Quick pimp question in regards to children:
What does 2-weeks, 6-months, and 12-months mean to you and what do they have in common?

Quick pimp question in regards to children:
What does 2-weeks, 6-months, and 12-months mean to you and what do they have in common?

Question #1
Which of the following genetic mutations is seen with chronic myelogenous leukemia?
Answer:
Translocation of chromosome 9 and 22. This new chromosome 22 is called “Philadelphia chromosome” after the city where the two hospitals that first identified the gene mutation in 1960 were both located.
Question #2
Which of the following cancer markers are classically associated with ovarian cancer?
Answer:
CA-125


The textbook definition of anemia is a reduction of the absolute number or mass of circulating red blood cells. This then causes a global reduction in the oxygen carrying capacity of the patient’s circulatory system. Clinically, we use hemoglobin and hematocrit as the surrogate markers and define anemia as 2 SD below the mean for gender:

Patel KV. Haematologica. 2008;93(9):1281-1283.
There are two general approaches you can use to help identify the cause of anemia in adults.
Anemia is usually first diagnosed by CBC. Once you have a documented low H/H, then you need order follow-up studies to help differentiate the cause of the anemia. These include:

Schrier SL, et al. Approach to adults with anemia. In: Up To Date. Waltham, MA (Accessed 03/23/2016)
Something new I thought I would bring to the PAINE Podcast. As you all know, I am quite a fan of medicine and antiquity. Shortly after I married my wife, her grandfather past away from a progressive esophageal cancer. One of the things I was able to keep when helping clean out his house, was a copy of The Cottage Physician printed in 1893. It was basically a handbook on how to treat common ailments of the time. I will try to add excerpts from this book when appropriate so you can have a sense of how medicine was practiced in the late 19th century.
