Definition – Hyperthyrodism caused by antibodies that stimulate T3/T4 secretion. The most common antibodies are thyroid-secreting hormone (TSH) and thyrotropin receptor antibody (TRAb).
Clinical Significance – Classic clinical manifestations of hyperthyroidism include thyromegaly, ophthalmaopathy, resting tremor, palpitations, weight loss, heat intolerance. For more in depth analysis of hyperthyroidism, see my 2017 talk at ASPA here.
History –Named after Robert James Graves (1796-1853), who was an prolific Irish physician, surgeon, and educator. He was named Regius professor of the Institute of Medicine in Trinity College, founded the Dublin Journal of Medical and Chemical Sciences, and was a an early adopter of clinical bedside rounding and teaching with medical students. Dr. Graves wrote a routine clinical lecture series in the London Medical and Surgical Journal and first described a young female patient with ophthalmopathy and goiter in 1835. Dr. Armand Trousseau then published the collection of these articles in 1864 entitled “Clinical Lectures on the Practice of Medicine” and gave him this eponym. Another contribution of Dr. Graves was the creation of the second hand on watches to time pulses and the practice of providing food and water with patients with a fever, instead of the common practice of withholding nourishment.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
What the two main sub-types of diabetes insipidus and how do you differentiate between the two?
What are the two lesser known sub-types?
Answer
The two main types of diabetes insipidus (DI) are central and nephrogenic. The hallmark of DI is deficiency of vasopressin and you can think of central DI as an ABSOLUTE deficiency and nephrogenic as a RELATIVE deficiency. Meaning, in central DI there is a problem with secretion of vasopressin from the posterior pituitary. The kidneys are fine, there just isn’t any vasopressin to make the kidneys hold onto water. In nephrogenic DI, there is plenty of circulating vasopressin (due to feedback to a normally functioning pituitary), but the kidneys are not responding to this stimulus. Central DI is most commonly caused by head trauma, post-neurosurgery, or autoimmune issues. Nephrogenic DI is most commonly caused by genetic defects in children, or renal problems in adults. A simple test to differentiate between central and nephrogenic DI is a desmopressin challenge. You can give desmopressin IN or SQ and measure urine osmolarity and volume every 30 minutes for 2 hours. In central DI, you should see a decrease in urine volume and increase in urine osmolarity. In nephogenic DI, nothing will change.
There are 2 other sub-types of DI that you need to be aware of as well. Gestational DI, which is considered a form of nephrogenic DI, can occur in the second/third trimester of pregnancy. This manifests as a transient ADH resistance due to increased vasopressinase from the placenta. The other subtype of DI is dipsogenic DI, which is a result of either a defect in the thirst center of the hypothalamus, or due to mental illness, which causes near constant polydipsia and polyuria. This basically overpowers the circulating ADH
References
Robertson GL. Diabetes insipidus: Differential diagnosis and management. Best practice & research. Clinical endocrinology & metabolism. 2016; 30(2):205-18. [pubmed]
Aleksandrov N, Audibert F, Bedard MJ, Mahone M, Goffinet F, Kadoch IJ. Gestational diabetes insipidus: a review of an underdiagnosed condition. Journal of Obstetrics and Gynaecology Canada. 2010; 32(3):225-31. [pubmed]
Perkins RM, Yuan CM, Welch PG. Dipsogenic diabetes insipidus: report of a novel treatment strategy and literature review. Clinical and experimental nephrology. 2006; 10(1):63-7. [pubmed]
Other Known Aliases – Capsula glomeruli, glomerular capsule
Definition – Double walled, cup-like capsule surrounding the glomerulus
Clinical Significance –It is made up of two poles: a vascular pole (afferent and efferent arterioles) and a urinary pole (proximal convoluted tubule). Within the capsule, there is a parietal layer and visceral layer with a space in between. This is where ultrafiltration takes place and urine is filtered from the blood.
History –Named after Sir William Bowman (1816-1892), who was an English ophthalmologist, histologist, and anatomist, and first identified this structure in 1841. He published his findings at the age of 25 and was awarded The Royal Medal by the Royal Society of London.
