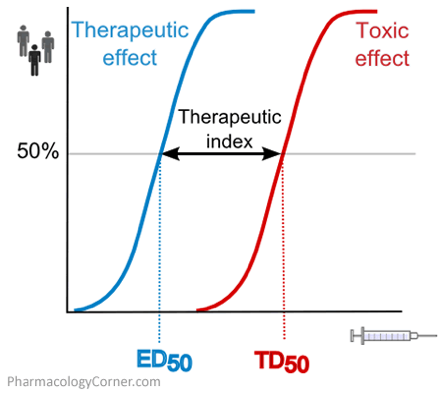
Therapeutic Index
This is the balance between toxic and therapeutic dosing of pharmacotherapeutic agents, and can be described as the relationship between underdosing (seeing no effect), effective dosing (achieving desired results), and overdosing (having toxic complications). Specifically, it is the difference between the toxic dose for 50% of the population and the effective dose for 50% of the population.

Types of Chemotherapy
Direct DNA-Interacting Agents
- Alkylating
- Cyclophosphamide
- Cisplatin
- Carboplatin
- Antitumor Antibiotics and Topoisomerase Poisons
Indirect DNA-Interacting Agents
- Antimetabolites
- 5-Fluorouracil (5FU)
- Methotrexate
- 6-mercaptopurine (6MP)
- Azithropine
Antimitotic Agents
Hormone Receptor-Targeted Agents
- Tamoxifen
- Diethylstilbestrol
Protein Kinase Antagonists
Multikinase Inhibitors
Proteasome Inhibitors
Histone Deacetylase Inhibitors
mTOR Inhibitors
Complications of Chemotherapy
Myelosuppression
By definition, chemotherapy is designed to destroy mature, cancer cells, so it only makes sense that bone marrow suppression is affected. The most dreaded complication associated with myelosuppression is acquired neutropenia. This can occur anywhere from 2-6 weeks after chemotherapy and the only presenting sign that something is wrong is a febrile episode (>38oC).
Definition of neutropenia is an absolute neutrophil count (ANC) < 1500 cells/microL. This can be automatically calculated by most labs, but it is calculated as follows:
ANC = WBC x 10(%PMN + %Bands)
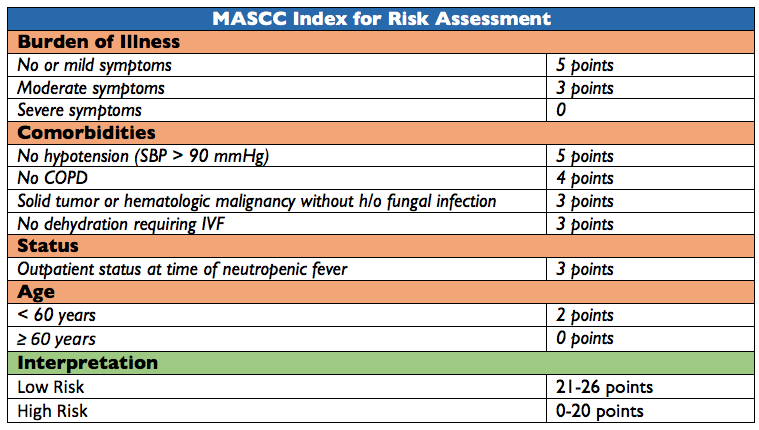
Risk assessment is done via the Multinational Association for Supportive Care in Cancer (MASCC) index:

Neutropenic patients are at an increased risk of infection due to the inefficiency, or absence, of circulating WBC to combat infection. The management of neutropenic patients should include
- Immediate contact precautions
- Providers and visits
- Gowns, gloves, hats, masks
- Broad spectrum antibiotics for duration of neutropenia
- Low Risk
- Outpatient oral antibiotics
- Ciprofloxacin + amoxicillin/clavuanate
- High risk
- Initial management is monotherapy with antipseudomonal agent:
- Pipercillin/tazobactam
- Meropenem
- Cefepime
- Imipenem
- Ceftazidime
- May add other agents if clinical scenario suggests:
- Vancomycin
- Metronidazole
- Antivirals
- Antifungals

