Crigler-Najjar Syndrome
Other Known Aliases – familial/hereditary nonhemolytic unconjugated hyperbilirubinemia
Definition – Rare, familial condition resulting in congenital hyperbilirubinemia secondary to a deficiency of glucuronyl transferase. There two types, with type I being very rare and severe (absolute absence) and type II being more common and less severe (relative deficiency)
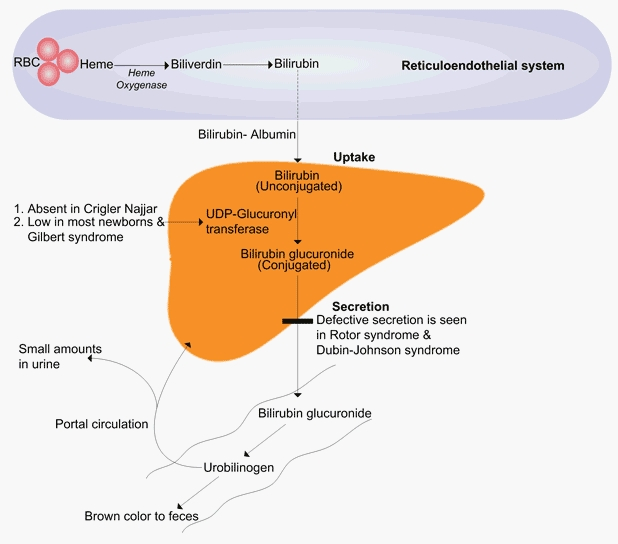
Clinical Significance – Congenital hyperbilirubinemia can have catastrophic effects on the infant including jaundice, lethargy, failure to thrive, hypotonia, kernicterus, and acute bilirubin encephalopathy once it saturates and binds to the brain tissue.
History – Named after:
1) John Fielding Crigler (1919-), who is an American pediatrician who earned his medical doctorate at Duke University in 1943 and practiced at the Children’s Hospital of Boston.
2) Victor Assad Najjar (1914-), who is a Lebonese-born, American pediatrician who earned his medical doctorate at the American University in Beirut and practiced at Johns Hopkins, Vanderbilt, and Tufts University.

They published their findings of a new disease causing congenital familial nonhemolytic jaundice with kernicterus in 1952.
References
- Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
- Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
-
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved
http://itunes.apple.com.
- Whonamedit – dictionary of medical eponyms. http://www.whonamedit.com
- Crigler-Najjar Syndrome. Genetics Home Reference. https://ghr.nlm.nih.gov/condition/crigler-najjar-syndrome#synonyms
-
CRIGLER JF, NAJJAR VA. Congenital familial nonhemolytic jaundice with kernicterus; a new clinical entity. A.M.A. American journal of diseases of children. 1952; 83(2):259-60. [
pubmed]