You are seeing an 8yo with his mother for increasing behavioral problems and decreasing school performance. She is concerned about ADHD because several of his friends have been diagnosed and are now on medications and doing well. On physical exam, he is not making consistent eye contact in the room, shows poor impulse control, and is does not want to speak with you when you ask him questions. You are now entertaining the possibility of an autism spectrum disorder.
What are the DSM-V diagnostic criteria for an autism spectrum disorder and what are some of the available testing tools?
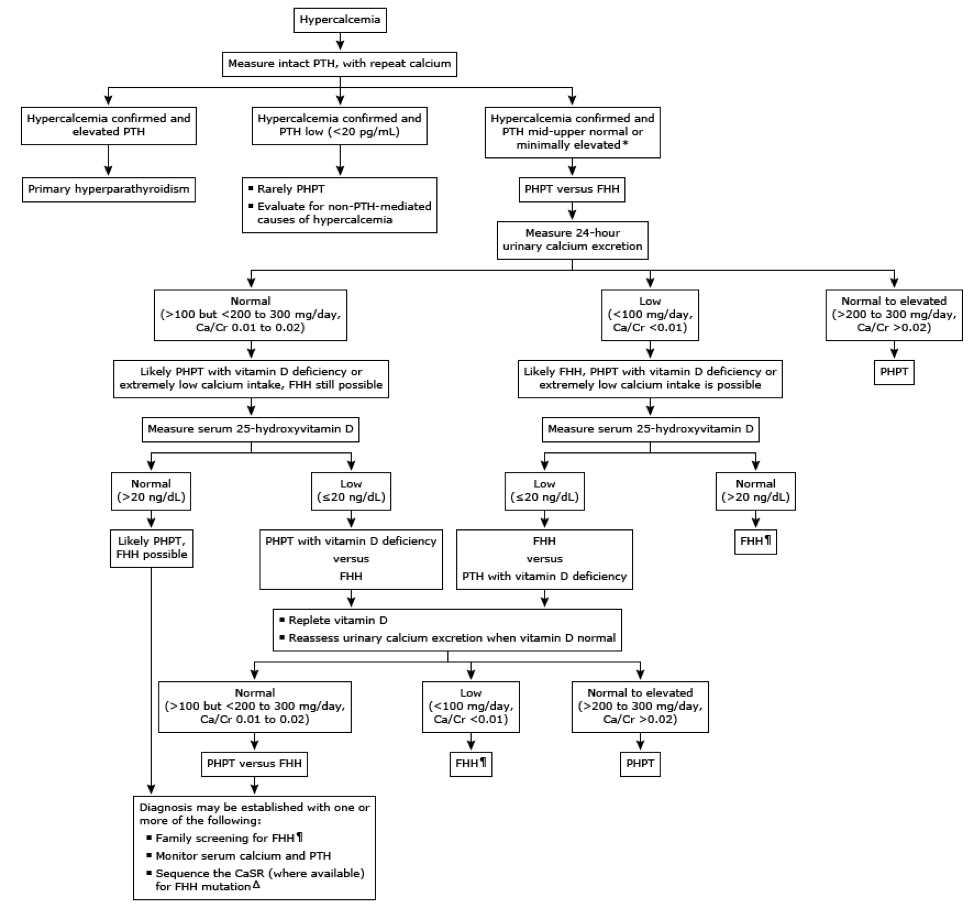
Allows for visualization of adenoma, hyperactive glands, or ectopic glands prior to surgery
Sensitivity – 70-81%, PPV – 91-95%
Procedure
Bilateral neck exploration
Medical
Bisphosphonates
Inhibits bone resorption and improves bone mass
Alendronate
Calcimimetics
Activate calcium-sensing receptors in the parathyroid gland, which decrease PTH secretion
Cinacalcet
Vitamin D
Secondary
Phosphate binders
Vitamin D supplementation
References
Potts JT, Juppner H. Parathyroid hormone: Molecular biology and regulation. In: Principles of Bone Biology, Bilezikian JP, Raisz LG, Rodan GA (Eds), Academic Press, San Diego 1996. p.325.