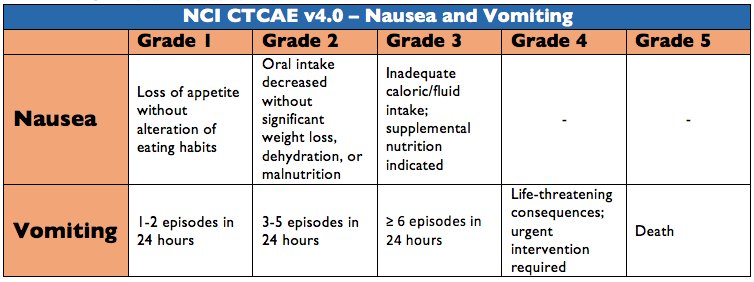
Nausea and Vomiting

N/V associated with chemotherapy can be acute (<24hr), delayed (>24hrs), or even anticipatory. Chemoprophylaxis for N/V is based on risk and broken down into highly emetogenic, moderately emetogenic, low emetogenic, and minimally emetogenic therapies. Treatment revolves around some combination of:
- Neurokinin 1 Receptor Antagonist (NK1)
- Aprepitant
- Fosaprepitant
- Rolapitant
- 5-hydroxytryptamine-3 Antagonist (5-HT3)
- Ondansetron
- Palonosetron
- Granistron
- Glucocorticoid

Mucositis
Profound inflammatory process of the mucous membranes and is characterized by:
- Initiation of insult (chemo)
- Upregulation/Generation of messenger signals and proinflammatory cytokines
- Signaling and Amplification
- Damage of tissue by cytokines is amplified via feedback loops
- Ulceration and inflammation
- Healing
Symptoms generally start to begin after day 7 and can range from mild inflammation to complete ulceration and inability to take anything PO. Epithelial sloughing after ulceration can produce the classic pseudomembane appearance. This desquamation can now lead to bacterial translocation in an already immunocompromised host.



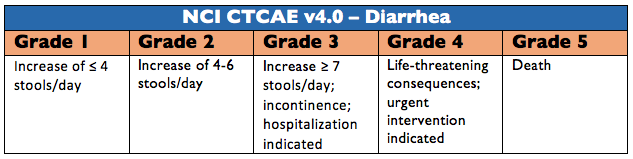
Diarrhea

3 main mechanisms that cause chemotherapy-related diarrhea:
- Secretory Diarrhea
- Increased intraluminal secretion of electrolytes from epithelial damage
- Osmotic Diarrhea
- Increased intraluminal osmotic substances from brush border damage
- Altered GI motility
- Increased peristalsis and emptying
Different types of colitis syndromes may also occur and cause diarrhea:
- Neutropenic entrocolitis
- A form of necrotizing enterocolitis, or typhlitis
- Ischemic colitis
- Associated with docetaxel regimens
- Diff associated colitis

Outpatient management can be:
- Loperamide 4mg initial dose followed by 2mg every 2-4 hours
- Octreotide 100-150 mcg SQ every 8 hours (can increase to 500-1500 mcg/dose)
Inpatient/Emergency management:
- Octreotide 25-50 mcg/hour infusion
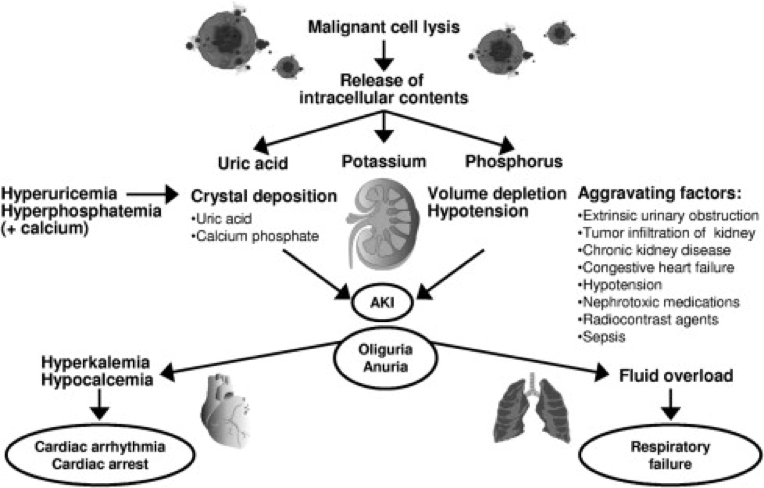
Tumor Lysis Syndrome

