We all know that nutritional supplementation during pregnancy is extremely important for fetal development. But…….there is one particular vitamin that can be teratogenic in excess doses.
What vitamin is this?
What types of foods are extremely high in this vitamin and why?
Question
The class of retinoic acids have two main forms of vitamin A:
Provitamin A – primarily plant based carotenoids
green leafy vegetables, sweet potatoes, carrots
Preformed vitamin A – primarily in animal sources
livers, kidneys
Up to 85% of metabolized vitamin A is stored in the liver and other tissues due to being fat soluble. As a result, animal organs (liver, kidneys, thymus) are extremely high in preformed vitamin A and can cause acute and/or chronic toxicity when ingested in large quantities.
References
Rothman KJ, Moore LL, Singer MR, Nguyen UD, Mannino S, Milunsky A. Teratogenicity of High Vitamin A Intake N Engl J Med. 1995; 333(21):1369-1373.
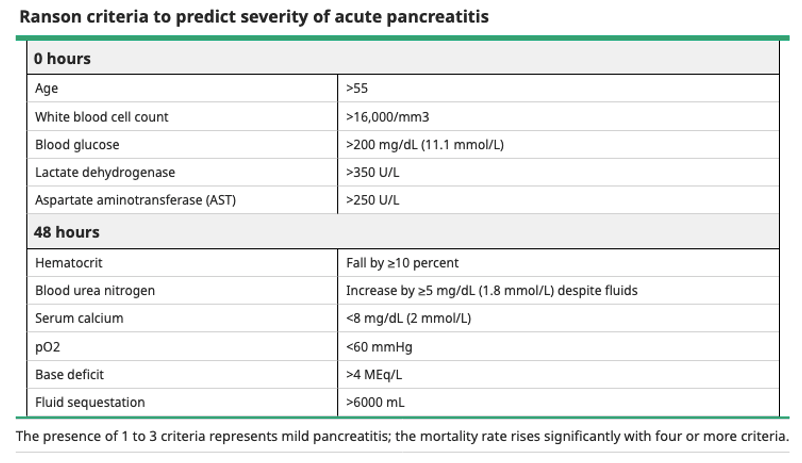
Definition – clinical decision instrument to predict mortality of acute pancreatitis on admission and after the first 48 hours
Clinical Significance – this was one of the first instruments to help with the initial management of patients with acute pancreatitis. Now, it has been largely been replaced by more accurate and reliable calculations and is taught only for historical purposes.
History – Named after John H. C. Ranson (1938-1995), an English-American surgeon who received his medical doctorate from Oxford University in 1960. He would complete his surgical residency at Bellevue Hospital and New York University Medical Center, where he would join as faculty and later as the Director of the Division of General Surgery. He would have a prolific career primarily focusing on the alimentary tract with concentration on the pancreas. He would publish his eponymous scoring system in 1974 which not only improved the clinical care of patients with pancreatitis, but also improved the quality of the research by finally being able to compare severity groups of treatment arms.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Reber HA. Obituary – John H. C. Ranson, Pancreas: April 1996 – Volume 12 – Issue 3 – p 215 [link]
Ranson JH, Rifkind KM, Roses DF, Fink SD, Eng K, Spencer FC. Prognostic signs and the role of operative management in acute pancreatitis. Surg Gynecol Obstet. 1974;139(1):69-81. [link]
We all know that nutritional supplementation during pregnancy is extremely important for fetal development. But…….there is one particular vitamin that can be teratogenic in excess doses.
What vitamin is this?
What types of foods are extremely high in this vitamin and why?
Definition –metaplastic change of the mucosal cells of the lower esophagus from normal stratified squamous epithelium to simple colunar epithelium and interspaced goblet cells
Clinical Significance – these histologic changes are premaligant and significantly increases a patient’s risk for developing esophageal adenocarcinoma.
