One of the more common conditions that is managed in all of medicine is hypertension. The first Joint National Committee (JNC) recommendations were published in 1976 and have gone through 8 revisions, with the most recent being in 2014. The interesting thing about the JNC 8 is that it took 11 years to get published (4-6 years for all the other updates). Even then there is still some controversy surrounding its recommendations.
Joint National Committee 8
Emphasis on randomized, controlled clinical trials to answer 3 key clinical questions:
- Does initiating antihypertensive pharmacologic therapy at specific blood pressure thresholds improve health outcomes?
- When to start
- Do attempts to reach specified blood pressure goals with antihypertensive pharmacologic therapy lead to improvements in health outcomes?
- What to shoot for
- Do various antihypertensive drugs or drug classes differ in regard to specific health outcomes?
- What to use
9 Graded Recommendations
- Adult patients 60 years of age or older, without specific comorbidities, should have antihypertensive medications initiated if SBP > 150 mmHg or DBP > 90 mmHg and treat to a goal SBP < 150 mmHg and DBP < 90 mmHg.
- Corollary
- If treated SBP < 140 mmHg is well tolerated and without adverse effects on health or quality of life, no adjustment is needed.
- Adult patients younger than 60 years of age, without specific comorbidities, should have antihypertensive medications initiation if DBP > 90 mmHg and treat to a goal DBP < 90 mmHg.
- Adult patients younger than 60 years of age, without specific comorbidities, should have antihypertensive medications initiation if SBP > 140 mmHg and treat to a goal SBP < 140 mmHg.
- Adult patients older than 18 years of age with chronic kidney disease should have antihypertensive medications initiated if SBP > 140 mmHg or DBP > 90 mmHg and goal should be SBP < 140 mmHg and DBP < 90 mmHg.
- Adult patients older than 18 years of age with diabetes should have antihypertensive medications initiated if SBP > 140 mmHg or DBP > 90 mmHg and goal should be SBP < 140 mmHg and DBP < 90 mmHg.
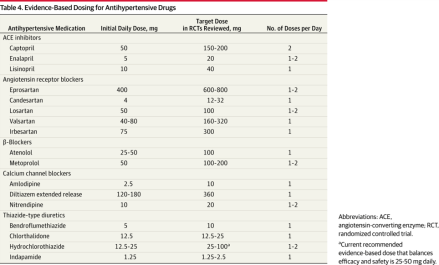
- Initial drug therapy for nonblack patients (including diabetic patients) should include a thiazide-type diuretic, calcium channel blocker, an ACEI, or ARB.
- Initial drug therapy for black patients (including diabetic patients) should include a thiazide-type diuretic or calcium channel blocker.
- Adult patients older than 18 years of age with chronic kidney disease, initial or additional therapy should include an ACEI or ARB, regardless of race or diabetic status.
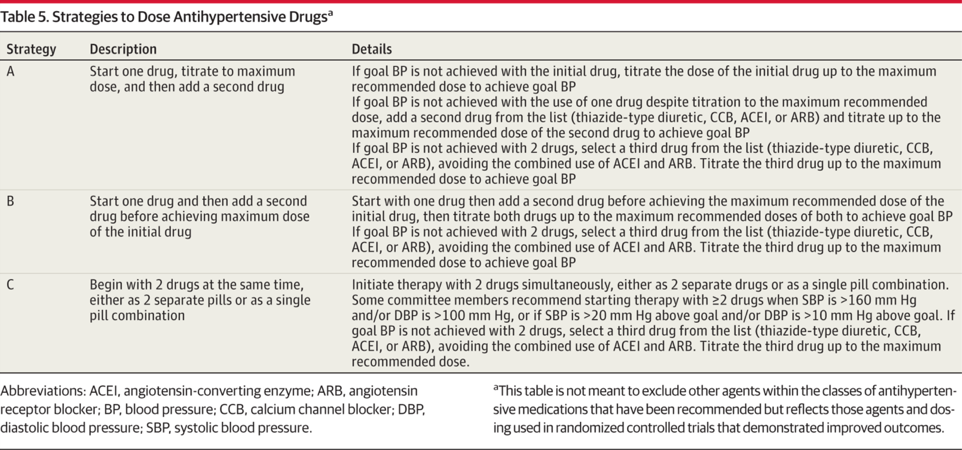
- If blood pressure goal is not achieved in one month, either increase dose of initial drug or add a second drug. A third drug should only be added if goal is not achieved with two medications.
- ACEI and ARB should not be used together