Diaz R, El-Hajj Fuleihan G, Brown EM. Regulation of parathyroid function. In: Handbook of Physiology, Section 7: The Endocrine System, Fray GGS (Ed), Oxford University Press, New York 1999.
Talmage RV, Mobley HT. Calcium homeostasis: reassessment of the actions of parathyroid hormone. General and Comparative Endocrinology. 2008;156(1):1-8. [pubmed]
van Abel M, Hoenderop JG, van der Kemp AW, Friedlaender MM, van Leeuwen JP, Bindels RJ. Coordinated control of renal Ca(2+) transport proteins by parathyroid hormone. Kidney International. 2005;68(4):1708-21. [pubmed]
Bartsch D, Nies C, Hasse C, Willuhn J, Rothmund M. Clinical and surgical aspects of double adenoma in patients with primary hyperparathyroidism. The British Journal of Surgery. 1995;82(7):926-9. [pubmed]
Ruda JM, Hollenbeak CS, Stack BC. A systematic review of the diagnosis and treatment of primary hyperparathyroidism from 1995 to 2003. Otolaryngology. 2005;132(3):359-72. [pubmed]
Rafferty MA, Goldstein DP, Rotstein L. Completion thyroidectomy versus total thyroidectomy: is there a difference in complication rates? An analysis of 350 patients. Journal of the American College of Surgeons. 2007;205(4):602-7. [pubmed]
Silverberg SJ, Bilezikian JP. Evaluation and management of primary hyperparathyroidism. The Journal of Clinical Endocrinology and Metabolism. 1996;81(6):2036-40. [pubmed]
Coker LH, Rorie K, Cantley L. Primary hyperparathyroidism, cognition, and health-related quality of life. Annals of Surgery. 2005;242(5):642-50. [pubmed]
Rastogi R, Beauchamp NJ, Ladenson PW. Calcification of the basal ganglia in chronic hypoparathyroidism. The Journal of Clinical Endocrinology and Metabolism. 2003;88(4):1476-7. [pubmed]
Stein R, Godel V. Hypocalcemic cataract. Journal of Pediatric Ophthalmology and Strabismus. 1980;17(3):159-61. [pubmed]
Kinirons MJ, Glasgow JF. The chronology of dentinal defects related to medical findings in hypoparathyroidism. Journal of Dentistry. 1985;13(4):346-9.[pubmed]
Goltzman D, Cole DEC. Hypoparathyroidism. In: Primer on the metabolic bone diseases and disorders of mineral metabolism, 6th ed, Favus MJ. (Ed), American Society of Bone and Mineral Research, Washington, DC 2006. p.216.
Winer KK, Ko CW, Reynolds JC. Long-term treatment of hypoparathyroidism: a randomized controlled study comparing parathyroid hormone-(1-34) versus calcitriol and calcium. The Journal of Clinical Endocrinology and Metabolism. 2003;88(9):4214-20. [pubmed]
Bilezikian JP, Brandi ML, Eastell R. Guidelines for the management of asymptomatic primary hyperparathyroidism: summary statement from the Fourth International Workshop. The Journal of Clinical Endocrinology and Metabolism. 2014;99(10):3561-9. [pubmed]
Eslamy HK, Ziessman HA. Parathyroid sctinigraphy in patients with primary hyperparathyroidism: 99mTc sestamibi SPECT and SPECT/CT. Radiographics. 2088;28:1461-1476.
What are the indications for high-intensity statin therapy for hyperlipidemia?
New joint guidelines were released in 2013 by ACC/AHA on the management of hyperlipidemia. In these guidelines, there are 3 criteria for high intensity statin therapy:
Age < 75 years with a clinical Atherosclerotic Cardiovascular Disease (ASCVD):
What are the drugs and dosing for high-intensity statin therapy?