History – Named after Norman Rupert Barrett (1903-1979), an Australian-born British thoracic surgeon who received his medical doctorate from Trinity College, Cambridge. He would practice his entire career at St. Thomas Hospital, with a brief training period in 1935-1936 when he traveled to the US on a Rockfeller Traveling Fellowship. It was here that he decided to pursue thoracic surgery instead of GI surgery. In 1947, he performed the first successful surgical repair of a ruptured esophagus. He would publish his eponymous findings of histologic changes of the distal esophagus in 1950, but erroneously believed this was due to congenitally shortened esophagus with a portion of the stomach trapped in the chest. Allison and Johnstone were the first to argue that these changes were esophagus, not stomach, and termed these ulcers “Barrett’s ulcers”. Of note, Allison first described this condition in 1948 before Barrett’s publication.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Can reintroduce within 24 hours if no nausea, vomiting, and decreasing pain and inflammatory markers
Start with low-residue, low fat, soft diet and advance as tolerated
Supplemental nutrition generally needed for moderately severe and severe cases, or if unable to tolerate oral nutrition within 5 days
Enteral > parental with placement of jejunal feeding tube beyond the ligament of Treitz
Helps prevent bacterial translocation
Parenteral is indicated if nutritional goals are not achieved with 48-72 hours due to pain or intolerance
Consult your hospital nutritional team and/or dietician for help
Antibiotics
No evidence to support prophylactic antibiotics
Most infected necroses will occur late in clinical course (5-10 days after admission)
Treat underlying causes
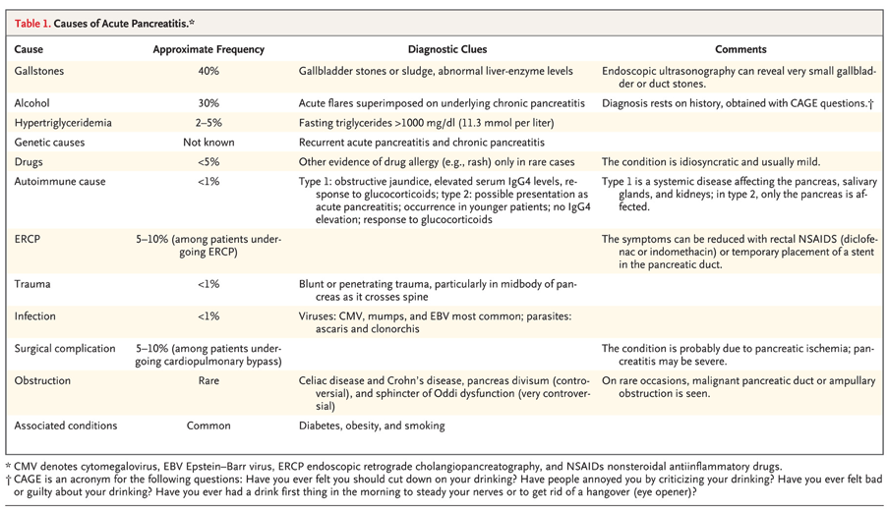
Gallstone pancreatitis
ERCP should be performed within 24 hours of admission
Cholecystectomy should be performed within 7 days and often during same hospitalization
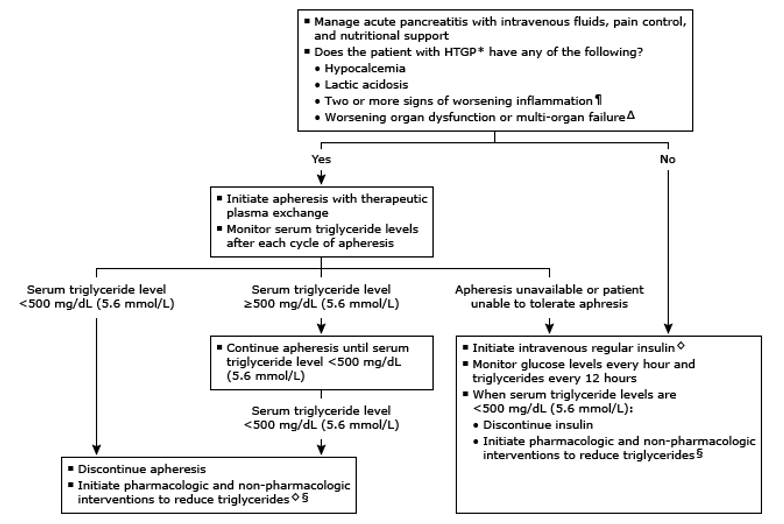
Hypertriglyceridemia
Therapeutic plasma exchange and insulin therapy
Complications
Necrosis
Pseudocyst
Splanchnic venous thrombosis
References
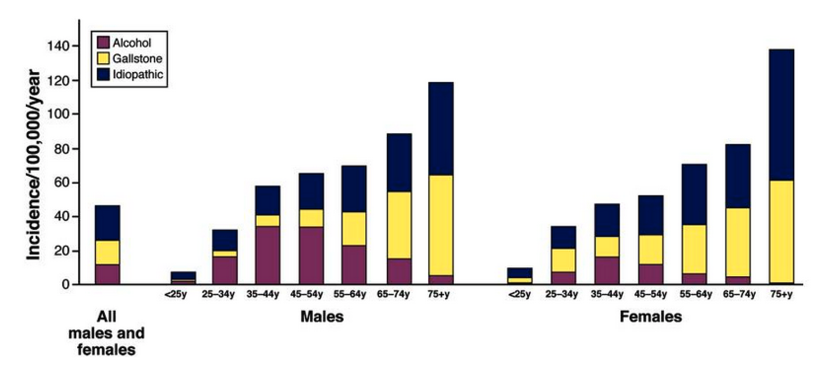
Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology. 2013; 144(6):1252-61. [PDF]
Conwell DL, Banks PA, Greenberger NJ. Acute and Chronic Pancreatitis. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 20e. McGraw-Hill;
Mechanisms of alcoholic pancreatitis. Proceedings of a conference. Chicago, Illinois, USA, November 2002. Pancreas. 2003; 27(4):281-355. [pubmed]
Nawaz H, Koutroumpakis E, Easler J, et al. Elevated serum triglycerides are independently associated with persistent organ failure in acute pancreatitis. Am J Gastroenterol. 2015; 110(10):1497-503. [pubmed]