He was well known for his extensive use microscopes in visualizing structures of the human body and publishing two works with his mentor, Robert Bentley Todd, entitled “Physiological Anatomy and Physiology of Man” and “Cyclopaedia of Anatomy and Physiology”.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
These questions stemmed from an email I got from a former student about electrolyte questions they are getting in the clinical year. These are a quick and basic overview of common electrolyte questions and issues students may see on clinical rotations
#1 – Clinical Repletion of Electrolytes and Monitoring
Not every electrolyte on the chemistry panel needs to be repleted when low…but you need to know which ones can cause problems. The problem children are:
Potassium
Calcium
Magnesium
Phosphorus
Why? These four can all cause cardiac dysrhythmias when low and why all these should be on telemetry, or at least some basic monitoring, when repleting.
Your first step should ALWAYS ALWAYS ALWAYS be to make sure you know why it is low. Yes, we can keep repleting electrolytes to normal levels, but you will be doing this in perpetuity unless you fix the problem causing it in the first place. Let’s review the major points for each:
Hypokalemia
Major Cause – Diuretics, GI losses
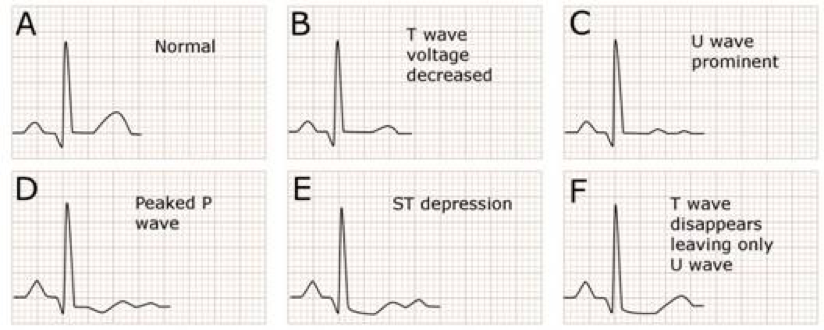
EKG Changes – Flat T-waves, U-wave. ST-depression
Repletion Pearls
Asymptomatic
Oral replacement – KCl 10-40 mEq 2-4 times per day
Major Causes – Hyperparathyroidism, Refeeding Syndrome, Hungry Bone Syndrome
Major Sequelae – ATP depletion, hemolysis
Repletion Pearls
Asymptomatic
Oral sodium/potassium phosphate 30-80 mmol/day
Symptomatic
IV sodium/potassium phosphate 10-40 mmol/day
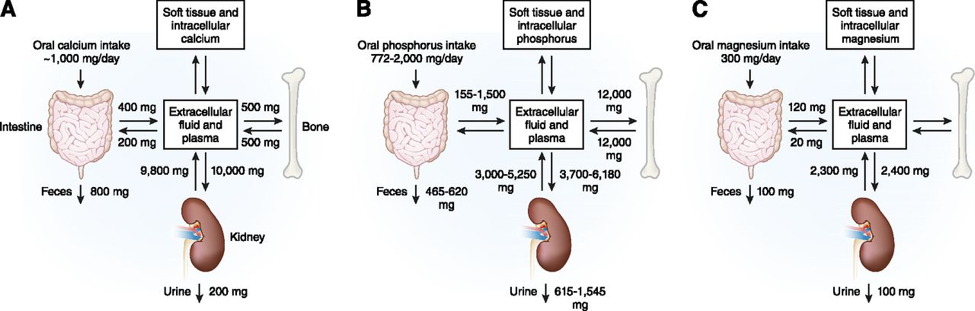
#2 – Calcium/Magnesium/Phosphorus Relationship
You must have a good understanding of this relationship when managing electrolyte deficiencies because you may not be able to make any headway on one if you don’t fix the other.
Magnesium and Calcium/Potassium
Hypomagnesemia causes functional hypoparathyroidism by inducing PTH resistance and decreasing calcium secretion and increasing calcium excretion.
Hypomagnesemia also causes cellular expression of ROMK channels in the nephron which increase potassium excretion
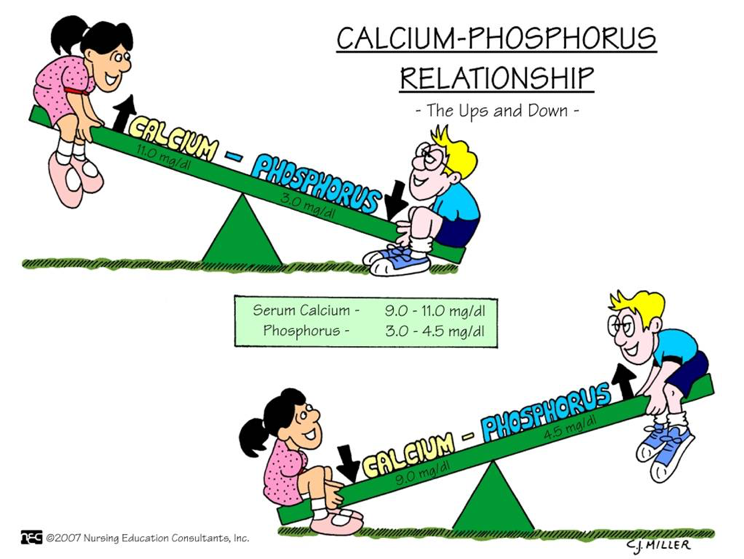
Calcium and Phosphorus
There is an inverse relationship between calcium and phosphorus because of PTH. As PTH increases (seen as a response to hypocalcemia), there is an increase in phosphorus excretion
#4 – Hyponatremia Pearls
Hyponatremia is actually really easy to work up. If you find you patient has a low sodium, check a serum osmolarity, urine osmolarity, and urine sodium.
References
Maday KR. Understanding electrolytes: important diagnostic clues to patient status. JAAPA. 2013; 26(1):26-31. [pubmed]
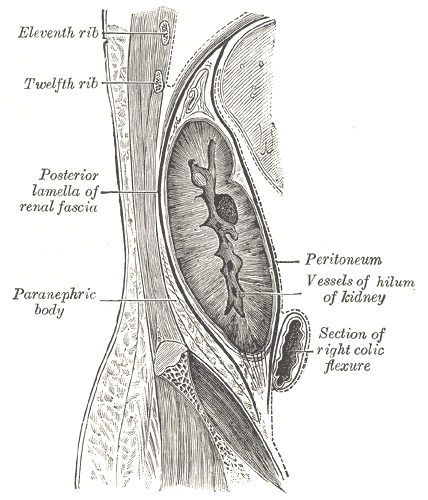
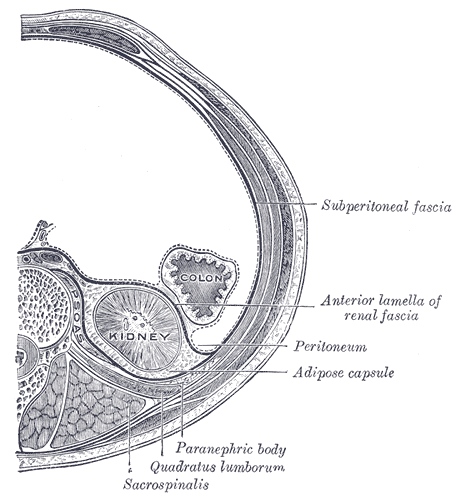
Definition – Connective tissue layers covering the kidneys and adrenal glands
Clinical Significance – This connective tissue encapsulates these organs and must be excised to perform nephrectomies and adrenalectomies. It has 4 attachments:
Anterior attachment – Connects the anterior layer of the renal fascia of the opposite kidney.
Posterior attachment – Connects the psoas fascia and the body of the vertebrae.
Superior attachment – The anterior and posterior layers fuse at the upper pole of the kidney and then split to enclose the adrenal gland. At the upper part of the adrenal gland they again fuse to form the suspensory ligament of the adrenal gland and fuse with the diaphragmatic fascia.
Inferior attachment – The posterior layer descends downwards and fuses with the iliac fascia. The anterior layer blends with the connective tissue of the iliac fossa.
History –Named after Dimitrie D. Gerota (1867-1939), who was a Romanian physician and professor of surgical anatomy and experimental surgery at the University of Bucharest. He was also the first radiologist in Romania and developed a method for injecting lymphatic vessels known as “The Gerota Method”
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Definition – Autoimmune disease that can effect the entire system…most commonly skin, joints, and constitutional.
Clinical Significance – For this eponym, there is no clinical significance. Just a cool fact I wanted to bring up….
History – You may have been wondering (or maybe not) where the “lupus” part of this disease comes from. Having studied Latin in high school all four years, this perplexed me in PA school because “lupus” is Greek for wolf. So why did early physicians decide on throwing “wolf” into the disease title?
Well (since you asked), it has been attributed to the 13th century Rogerius (who practiced with his friend, Stevius) who thought the characteristic erosive, dermatologic skin findings were similar to the effects of a wolf bite.
For those fellow PotterHeads out there, now you know the foreshadowing of (my favorite character) Remus LUPIN in the series.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Blotzer JW. Systemic lupus erythematosus I: historical aspects. Maryland State Medical Journal. 1983; 32(6):439-41. [pubmed]
Bertino LS, Lu LC. The bite of a wolf: systemic lupus erythematosus. Rehabilitation nursing : the official journal of the Association of Rehabilitation Nurses. 1993; 18(3):173-8. [pubmed]
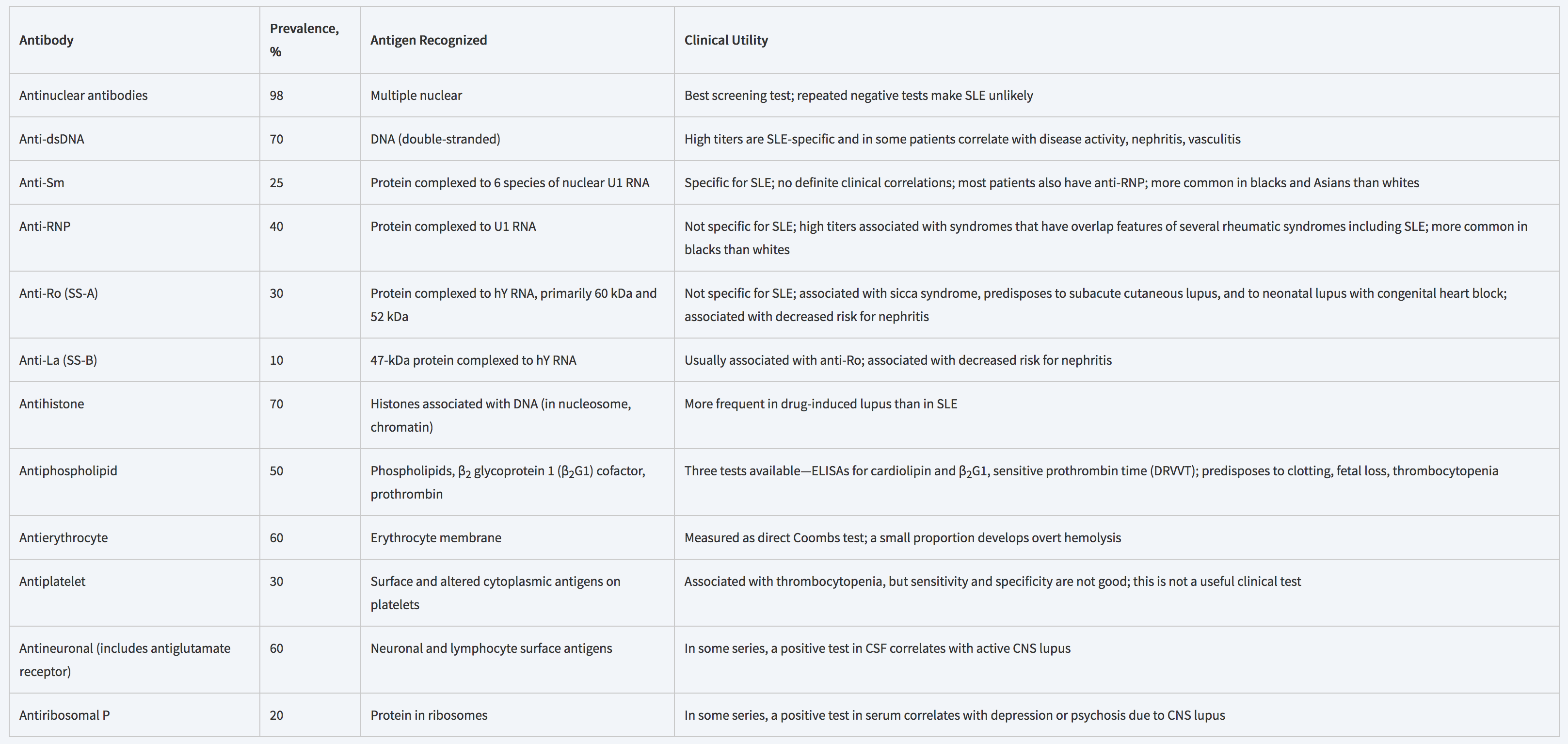
Anti-dsDNA is the MOST SPECIFIC for SLE when positive, but ANA is MOST SENSITIVE. This is why ANA is the antibody is used for screening and anti-dsDNA is used for confirming.
200,000-300,000 estimated new cases each year in the United States
Cause of approximately 10% of total hip replacements
Mean age at time of diagnosis is < 50 years
Pathogenesis and Etiologies
Current thoughts on exact mechanisms are an area of hot debate, but include:
Genetic predisposition
Metabolic factors
Vascular factors
Vascular damage
Increased intraosseous pressure
Mechanical stresses
80% of all atraumatic cases of AVN are due to:
Glucocorticoid Use
Theories
Microemboli in the arteries of the bone from alterations in lipid metabolism
Increased bone marrow adipocyte size and number causing decreased venous outlow
Changes venous endothelial cells of the bone leading to stasis and necrosis
Dose of prednisone < 15-20 mg/day has lowest risk of developing AVN (<3%)
Alcohol Use
Causes fat emboli, venous stasis, elevated cortisol, and adipocyte hyperrophy
While not considered an absolute risk factor, it is associated with up to 31% of AVN cases
Trauma can also predispose patients to develop AVN and most commonly associated with:
Femoral neck fracture
Hip dislocations
Other atraumatic causes of AVN include sickle cell disease, Gaucher disease, decompression disease, treatment for ALL, and transplantation
Signs and Symptoms
Pain
Groin, thigh, and/or buttock pain
Worse with weightbearing or motion
Although 2/3rd may have rest pain
1/3rd may have night pain
Decreased ROM with forced internal rotation and abduction
Limp
Imaging
Plain Radiographs
May not see any changes early in disease course
Progression of changes
Decreased density –> sclerosis –> subchondral radiolucency (crescent sign) and collapse
Magnetic Resonance Imaging
Much more sensitive than plain films
May see early changes undetectable on plain radiographs
T1 – Signal low-density line differentiating healthy and ischemic bone
T2 – Second high-density line showing hypervascular granulation
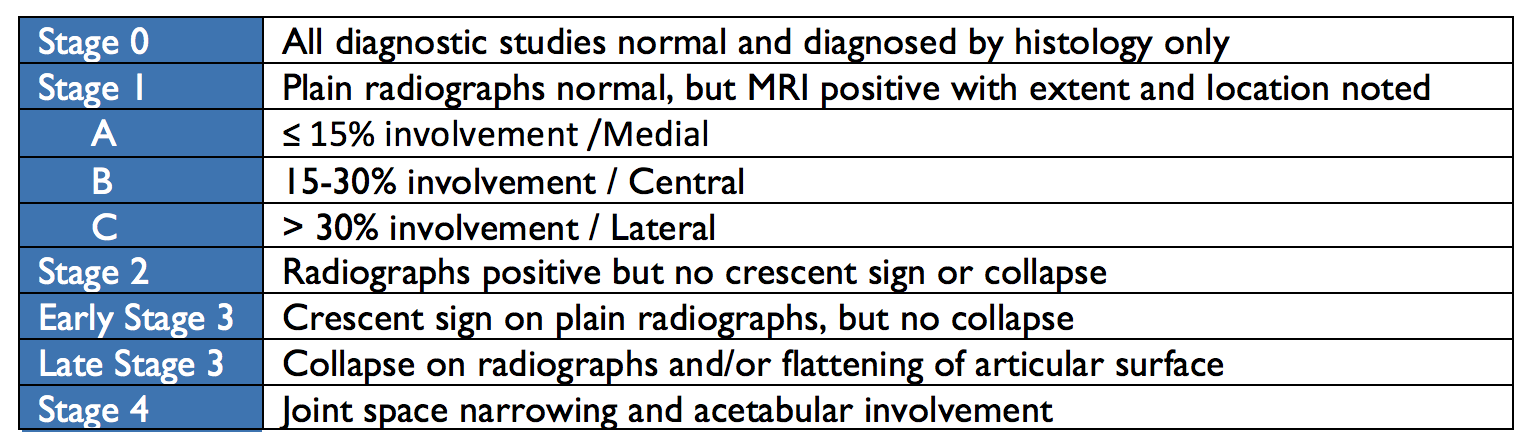
Classification and Staging
In 1993, The Association of Research Circulation Osseous (ARCO) staging system for AVN was developed to unify descriptions for treatment and research purposes.
Treatment
The goal of treatment is to preserve the native joint for as long as possible.
Nonoperative Management
Generally ineffective at halting the process
Includes bed rest, partial weightbearing, and pharmacotherapeutics
Bisphosphonates
Slows bone resorption
Vasodilators
Decrease intraosseous pressure and improve blow flow
Statins
Anticoagulants
Joint-Preserving Procedures
Core Decompression
Drills holes into femoral neck decrease pressure and allow for neovascularization
Displacement of the capital femoral epiphysis from the neck of the femur through the physeal plate anterolaterally and superiorly
Risk Factors
Obesity is #1 risk factor
> 60% of patients in > 90th percentile for weight
Renal failure
History of radiation therapy
Endocrine abnormalities
Hypothyroidism, GH deficiency
Signs and Symptoms
The most common clinical presentation of SCFE are pain and altered gait, but can be divided into four presentation patterns:
Preslip
(+) pain, but no radiographical displacement of epiphysis
May show widening of the physis
Acute
< 3 weeks duration
(+) joint effusion but no metaphyseal remodeling
10-15% of initially presentation of hip pain and often associated with trauma
Acute-on-chronic
Worsening symptoms in known SCFE
Chronic
Most common pattern of presentation
Vague, intermittent symptoms > 3 weeks
(+) metaphyseal remodeling but no effusion
Pain is classically characterized as dull, aching in the hip, groin, thigh, or knee. Physical exam reveals decreased internal rotation and abduction ROM with increased pain. Passively flexing the affected hip while the leg is extended will cause external rotation and abduction.
Stability
Stable Slips
Walking and weightbearing still possible with or without crutches
Unstable Slips
No ability to weightbear, even with crutches
No examination of the ROM of the hip should occur until orthopaedic consultation
Radiographic Evaluation
Most SCFE are diagnosed by plain radiography and have characteristic findings on each view:
AP view
Mild, widening, lucency, and irregularity of the physis
Blurring of the junction between metaphysis and growth plate
Klein’s Line
Normal = intersecting lateral portion of femoral head from superior femoral neck
SCFE = line passes outside of epiphysis
Lateral View
Usually obtained via frog-leg or cross-table
Unstable SCFE should have true lateral
Posterior displacements are best seen on lateral views
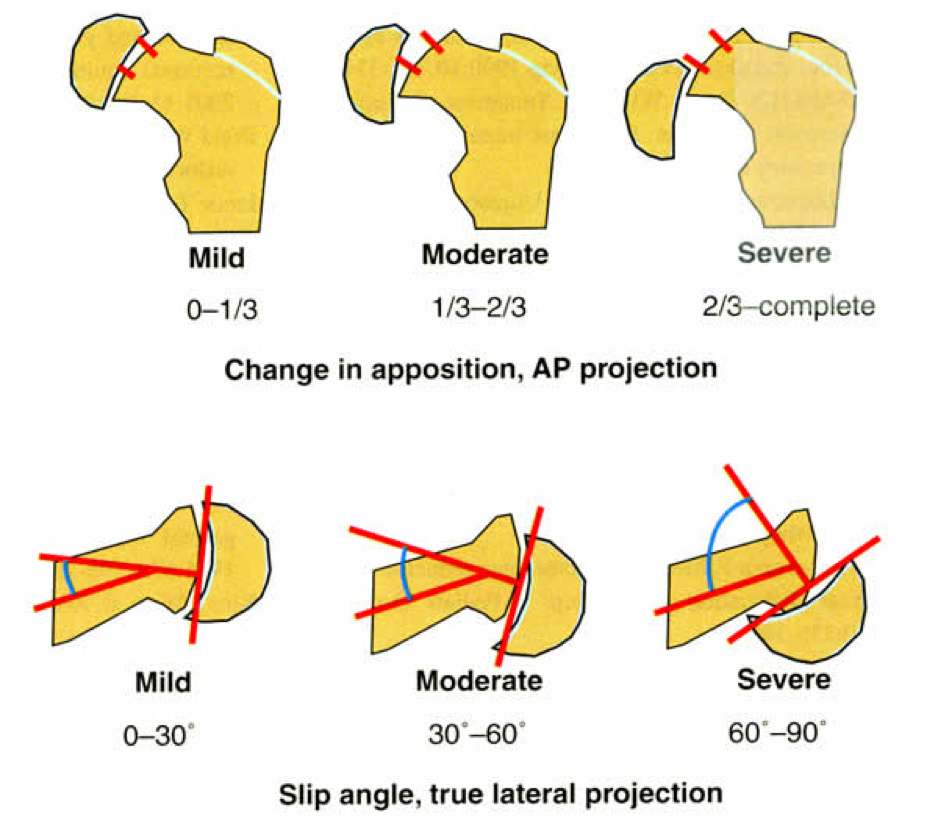
Grading of Severity
2 ways to grade severity: Displacement of femoral neck or Angle of Southwick.