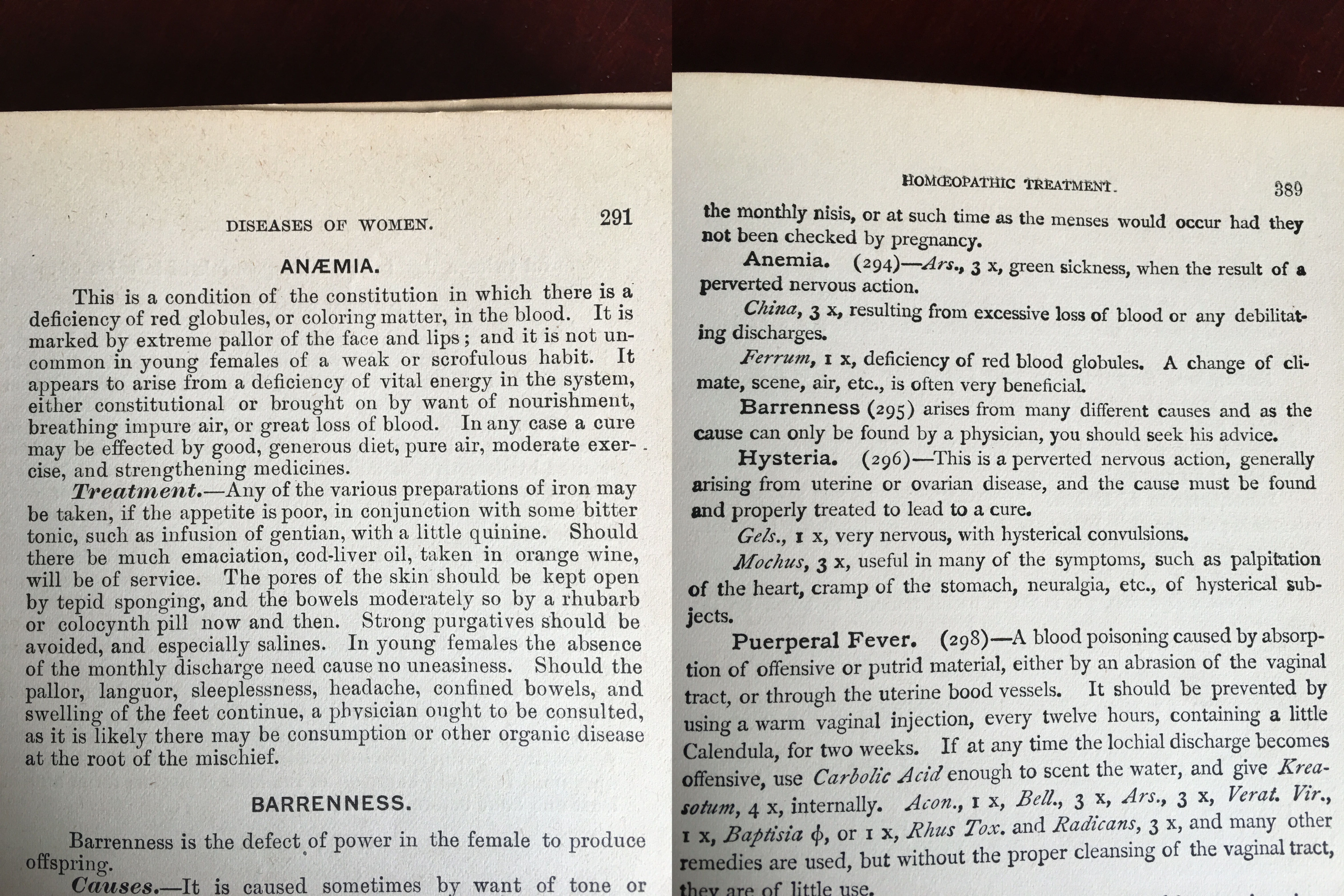
The Cottage Physician. 1863
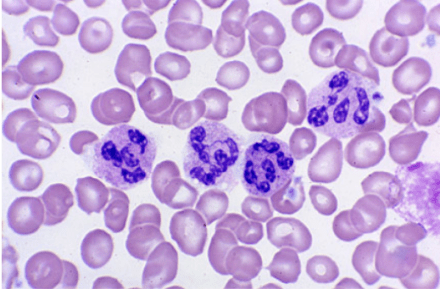
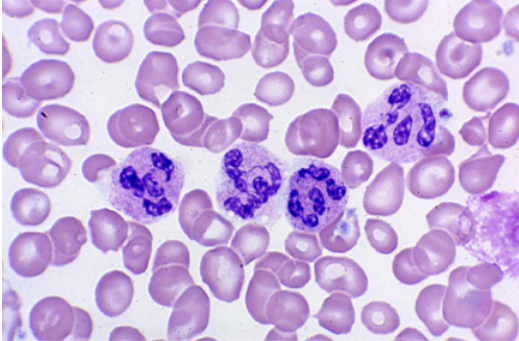
This patient has had a history of gastric cancer with a partial gastrectomy and now presents with a fatigue and gait disturbances. CBC reveals a macrocytic aneamia and peripheral smear shows multinucleated neutrophils. The gait disturbances are most likely due to the progressive peripheral neuropathy. This is most consistent with vitamin B12 deficiency. Intrinsic factor, which is secreted by the parietal cells of the stomach, is required for vitamin B12 absorption in the terminal ileum.
Work-Up for Vitamin B12 Deficiency
Serum B12 Level
Metobolites
Possible additional testing in the setting of macrocytic anemia:
Treatment for B12 Deficiency
References
62-year-old male presents to primary provider’s office with a six-month history of fatigue and gait disturbance. He denies recent falls, weakness, pain, paralysis, or dizziness.
Medications
Lisinopril 10mg daily
Metformin 1000mg BID
Men’s multivitamin
Fish oil
Past Medical History
Diabetes Mellitus II
Hypertension
Gastric cancer
Past Surgical History
Cholecystectomy – 1997
Partial gastrectomy – 2004
Vitals
BP-128/79, HR-81, RR-14, O2-100%, Temp-98.9o
Physical Exam
General – WN/WD, NAD
Skin – scattered senile purpura, no petechiae
CV – RRR without M/G/R
Pulmonary – CTA bilaterally without adventitial breath sounds
Neurologic – A&Ox3, 5/5 strength throughout bilaterally, DTR 2+ and equal, FROM, vibratory sensation decreased in bilateral lower extremities
Laboratory Studies
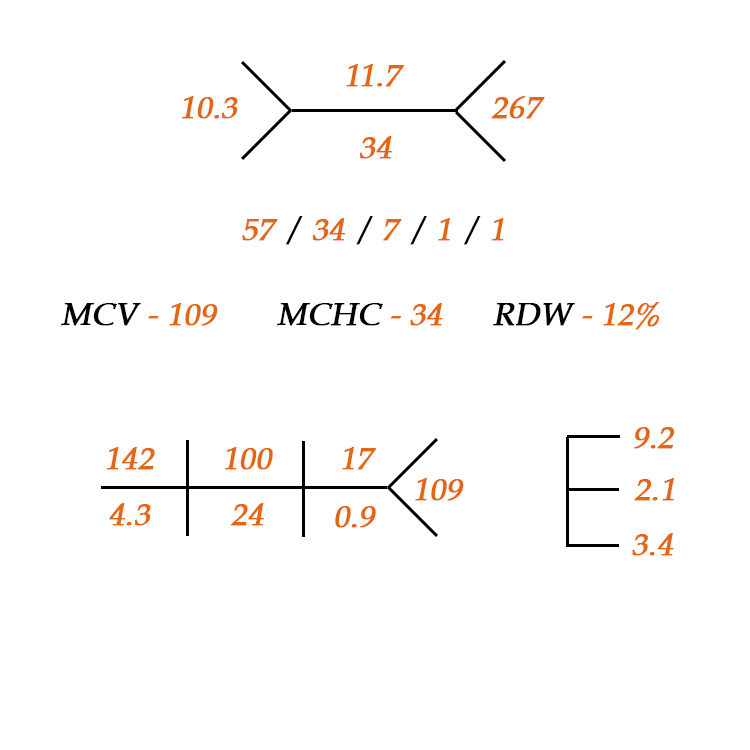