Scherer J, Singh VP, Pitchumoni CS, Yadav D. Issues in hypertriglyceridemic pancreatitis: an update. J Clin Gastroenterol. 2014; 48(3):195-203. [PDF]
Kahaleh M, Freeman M. Prevention and management of post-endoscopic retrograde cholangiopancreatography complications. Clin Endosc. 2012; 45(3):305-12. [PDF]
Lankisch PG, Dröge M, Gottesleben F. Drug induced acute pancreatitis: incidence and severity. Gut. 1995; 37(4):565-7. [PDF]
Forsmark CE, Swaroop Vege S, Wilcox CM. Acute Pancreatitis N Engl J Med. 2016; 375(20):1972-1981.
Yadav D, Agarwal N, Pitchumoni CS. A critical evaluation of laboratory tests in acute pancreatitis. Am J Gastroenterol. 2002; 97(6):1309-18. [pubmed]
Wu BU, Johannes RS, Sun X, Tabak Y, Conwell DL, Banks PA. The early prediction of mortality in acute pancreatitis: a large population-based study. Gut. 2008; 57(12):1698-703. [pubmed]
Vege SS, DiMagno MJ, Forsmark CE, Martel M, Barkun AN. Initial Medical Treatment of Acute Pancreatitis: American Gastroenterological Association Institute Technical Review. Gastroenterology. 2018; 154(4):1103-1139. [pubmed]
Basurto Ona X, Rigau Comas D, Urrútia G. Opioids for acute pancreatitis pain. Cochrane Database Syst Rev. 2013; [pubmed]
Casaer MP, Mesotten D, Hermans G, et al. Early versus late parenteral nutrition in critically ill adults. N Engl J Med. 2011; 365(6):506-17. [pubmed]
Kutsogiannis J, Alberda C, Gramlich L, et al. Early use of supplemental parenteral nutrition in critically ill patients: results of an international multicenter observational study. Crit Care Med. 2011; 39(12):2691-9. [pubmed]
Aboulian A, Chan T, Yaghoubian A, et al. Early cholecystectomy safely decreases hospital stay in patients with mild gallstone pancreatitis: a randomized prospective study. Ann Surg. 2010; 251(4):615-9. [pubmed]
Uhl W, Müller CA, Krähenbühl L, Schmid SW, Schölzel S, Büchler MW. Acute gallstone pancreatitis: timing of laparoscopic cholecystectomy in mild and severe disease. Surg Endosc. 1999; 13(11):1070-6. [pubmed]
Ipe TS, Pham HP, Williams LA 3rd. Critical updates in the 7 edition of the American Society for Apheresis guidelines. J Clin Apher. 2018; 33(1):78-94. [pubmed]
47yo man presents to the emergency department after an episode of hematemesis at the end of a 2 day alcoholic binge. He reports drinking 1-3 handles of vodka over the weekend after his 14 consecutive day, third shift schedule every month at the local manufacturing plant. He reports moderate central chest pain, but denies shortness of breath. Vitals are BP-110/82 mmHg, HR-112, RR-14, O2-98%, and temp-99.2o. Physical exam is unremarkable, hemoccult is negative, and labs are below.
