Question
What the anatomic landmarks for estimation of gestational age based on fundal height measurements?


What the anatomic landmarks for estimation of gestational age based on fundal height measurements?
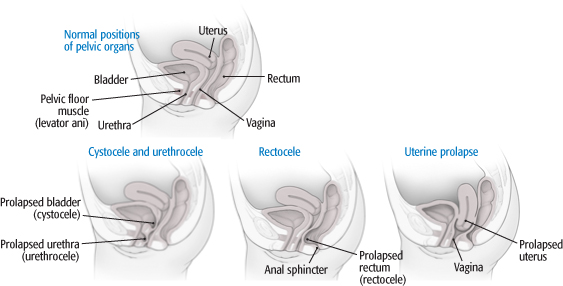
What are the two main classification and scoring systems for grading pelvic organ prolapse syndrome in women?
Other Known Aliases – alkali denaturation test
Definition – Lab test where the blood sample is hemolyzed using sterile water and centrifuged to produce a hemoglobin supernatent. This is then mixed with 1% NaOH. Fetal hemoglobin will stay pink, while maternal hemoglobin will turn yellow/brown.

Clinical Significance – Helps differentiate maternal from fetal blood in cases of vaginal bleeding or neonatal hematemesis/hematochezia.
History – Given to Dr. Leonard Apt and Dr. William Downey, Jr., who were physicians at Harvard Medical School and Children’s Medical Center in Boston, MA in the mid-1900’s.
References
References
Other Known Aliases – Fetus Ejection Reflex
Definition – Stimulation of the cervix leading to contraction of the uterus through oxytocin release.
Clinical Significance – Demonstrates positive feedback during labor and delivery to increase uterine contractions as cervical dilation progresses. Long standing belief that epidural anesthesia before cervical dilation increased risk of cesarean section (this was debunked in 2005).
History – Given to Dr. James Ferguson, a Canadian obstetrician, in 1940 after he showed this physiologic effect in rabbits and postulated it to be true in humans.
References

History of FIGO
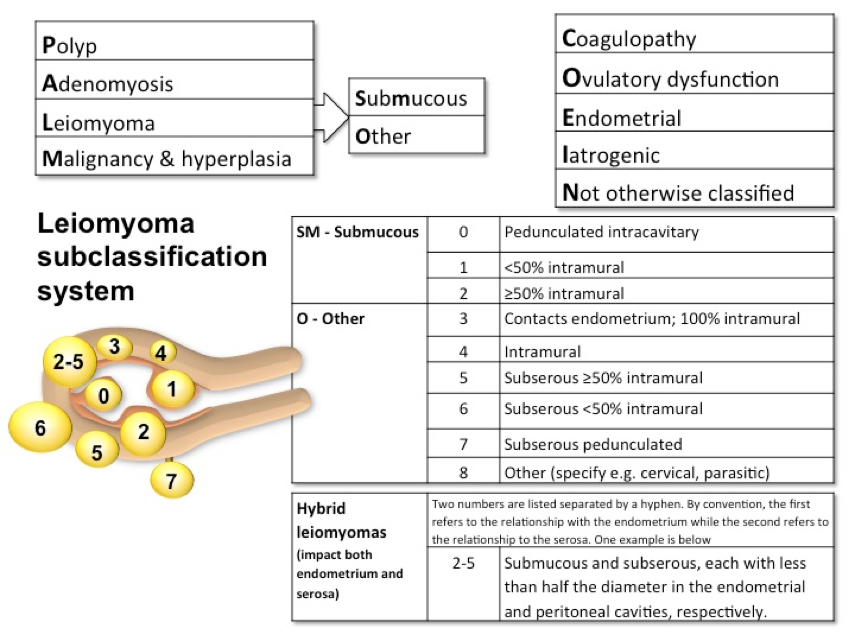
Because of confusing terminology and difficulty in translating to other languages, the International Federation of Obstetrics and Gynecology (FIGO) created a special task force in 2005 charged with clarifying the terminology and classifying the different causes. This way clinicians, patients, and researchers throughout the world could be talking the same language. Dysfunctional uterine bleeding (DUB) was replaced by abnormal uterine bleeding (AUB).. They also introduced a classification system to help sub-divide the causes of AUB.
But in order to define something as “abnormal”, they needed to define normality, which can obviously be very difficult when incorporating the world’s population. The consensus definitions were then agreed upon in 2015 to include the 5th to 95th percentiles form the available data.
The FIGO definition of AUB is any symptomatic variation from normal menstruation, with regards to frequency, regularity, duration, or volume.