Fishbone diagram for CBC with differential
References
1) Pagana KD, Pagana TJ. Mosby’s Manual of Diagnostic and Laboratory Tests. 5th ed. St. Louis, MO. Elsevier. 2014.
2) Lee M. Basic Skills in Interpreting Laboratory Data. 5th ed. Bethesda, MD. American Society of Health-Systems Pharmacists. 2013
3) Laposata M. Laboratory Medicine: The Diagnosis of Disease in the Clinical Laboratory. 2nd ed. New York, NY. 2014.
This is my post for The American Academy of Physician Assistants Blog “PAs Connect” in a recurring series called “Professor’s Corner”.
School is all about memory. You are presented information in class and you try to remember everything the professor is saying in order to transcribe what you think is important on your notes. Then you go home and study these notes, textbook chapters, and journal articles to help try to make sense of the material. This is where our cognitive weapons of choice come out: different colored highlighters, index cards, sticky notes….all in the hopes that it is processed into neat little compartments in your brain so you can recall them for the exam. Rinse…wash…repeat for 2.5 years of PA school. But what is the science behind memory and why do somethings work better than others?
Most people think of memory as just short term and long term, but depending on which psychologic theory of memory you prescribe to, there can be many more. I, personally and professionally, like the three-tiered, information processing model to memory: sensory, working, and long-term.

Sensory Memory
The first step in memory involves the processing of sensory stimuli that are introduced in the learning environment. The brain uses three main senses (sight, sound, touch) to get as much information brought in as possible. Now, if you had to process every single sensory stimulus into your working memory, your brain would get overloaded in a matter of seconds. To avoid this, you use sensory memory as the environmental buffer to pick and choose what you think is the most important……this is where attention comes in. Attention is the filter from the sensory memory system into the working memory system and allows us to focus on smaller, more important sensory stimuli.
Attention is the bodyguard outside of Club Working Memory. He will pick and choose what information gets through for further processing to make sure the club isn’t overcrowded.
Working Memory
Once the sensory information is attended to, we can store it in a temporary cognitive sandbox where we can actually work with it. This is your working memory. It is short (15-30s) and the information stored here only stays if the learner is actually doing something with it (rehearsal). There are 3 main components of working memory: central executive (supervisor), the phonological loop (language storage), the visuospatial sketchpad (visual storage). As you hear and see things over and over again, you start to make connections and correlation between the information and begin to encode it all into neat data packages. Each system is different and the cognitive load when using both systems is only slightly higher than using them individually. Cognitive psychologists recommend using this to your advantage while studying. For example, assign each class a room in your house and only study in this room. It will increase the likelihood of correctly recalling the information when you can get your cognitive bearings straight on the location you learned the information. You can incorporate similar strategies such as listening to different music or artists for different subjects.
The more you rehearse this information in working memory, the greater the cognitive load….but the higher likelihood it will make it to long-term memory.

Long-term Memory
Due to this increased cognitive load of working memory, it is not possible to keep information in working memory indefinitely. This is where long-term memory comes into play. We try to categorize this information into packages for easy storage and recall in long-term memory. There are 3 steps to this process: encoding, storage, and retrieval/rehearsal. The majority of the energy used when studying is trying to encode the information in working memory so it can be efficiently and effortless recalled when needed. This is why mnemonics, acronyms, and all the other things we do as students help process and package new information so we can remember them later. “Oh Oh Oh To Touch And Feel Very Good Velvet, Ahhhh” may mean nothing to you, but it is how I can still recall all 12 cranial nerves to this day.
Loss of Memory
Even with all these sophisticated and complicated cognitive pathways that our brains have developed to retain information, we still forget and lose information. There are many theories behind this, but the 2 main ones I like are: information decay (the less you use it, the less you can recall) and interference (learning new information inhibits recall of old information).
To limit interference when I am teaching, I try not to overload the senses with extraneous stimuli. If I stand up and just read the powerpoint (which is not teaching by the way), you (the student) can’t listen to what I am saying when you are being bombarded with paragraphs of text that you feel compelled to read. This leads to overload of the sensory and working memory as you are trying to listen, read, and process everything that is being thrown at you.
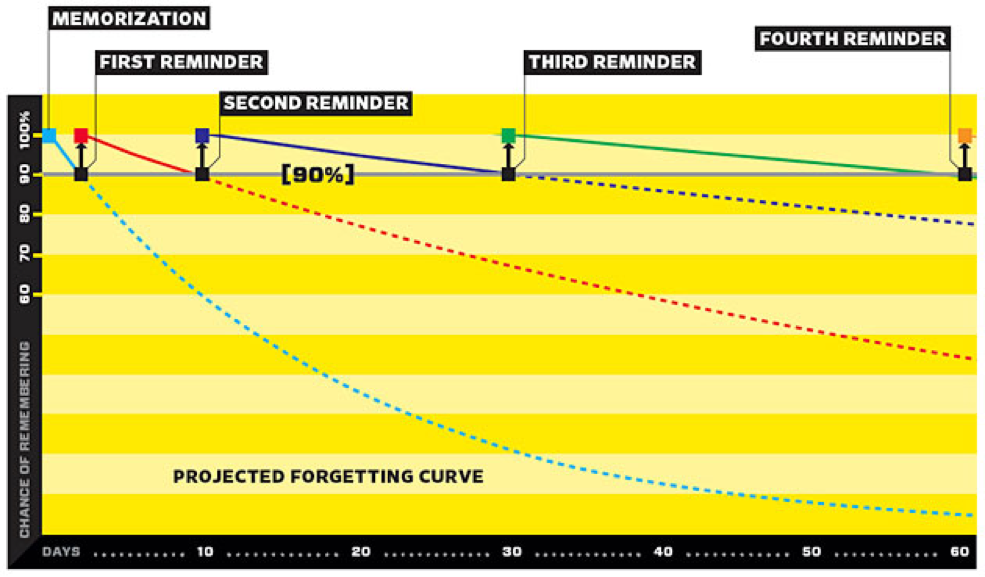
To limit long-term memory decay, I utilize spaced repetition. When I am teaching, I like to bring up old information (last exam, least semester, etc…) to re-introduce to it to my students. It is also why I believe in comprehensive final examinations. It gives them an opportunity to dust off the stored information in long-term memory and play with it again in the sandbox of working memory. This strategy has been shown to improve retention and efficiency of recall when you need it the most…..when taking care of patients.
Wolf G. Want to Remember Everything You’ll Ever Learn? http://www.wired.com/2008/04/ff-wozniak/?currentpage=all
References
1) Anderson JR. Cognitive psychology and its implications. 7th ed. Worth Publishers. 2009
2) McLeod SA. Working Memory | Simply Psychology. Available at: http://www.simplypsychology.org/working memory.html. Accessed February 15, 2016.
