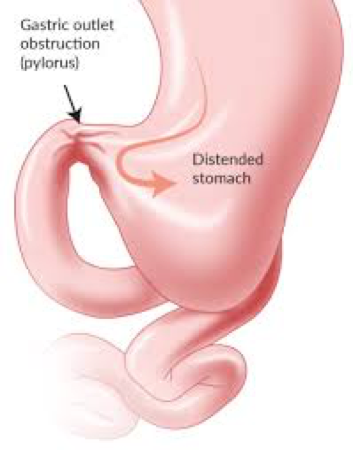
Complications
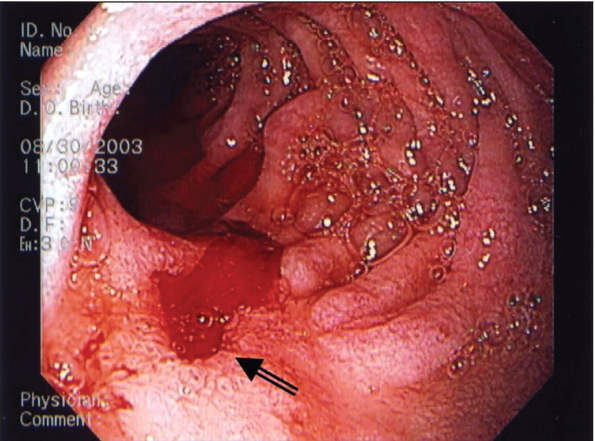


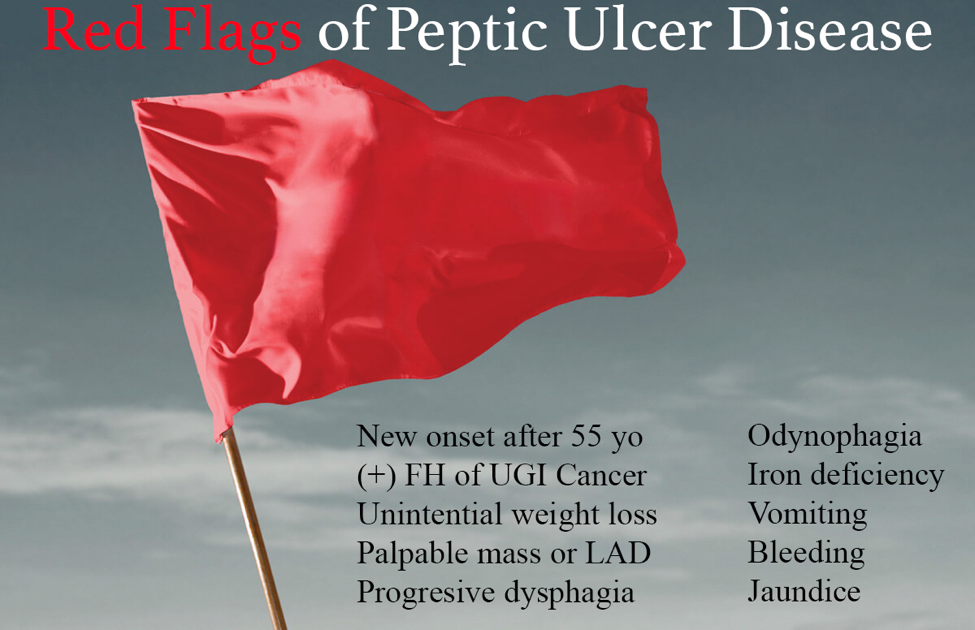
Red Flags
Work-up
Initial Management


References
Other Known Aliases – none
Definition – Hernia involving a Meckel’s diverticulum
Clinical Significance – No real clinical significance other than it is an extremely rare type of hernia, but is always included in the typical pimping barrage of surgery students. It should also be included in the “zebras” of differential diagnoses of RLQ pain.


History – Named after Alexis Littrè (1654-1726), who was a distinguished physician and prolific surgeon at the historic Salpêtriére Teaching Hospital in Paris. He was inducted into the famed Académie des Sciences in part to his ridiculous dissection of over 200 cadavers in 1684. He first described an femoral hernia involving an intestinal diverticulum in 1700 in one of his cadaver dissections.
References

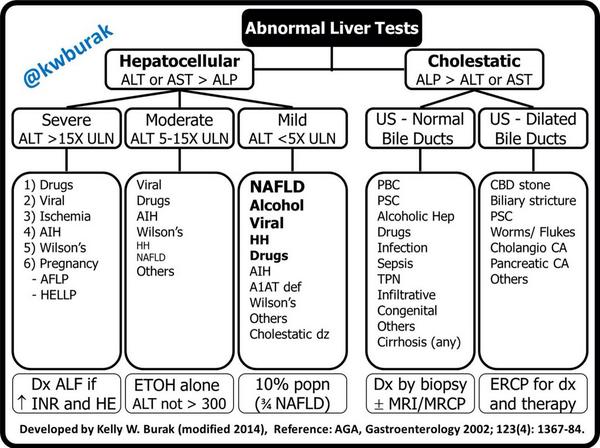
There are many individual lab tests that encompass “liver function tests” or LFTs. So for this week’s pearl:
Now let me make this clear, there is MUCH MORE that goes into interpreting LFTs, but this is good, quick start when you get abnormal LFTs back on your patient.
References
Other Known Aliases – none
Definition – Vestigial remnant of the omphalomesenteric duct
Clinical Significance – It is the most common malformation in the GI tract and is mainly asymptomatic. When symptoms do occur, it commonly presents as painless, rectal bleeding in children. The “Rule of 2s” will help you remember the facts of this pathology:


History – Named after Johann Friedrich Meckel, the Younger (1781-1833), who was born into a prestigious medical family, with his father and grandfather already prolific physicians and professors of medicine in Halle, Prussia. He made tremendous advancements in the area of anatomy and embryonic development with special attention to birth defects and abnormalities, where he pioneered the early study of teratology. He first described the abnormality which bears his name in 1809.

References
There are many individual lab tests that encompass “liver function tests” or LFTs. So for this week’s pearl:
