***LISTEN TO THE PODCAST HERE***
Guest Information

Wes Johnson, MSPAS, PA-C, (soon to be), DHSc was a former student of mine at UAB and was a respiratory therapist prior to PA school. He is the Regional Director of Clinical Education for Island Medical Management Emergency group in North Alabama. He won the Preceptor of The Year award from UAB in 2016 and currently finishing up his doctorate degree from A.T. Still University.
Twitter – @wesj2288
Disclaimer
For the purposes of this podcast and post, we will be using the Puritan Bennett 840 ventilator (pictured below). All the term we use are synonymous with all vents, but the screens will be different.

Puritan Bennett 840
Big Concepts of The Ventilator
- Mode
- Assist Control (AC)
- Every breath is either a machine driven (set by rate) or fully assisted (initiated by the patient)
- Uses either pressure (ACPC) or volume (ACVC)
- Every breath is either a machine driven (set by rate) or fully assisted (initiated by the patient)
- Synchronized Intermittent Mechanical Ventilation (SIMV)
- Set number of machine driven breaths, and patient intitated breaths are partially assisted
- Pressure Support (PS)
- No machine driven breaths and all breaths are initiated by the patient and partially assisted
- Assist Control (AC)
- Delivery
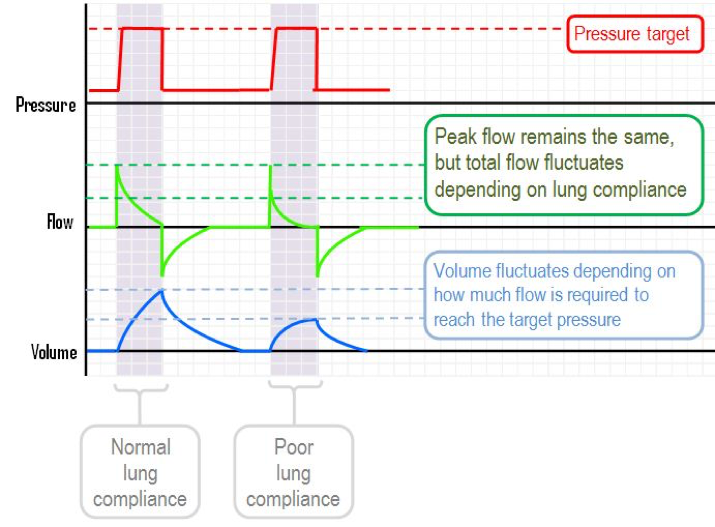
- Pressure
- Static Controls
- Pressure
- Time (inspiratory)
- Peak flow
- Variable Factors
- Volume
- Total flow

- Static Controls
- Volume
- Static Controls
- Tidal volume (cc)
- Flow (L/min)
- Variable Factors
- Pressure

- Static Controls
- Pressure
- Positive End Expiratory Pressure (PEEP)
- The pressure left in the circuit at the end of expiration
- Prevents alveolar collapse and improves oxygenation
- Can cause barotrauma and affect hemodynamics



Static Controls
(For this section, refer back to the vent picture above)
- Fraction of Inspired Oxygen (FiO2)
- Start at 100% and titrate down to 21%
- f (machine breath rate)
- Control
- Pressure Control (PC)
- Inspiratory pressure (Pi)
- Peak pressure in circuit
- Initial setting = < 20 cm H20
- Inspiratory time (I-time)
- Initial setting = 1.25 seconds
- Inspiratory pressure (Pi)
- Volume Control (VC)
- Vt (tidal volume of each breath)
- Initial setting = 6-8 cc/kg IBW
- Vmax (flow rate)
- Vt (tidal volume of each breath)
- Pressure Control (PC)
- Spontaneous Support
- Trigger for spontaneous support
- Volume = V-trig

- Pressure = P-trig

- Pressure Support (PS)
- I was always taught at least 5 cm H20 to overcome circuit resistance
- Trigger for spontaneous support


Real-Time Controls
- Flashing “C” and “S”
- Lets you know what breaths are controlled (machine) or spontaneous (patient)
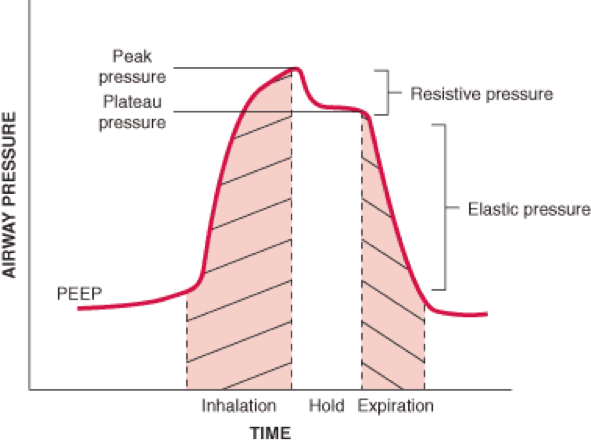
- Airway Pressure
- Ppeak (max airway pressure)
- A marker of resistance
- Pmean (average airway pressure)
- A measure of alveolar pressure
- Pplat (small airway and alveoli pressure)
- A measure of compliance


- Ppeak (max airway pressure)
- fTotal (machine + spontaneous breaths)
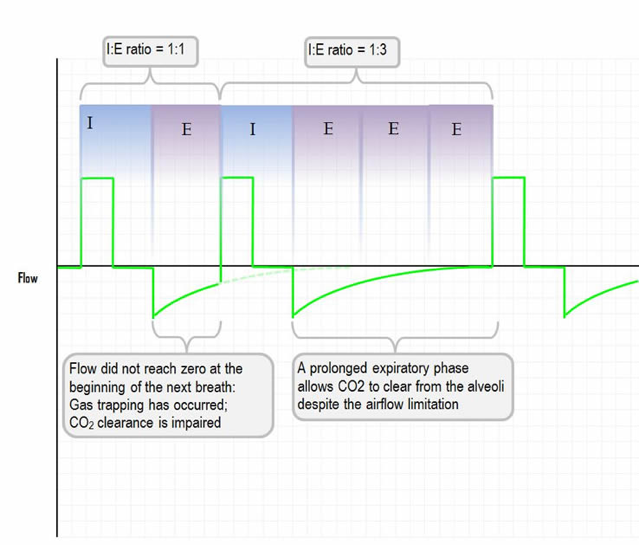
- I:E (inspiratory:expiratory ratio)
- Normal = 1:2 (at rest)
- Inverse ratio (2:1) can improve oxygen due to intention auto-PEEP


Wes Johnson’s Approach to Setting Up a Ventilator (after RSI)
Mode: AC
Vt: 6-8 mL/kg based on pt’s IBW
Rate: 12-16 bpm
FiO2: 100%
PEEP: 5.0
At the 5-minute mark:
- Check an ABG
- Titrate FiO2 off of PaO2 and pulse oximeter
- Adjust minute ventilation off of PaCO2 and/or ETCO2
References
- Respiratory Review YouTube Channel https://www.youtube.com/channel/UCtaRF58UDVthvH36YYCttng
- Deranged Physiology. Mechanical Ventilation. http://www.derangedphysiology.com/main/core-topics-intensive-care/mechanical-ventilation-0
- Weingart SD – “Spinning Dials – How to Dominate the Ventilator” – https://emcrit.org/wp-content/uploads/vent-handout.pdf
-
Weingart SD. Managing Initial Mechanical Ventilation in the Emergency Department. Annals of emergency medicine. 2016; 68(5):614-617. [pubmed]
- Air Link Regional West – “Initial Adult Ventilator Settings” – https://www.rwhs.org/sites/default/files/airlink-factsheet-ventsettings.pdf
- Open Anesthesia. Modes of Mechanical Ventilation. https://www.openanesthesia.org/modes_of_mechanical_ventilation/
- Modern Medicine Network. A Quick Guide to Vent Essentials. http://www.modernmedicine.com/modern-medicine/content/tags/copd/quick-guide-vent-essentials
-
Tobin MJ. Extubation and the myth of “minimal ventilator settings”. American journal of respiratory and critical care medicine. 2012; 185(4):349-50. [pubmed]