Displacement
Mild = < 1/3rd the diameter of the femoral neck
Moderate = > 1/3rd, but < 2/3rd the diameter of the femoral neck
Severe = > 2/3rd the diameter of the femoral neck
Angle of Southwick
Mild = < 30o
Moderate = 30-60o
Severe = > 60o
Treatment
All SCFEs must be repaired surgically and the goals of surgery are to stabilize the diseased physis to prevent further slippage and avoid complications (AVN). Treatment of choice is a single cannulated screw placed in the center of the epiphysis.
References
Moya-Angeler J, Gianakos AL, Villa JC, Ni A, Lane JM. Current concepts on osteonecrosis of the femoral head. World Journal of Orthopedics. 2015; 6(8):590-601. [pubmed]
Mankin HJ. Nontraumatic necrosis of bone (osteonecrosis). The New England journal of medicine. 1992; 326(22):1473-9. [pubmed]
Jones JP. Fat embolism and osteonecrosis. The Orthopedic clinics of North America. 1985; 16(4):595-633. [pubmed]
Dilisio MF. Osteonecrosis following short-term, low-dose oral corticosteroids: a population-based study of 24 million patients. Orthopedics. 2014; 37(7):e631-6. [pubmed]
Fukushima W, Fujioka M, Kubo T, Tamakoshi A, Nagai M, Hirota Y. Nationwide epidemiologic survey of idiopathic osteonecrosis of the femoral head. Clinical orthopaedics and related research. 2010; 468(10):2715-24. [pubmed]
Shigemura T, Nakamura J, Kishida S. The incidence of alcohol-associated osteonecrosis of the knee is lower than the incidence of steroid-associated osteonecrosis of the knee: an MRI study. Rheumatology (Oxford, England). 2012; 51(4):701-6. [pubmed]
Slobogean GP, Sprague SA, Scott T, Bhandari M. Complications following young femoral neck fractures. Injury. 2015; 46(3):484-91. [pubmed]
LaPorte DM, Mont MA, Mohan V, Jones LC, Hungerford DS. Multifocal osteonecrosis. The Journal of rheumatology. 1998; 25(10):1968-74. [pubmed]
Mont MA, Hungerford DS. Non-traumatic avascular necrosis of the femoral head. The Journal of bone and joint surgery. American volume. 1995; 77(3):459-74. [pubmed]
Loder RT. The demographics of slipped capital femoral epiphysis. An international multicenter study. Clinical orthopaedics and related research. 1996; [pubmed]
Benson EC, Miller M, Bosch P, Szalay EA. A new look at the incidence of slipped capital femoral epiphysis in new Mexico. Journal of pediatric orthopedics. 2008; 28(5):529-33. [pubmed]
Murray AW, Wilson NI. Changing incidence of slipped capital femoral epiphysis: a relationship with obesity? The Journal of bone and joint surgery. British volume. 2008; 90(1):92-4. [pubmed]
Koop S, Quanbeck D. Three common causes of childhood hip pain. Pediatric clinics of North America. 1996; 43(5):1053-66. [pubmed]
Causey AL, Smith ER, Donaldson JJ, Kendig RJ, Fisher LC. Missed slipped capital femoral epiphysis: illustrative cases and a review. The Journal of emergency medicine. 1995; 13(2):175-89. [pubmed]
Reynolds RA. Diagnosis and treatment of slipped capital femoral epiphysis. Current opinion in pediatrics. 1999; 11(1):80-3. [pubmed]