There are only 2 medications that have been studied that are recommended for high-intensity statin therapy:
Atorvastatin 40-80mg daily
Rosuvastatin 20-40mg daily
2013 ACC/AHA Hyperlipidemia Guidelines
Knowmedge
Reference
Stone NJ, Robinson JG, Lichtenstein AH. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. 63(25 Pt B):2889-934. 2014. [pubmed]
The prostate begins to enlarge in the 4th decade of life with a significant jump in the 6th decade of life. Mean prostate weight in normal men < 30yo is around 20g and steadily increases after this. Volume of the prostate also steadily increases after the 4th decade with symptoms typically starting to manifest once it reaches 30cc3.
Up-To-Date. 2016
Risk Factors
Race
African Americans are at higher risk of requiring surgery
Asians have the lowest risk of requiring surgery
Prostatitis
Associated with increased risk of BPH
Pathogenesis of BPH
The main areas of the prostate that contribute to BPH are the periurethral (transitional zone) of the prostate and the hyperplastic nodules that develop are primarily comprised of stromal cells. The specific pathogenesis of BPH is still not completely understood and only 2 variables that have been identified as essential for BPH development: age and functioning Leydig Cells of the testes. Androgens, estrogens, inflammation, genetics, and stromal growth factors have all been studied and have variable results.
De Marzo. 2007.
Clinical Manifestations of BPH
The signs of symptoms of BPH can be broken down into 3 main categories:
Storage Symptoms
Urgency
Daytime frequency
Nocturia
Urgency incontinence
Voiding Symptoms
Slow, urinary stream
Splitting or spraying of the urinary stream
Intermittent urinary stream
Urinary hesitancy
Straining to void
Terminal dribbling
Post-micturition Symptoms
Incomplete bladder voiding
Post micturition dribble
Differential Diagnosis of BPH Symptoms
Urethral stricture or bladder neck contracture
Previous history of catheterization or instrumentation
Urethral trauma
Urethritis
Neurogenic bladder
Other signs and symptoms of neurologic disease
Bladder calculi
History of nephrolithiasis
Carcinoma of the bladder or prostate
Hematuria
Previous history of cancer
Urinary tract infection and prostatitis
Dysuria
Fever
Medications
Antcholinergics (decreases bladder function)
Sympathomimetics (increases outflow resistance)
International Prostate Symptom Score
The original AUA score was developed in 1992 and is used to assess the severity of symptoms of BPH, BUT NOT FOR DIFFERENTIAL DIAGNOSIS. This is a seven-part questionnaire that evaluates symptoms on a 0-5 scale and then calculates the symptoms as mild, moderate, or severe. An eight question was added to evaluate quality of life.
International Prostate Symptom Score
Work-Up
Physical Exam
Digital Rectal Exam (DRE) should be performed to assess size, contour, regularity, and nodularity
Laboratory Testing
Urinalysis
Initial test to evaluate for microscopic hematuria and infection
Basic Metabolic Profile
BUN/Creatinine
Evaluate baseline renal function
Serum Prostate Specific Antigen (PSA)
PSA and prostate volume have a log-linear relationship
DOES NOT CORRELATE WITH CANCER
Uroflowmetry Study
Optional testing per AUA
Can evaluate maximal urinary flow rate
Patient voids with a full bladder (> 150cc)
< 15ml/s = outflow obstruction
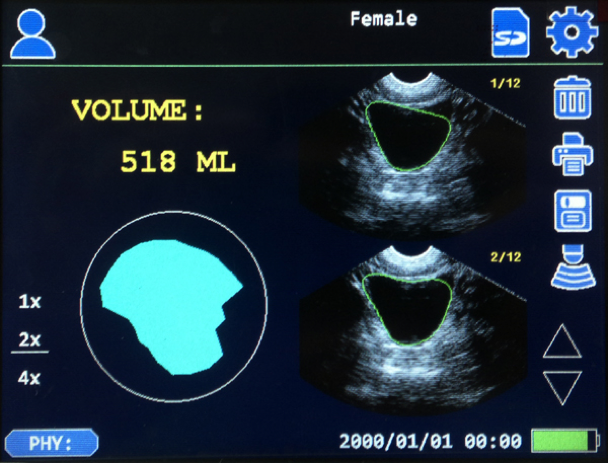
Post-void Residual Urine Volume
Bladder scan is least invasive and most common
Normal men have < 12mL of residual urine post-void
Management
BPH can be managed by PCP if the patient has mild symptoms (low IPSS ≤ 7) and no complications.