3) Cognition (Sensory memory). Introduction to Instructional Design. Available at: http://byuipt.net/564/2013/08/23/cognition-sensory-memory/. Accessed February 15, 2016
4) Baddeley AD. Working memory. Science. 1992;255:556-559.
5) Cognition (Long-term memory). Introduction to Instructional Design. Available at: http://byuipt.net/564/2013/08/23/cognition-long-term-memory/. Accessed February 15, 2016.
6) Wolf G. Want to Remember Everything You’ll Ever Learn? Surrender to This Algorithm. Wired.com. Available at: http://www.wired.com/2008/04/ff-wozniak/?currentpage=all. Accessed February 15, 2016.
7) Nickson C. Learning by Spaced Repetition. Life in the Fast Lane Medical Blog 2011. Available at: http://lifeinthefastlane.com/learning-by-spaced-repetition/. Accessed February 15, 2016
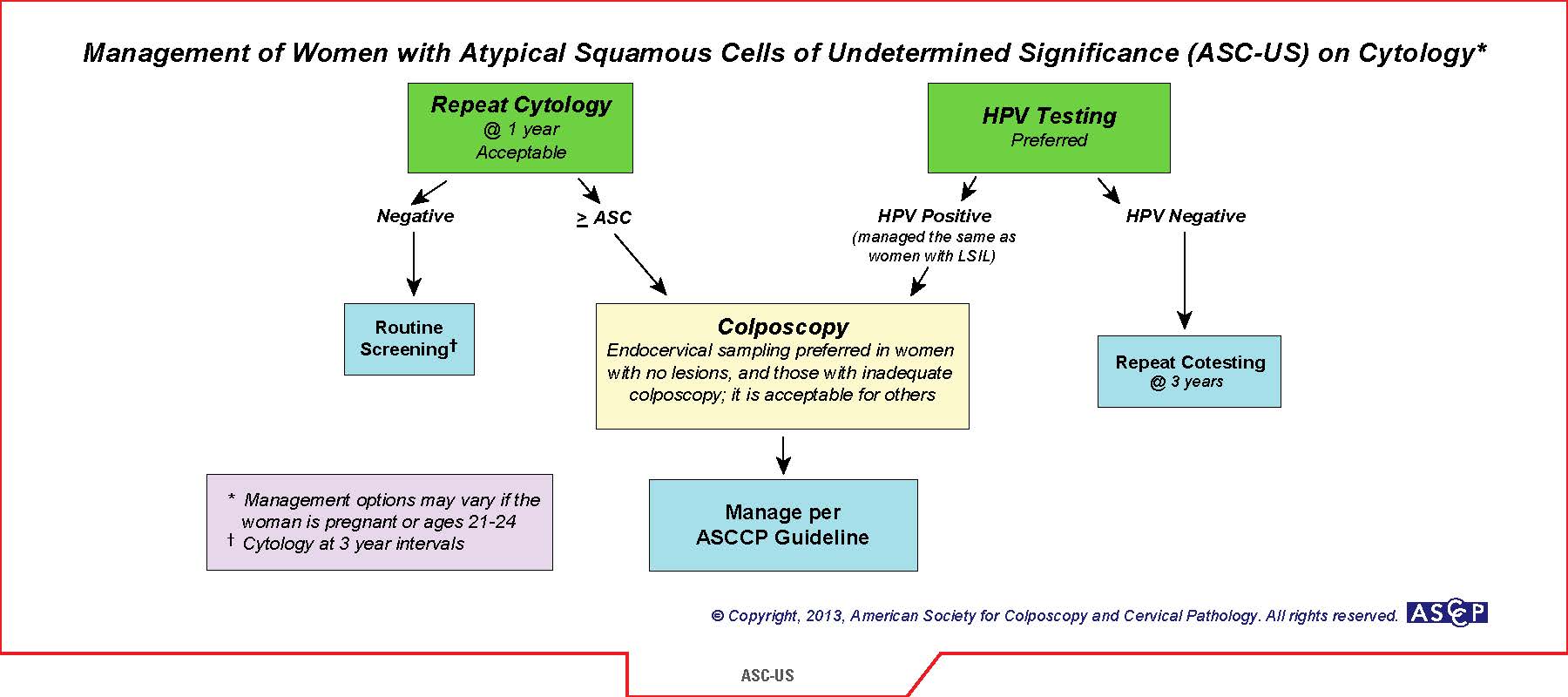
Next best step: Reflex HPV cotesting
Follow-up Recommendations: 3 years
Atypical squamous cells of undetermined significance (ASC-US) is a common “abnormal” pap result. The 2012 American Society of Clinical Pathologist (ASCP) recommend that women ages 21-29 should have routine cytology alone performed every 3 years as long as the results are normal. If ASC-US results, then reflex HPV contesting is recommended. If HPV (-), then return to routine cytology in 3 years. If HPV (+), then proceed to colposcopy. Another acceptable option is to have the patient return to clinic in 1 year for repeat pap. If ASC-US (+) again, then proceed to colposcopy. The logic is that most women in this age group clear any HPV infection without the need for colposcopy. This is the safer choice if the patient is wanting to have more children to limit any complications of cervical incompetence.
References
1) American Society of Clinical Pathologists. Screening Guidelines. Available at: http://www.asccp.org/guidelines/screening-guidelines.

Definition of Gestation/Pregnancy-Induced Hypertension
Epidemiology
Pathophysiology
This is still unknown but several theories exist and include:
Risk Factors
Fetal Well-being
Laboratory Evaluation
Preeclampsia
Management
Revolves around 3 main factors:

Broekhuijsen K, et al. Lancet. 2015;385(9986):2492-501.
HYPITAT-II Trial (HYPertension and Preeclampsia Intervention At Term)
Non-severe (<160/110mmHg) and no preeclampsia
Severe (>160/110mmHg) and no preeclampsia

Preeclampsia

Hauth JC, et al. Obstet Gynecol. 200;95(1):24-8.
Long-term Prognosis
References
1) ACOG Task Force on Hypertension in Pregnancy. Obstetrics & Gynecology. 2013;122(5).