Occurs after massive tumor cell lysis (most commonly with high-grade lymphomas and ALL) and can cause the following biochemical abnormalities:
- Hyperuricemia
- Can cause uric acid nephropathy and AKI
- Hyperkalemia
- From the lysis and intracellular distribution
- Hyperphosphatemia
- Can cause calcium phosphate deposition in the renal tubules and precipitate AKI
- Hypocalcemia
- Hyperphosphatemia causes significant hypocalcemia and can precipitate dysrhythmias
The Cairo-Bishop scale is used for grading severity of disease:

Diagnosis can be made with 2 or more laboratory abnormalities, or one laboratory abnormality and one clinical abnormality.
Treatment is multitiered and consists of:
- Fluid resuscitation
- Electrolyte correction
- Renal protection
- Rasburicase – oxidizes uric acid
Cottage Physician


References
- Information for Health Care Providers. (2016, December 14). Retrieved February 27, 2017, from https://www.cdc.gov/cancer/preventinfections/providers.htm
- Sausville EA, Longo DL. Principles of Cancer Treatment. In: Kasper D, Fauci A, Hauser S, Longo D, Jameson J, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 19e New York, NY: McGraw-Hill; 2014. http://accessmedicine.mhmedical.com/content.aspx?bookid=1130§ionid=71748332. (Accessed February 27, 2017).
- Freifeld AG, Bow EJ, Sepkowitz KA. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of America. Clinical Infectious Diseases : an official publication of the Infectious Diseases Society of America. 2011;52(4):e56-93. [pubmed]
- Klastersky J, Paesmans M, Rubenstein EB. The Multinational Association for Supportive Care in Cancer risk index: A multinational scoring system for identifying low-risk febrile neutropenic cancer patients. Journal of Clinical Oncology : official journal of the American Society of Clinical Oncology. 2000;18(16):3038-51. [pubmed]
- Hesketh PJ, Kris MG, Grunberg SM. Proposal for classifying the acute emetogenicity of cancer chemotherapy. Journal of Clinical Oncology : official journal of the American Society of Clinical Oncology. 1997;15(1):103-9. [pubmed]
- Hesketh PJ, Bohlke K, Lyman GH. Antiemetics: American Society of Clinical Oncology Focused Guideline Update. Journal of Clinical Oncology : official journal of the American Society of Clinical Oncology. 2016;34(4):381-6. [pubmed]
- Roila F, Molassiotis A, Herrstedt J. 2016 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting and of nausea and vomiting in advanced cancer patients. Annals of Oncology : official journal of the European Society for Medical Oncology. 2016;27(suppl 5):v119-v133. [pubmed]
- Sonis ST, Elting LS, Keefe D. Perspectives on cancer therapy-induced mucosal injury: pathogenesis, measurement, epidemiology, and consequences for patients. Cancer. 2004;100(9 Suppl):1995-2025. [pubmed]
- Sonis ST. The pathobiology of mucositis. Nature reviews. Cancer. 2004;4(4):277-84. [pubmed]
- Common Terminology Criteria for Adverse Events (CTCAE), Version 4.0, June 2010, National Institutes of Health, National Cancer Institute. Available at: http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf (Accessed February 27, 2017).
- Benson AB, Ajani JA, Catalano RB. Recommended guidelines for the treatment of cancer treatment-induced diarrhea. Journal of Clinical Oncology : official journal of the American Society of Clinical Oncology. 2004;22(14):2918-26. [pubmed]
- Hande KR, Garrow GC. Acute tumor lysis syndrome in patients with high-grade non-Hodgkin’s lymphoma. The American Journal of Medicine. 1993;94(2):133-9. [pubmed]
- Cairo MS, Bishop M. Tumour lysis syndrome: new therapeutic strategies and classification. British journal of haematology. 2004;127(1):3-11. [pubmed]