What are the three (3) main differentials you need to consider?
What is the most likely diagnosis based on exam and labs?
The most likely of these is Mallory-Weiss tear. The unremarkable physical exam points away from Boerhaave’s as patients most commonly present with mediastinitis and, in some instances, sepsis. Other physical examination findings of Boerhaave’s include subcutaneous emphysema of the neck with crepitus and Hamman’s sign of medisatinal crunch on auscultation. Varices can self-tamponade after an acute bleed, but given the patient’s hemodynamic status being stable with a normal H/H and negative hemoccult also move this down the differential list.
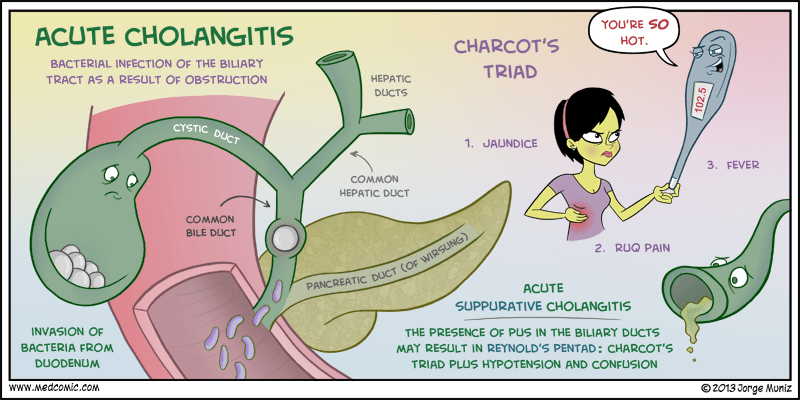
Definition – triad of physical examination findings seen with ascending cholangitis and includes jaundice, fever, and right upper quadrant pain.
Clinical Significance – this is a classic triad to memorize for your surgery rotation to help differentiate cholecystitis, cholelithiasis, and cholangitis.
History – Named after Jean-Martin Charcot (1825-1893), a French neurologist and professor of anatomic pathology who recieved his medical doctorate from the University of Paris in 1853. He would start his career at the famous Hôpital de Salpêtrière and stay there for over 30 years establishing the reputation of this hospital as the premier training center in Europe. He would also create the first neurology clinic in all of Europe at the Salpêtrière where his reputation would be solidified as the “father of modern neurology”. His career is too prestigious to give it justice in a quick eponym review, as evidenced by at least 15 current eponyms bearing his name.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
47yo man presents to the emergency department after an episode of hematemesis at the end of a 2 day alcoholic binge. He reports drinking 1-3 handles of vodka over the weekend after his 14 consecutive day, third shift schedule every month at the local manufacturing plant. He reports moderate central chest pain, but denies shortness of breath. Vitals are BP-110/82 mmHg, HR-112, RR-14, O2-98%, and temp-99.2o. Physical exam is unremarkable, hemoccult is negative, and labs are below.
What are the three (3) main differentials you need to consider?
What is the most likely diagnosis based on exam and labs?
Other Known Aliases – end-to-end surgical anastomosis
Definition – gastrointestinal tract is divided into two limbs (proximal, Roux limb and a distal limb) and are re-anastomosed farther down the GI tract, typically in the jejunum
Clinical Significance – this type of surgery is the traditional form of gastric bypass, where the proximal, Roux limb serves as the food reservoir and somach and the distal limb allows for physiologic drainage of gastric, hepatic, and pancreatic enzymes to aid in digestion. Other conditions it can be used is are chronic pancreatitis, alkaline gastritis, and various GI substitution procedures.