JNC-8. JAMA. 2014;311(5):507-520
JNC-8. JAMA. 2014;311(5):507-520

JNC-8. JAMA. 2014;311(5):507-520

Systolic Blood Pressure Intervention Trial (SPRINT)
Published in November 2015 in New England Journal of Medicine
This was a multi-center randomized, controlled, open label clinical trial performed to evaluate a more intensive blood pressure strategy (SBP < 120 mmHg) in patients with high risk cardiovascular risk (excluding diabetes, previous stroke, symptomatic heart failure, proteinuria, or nursing home residents). They used a primary composite outcome was first occurrence of AMI, other ACS, stroke, heart failure, or death from cardiovascular disease.
Participant criteria:
- ≥ 50 years of age
- SBP of 130-180 mmHg
- Increased cardiovascular risk as defined by at least one of the following:
- Clinical or subclinical cardiovascular disease other than stroke
- Chronic kidney disease (excluding PCKD)
- 10-year cardiovascular disease risk of ³ 15% using Framingham Score
- ≥ 75 years of age
Treatment algorithm used all major classes of antihypertensives in no particular rank order. Participants were seen monthly for the first three months and every three months thereafter. The median follow-up was 3.26 years, but the study was stopped early due to the benefit of treatment group by the data and safety monitoring board of the trial.
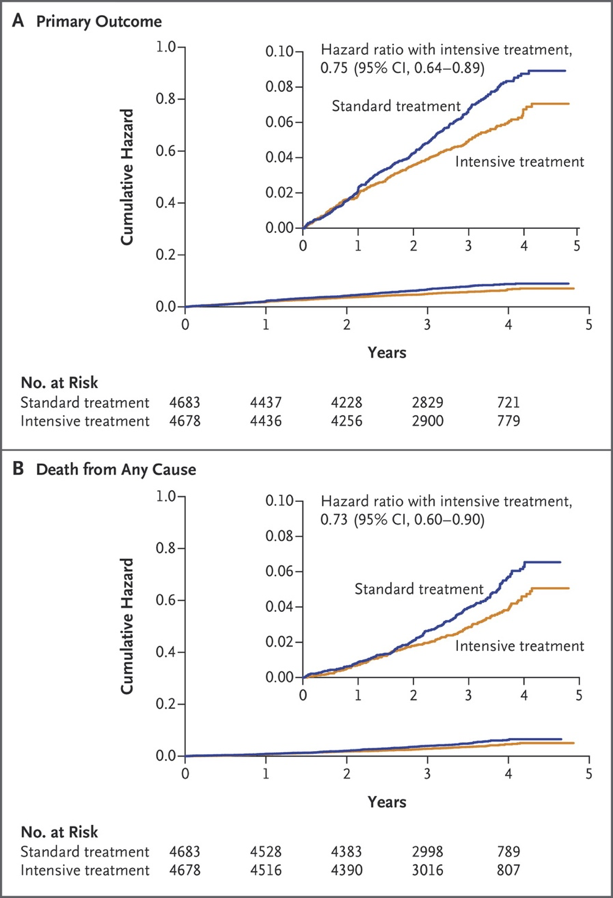
Outcomes
562 primary outcome events identified
- 243 in the intensive group (1.65% per year)
- 319 in the control group (2.19% per year)
Number needed to treat to prevent a primary outcome – 61
Number needed to treat to prevent death from any cause – 90
Number needed to treat to prevent death from cardiovascular causes – 172
Serious Adverse Events
1793 participants in intensive group (38.3%)
1736 participants in control group (37.1%)
Examples:
- Hypotension
- Syncope
- Electrolyte abnormalities
- Acute kidney injury
- Injurious falls
- Bradycardia
Discussion
25% lower relative risk of primary outcome in intensive group (5.2% vs 6.8%):
- 38% lower relative risk of heart failure (1.3% vs 2.1%)
- 43% lower relative risk of death from cardiovascular causes (0.8% vs 1.4%)
- 27% lower relative risk of death from any cause (3.3% vs 4.5%)

SPRINT Research Group. NEJM. 2015;373:2103-2116

SPRINT Research Group. NEJM. 2015;373:2103-2116
Should we be more aggressive in the SPRINT patient population?
(great review by Health News Review here)
First of all, this is only ONE study addressing a clinical question that has been extensively researched and we still don’t have good, reliable, reproducible results yet. See 2009 Cochrane Hypertension Review that stated blood pressure < 140/90 mmHg was not beneficial.
Second of all, the researchers seemed to down play the serious adverse events. The author of the Health News Review put a nice table together and did a few extra EBM calculations (below) to help illustrate:

125: Number needed to treat to prevent one case of heart failure.
167: Number needed to treat to prevent one death by cardiovascular causes
83: Number needed to treat to prevent death by any cause
100: Number needed to harm to cause one case of hypotension
167: Number needed to harm to cause one case of syncope
125: Number needed to harm to cause one case of electrolyte abnormality
56: Number needed to harm to cause one case of acute kidney injury or renal failure
42: Number needed to harm to cause one serious adverse event
So what I take away from the SPRINT study:
- This is data from a single study. Need more to change practice.
- Composite endpoints should be used with caution…especially since it was stopped early and may overestimate the benefit and underestimate the risk.
- Researchers used automated BP measurements which is shown to be lower (5-10 mmHg) than auscultated BP measurement. This alone could cause clinicians to intensify BP control and increase adverse events that weren’t needed.
- It doesn’t help us with patients with diabetes, previous stroke, symptomatic heart failure, or nursing home residents…which encompass a lot of patients being managed for hypertension.
References
- James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-20.
- Hernandez-Vila E. A review of the JNC 8 blood pressure guideline. Tex Heart Inst J. 2015;42(3):226-228.
- The SPRINT Research Group. A randomized trial of intensive versus standard blood pressure control. N Engl J Med. 2015;373:2103-2116.