Classifications of Abnormal Uterine Bleeding
In 2011, FIGO created a classification system for the main causes of AUB. It is broken down into 2 main categories based on whether or not the pathology can be seen on imaging or histopathology. This also allows for subclassifications due to multiple etiologies.
Documentation
Very similar to the documentation for an OB patient (TPAL score), the documentation uses the PALM-COEIN scoring system for “simplicity”. Example:
References

Definition – Blue discoloration of the cervix and vaginal mucosa seen in early pregnancy.
Clinical Significance – Due to increased blood flow to support a newly implanted embryo and can be seen 6-8 weeks after conception.
History – Given to James R. Chadwick, an American gynecologist of the late 19th century, after he read a paper before the American Gynecologic Society in 1886, but 1st described by Etienne Jacquemin in 1836. Dr. Chadwick did give appropriate recognition to Dr. Jacquemin during this presentation.
References

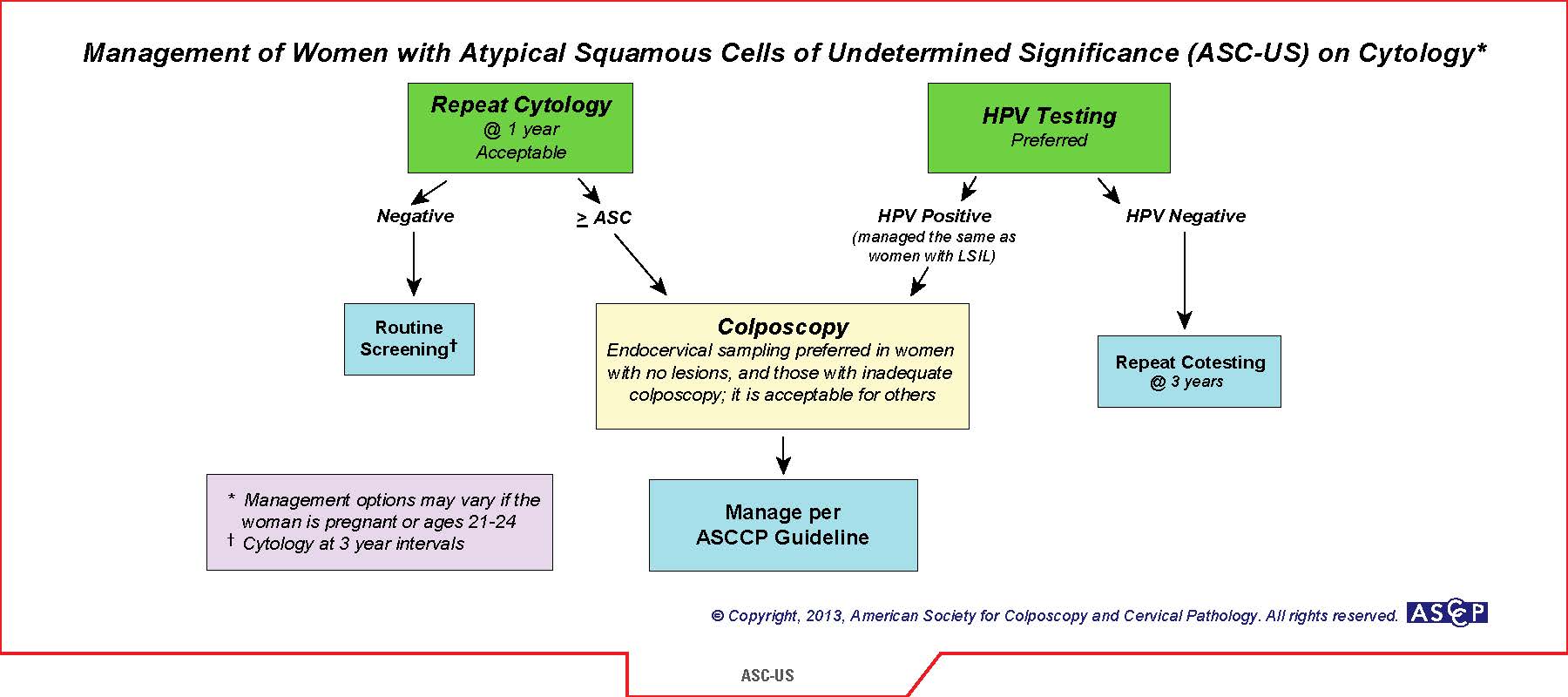
Next best step: Reflex HPV cotesting
Follow-up Recommendations: 3 years
Atypical squamous cells of undetermined significance (ASC-US) is a common “abnormal” pap result. The 2012 American Society of Clinical Pathologist (ASCP) recommend that women ages 21-29 should have routine cytology alone performed every 3 years as long as the results are normal. If ASC-US results, then reflex HPV contesting is recommended. If HPV (-), then return to routine cytology in 3 years. If HPV (+), then proceed to colposcopy. Another acceptable option is to have the patient return to clinic in 1 year for repeat pap. If ASC-US (+) again, then proceed to colposcopy. The logic is that most women in this age group clear any HPV infection without the need for colposcopy. This is the safer choice if the patient is wanting to have more children to limit any complications of cervical incompetence.
References
1) American Society of Clinical Pathologists. Screening Guidelines. Available at: http://www.asccp.org/guidelines/screening-guidelines.

Definition of Gestation/Pregnancy-Induced Hypertension
Epidemiology
Pathophysiology
This is still unknown but several theories exist and include:
Risk Factors
Fetal Well-being
Laboratory Evaluation
Preeclampsia
Management
Revolves around 3 main factors:

Broekhuijsen K, et al. Lancet. 2015;385(9986):2492-501.
HYPITAT-II Trial (HYPertension and Preeclampsia Intervention At Term)
Non-severe (<160/110mmHg) and no preeclampsia
Severe (>160/110mmHg) and no preeclampsia

Preeclampsia

Hauth JC, et al. Obstet Gynecol. 200;95(1):24-8.
Long-term Prognosis
References
1) ACOG Task Force on Hypertension in Pregnancy. Obstetrics & Gynecology. 2013;122(5).