History – Named after César Roux (1857-1934), who was a Swiss surgeon and received his medical doctorate from the University of Bern 1880. He would stay on at his alma mater and assist Theodor Kocher until 1887, when he became chief of surgery at cantonal hospital of Lausanne. He would go on to have a modest career in surgery notable for two historical accomplishments. In 1893, he performed his eponymous procedure on a patient with gastric strictures from peptic ulcer disease to alleviate his obstruction symptoms. In 1926, the year of his retirement, he was the first surgeon to successfully remove a pheochromocytoma….7 months before Charles Mayo performed the same operation in the United States. Harvey Cushing visited his clinic in 1900 and said “he is a rough diamond-looks like Kipling-does excellent work and comes nearer to being the kind of man I am looking for than anyone else I have seen”.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
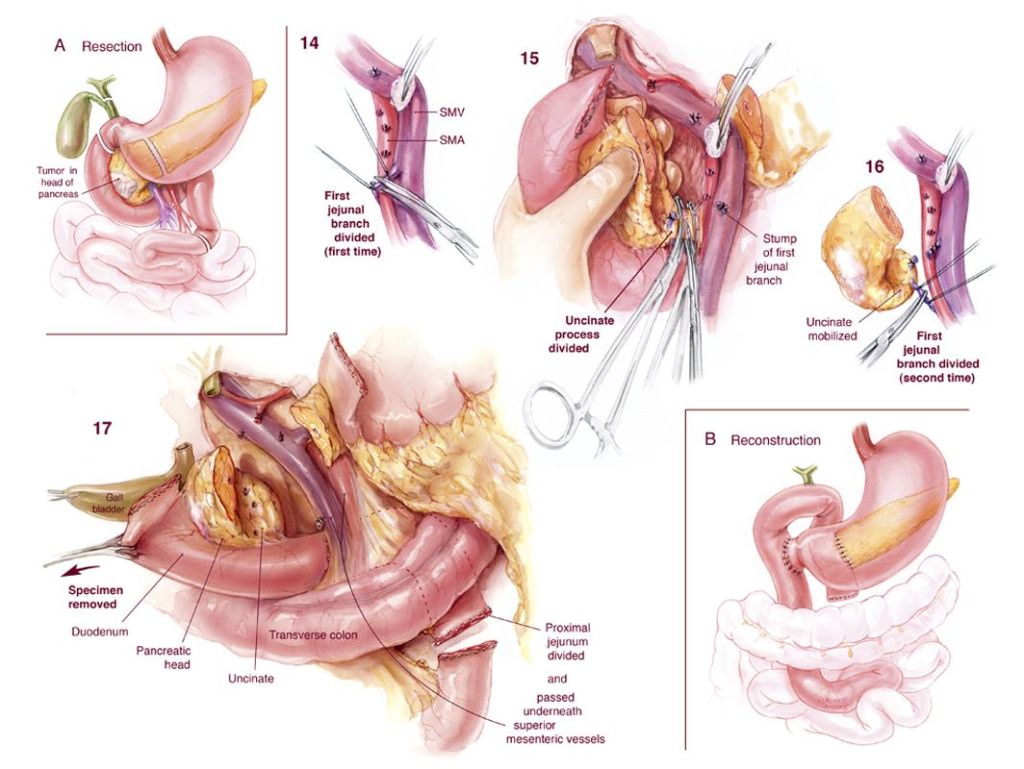
Definition – pancreaticoduodenectomy cholecystectomy, choledochojejunostomy, pancreaticojejunostomy, and gastrojejunostomy
Clinical Significance – this type of surgery is performed to resect pancreatic head tumors. It generally performed at large, high-volume medical centers as this has been shown to reduce mortality to less than 5%. An experienced surgeon can complete this surgery in < 6 hours with < 500mL of blood loss. Barring any postoperative complications, most patients are discharged from the hospital in 7-10 days.
History – Named after Allen Oldfather Whipple (1881-1963), who was an American surgeon and received his medical doctorate from Columbia University College of Physicians and Surgeons in 1908. He was appointed faculty at Columbia and Presbyterian Medical Centers before going on to become professor of surgery at his alma mater for the next 25 years. He published the report of his eponymous surgery in 1935 and only performed it 37 times in his lifetime. He also supervised Virginia Apgar and advised her to pursue a career in anesthesiology because he saw an “energy and ability to make significant contributions” that would advance both fields. Other notable accomplishments include helping establish the American Board of Surgery and establishing another eponymous diagnostic triad for insulinoma.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.