Indications for urology referral are:
Symptoms with autonomic or peripheral neuropathy
Symptoms following invasive treatment of the urethra or prostate
Age < 45yo
Abnormality of prostate on DRE
Presence of hematuria in the absence of infection
Incontinence
Severe symptoms (IPSS ≥ 20)
Treatment
Medical
Alpha-1-adrenergic antagonists
Mechanism of Action
Relax smooth muscle of bladder neck, prostate capsule, and prostatic urethra
Side effects
Hypotension
Drugs
Terazosin (need to titrate)
Doxazosin (need to titrate)
Tamsulosin
5-alpha-reductase inhibitors
Used if patients can’t tolerate hypotension of alpha-1-adrenergic antagonists
Need 6-12 months of treatment to see effects
Mechanism of Action
Reduce prostate size by preventing the conversion of testosterone to the more potent dihydrotestosterone
Drugs (no difference due to EPICS trial)
Finasteride
Dutasteride
Combination Alpha-1/5-Alpha Therapy
Indications
Severe symptoms (IPSS ≥ 20)
Large prostate (> 40cc)
Inadequate response to maximal monotherapy
Drugs
Doxazosin/finasteride
Tamsulosin/dutasteride
Surgical
Indications
Moderate/severe symptoms (IPSS ≥ 8) with high quality of life score (≥ 4)
Hyponatremia as a result of the systemic absorption of the hypotonic irrigation solution
Sexual Dysfunction
Ejaculatory Dysfunction
Erectile Dysfunction
Urethral Stricture
Urinary Incontinence
Cottage Physician
References
Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. The Journal of Urology. 1984;132(3):474-9. [pubmed]
Bosch JL, Hop WC, Kirkels WJ, Schröder FH. Natural history of benign prostatic hyperplasia: appropriate case definition and estimation of its prevalence in the community. Urology. 1995;46(3 Suppl A):34-40. [pubmed]
Sidney S, Quesenberry CP, Sadler MC, Guess HA, Lydick EG, Cattolica EV. Incidence of surgically treated benign prostatic hypertrophy and of prostate cancer among blacks and whites in a prepaid health care plan. American Journal of Epidemiology. 1991;134(8):825-9. [pubmed]
Kang D, Andriole GL, Van De Vooren RC. Risk behaviours and benign prostatic hyperplasia. BJU International. 2004;93(9):1241-5. [pubmed]
St Sauver JL, Jacobson DJ, McGree ME, Girman CJ, Lieber MM, Jacobsen SJ. Longitudinal association between prostatitis and development of benign prostatic hyperplasia. Urology. 2008;71(3):475-9; discussion 479. [pubmed]
Rohr HP, Bartsch G. Human benign prostatic hyperplasia: a stromal disease? New perspectives by quantitative morphology. Urology. 1980;16(6):625-33. [pubmed]
De Marzo AM, Platz EA, Sutcliffe S. Inflammation in prostate carcinogenesis. Nature Reviews. Cancer. 2007;7(4):256-69. [pubmed]
Jones C, Hill J, Chapple C, . Management of lower urinary tract symptoms in men: summary of NICE guidance. BMJ (Clinical research ed.). 2010;340:c2354. [pubmed]
Barry MJ, Fowler FJ, O’Leary MP. The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. The Journal of Urology. 1992;148(5):1549-57; discussion 1564. [pubmed]
McVary KT, Roehrborn CG, Avins AL. Update on AUA guideline on the management of benign prostatic hyperplasia. The Journal of Urology. 2011;185(5):1793-803. [pubmed]
Roehrborn CG. The utility of serum prostatic-specific antigen in the management of men with benign prostatic hyperplasia. International Journal of Impotence Research. 2008;20 Suppl 3:S19-26. [pubmed]
Oelke M, Bachmann A, Descazeaud A. EAU guidelines on the treatment and follow-up of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. European Urology. 2013;64(1):118-40. [pubmed]
Chapple CR. Pharmacological therapy of benign prostatic hyperplasia/lower urinary tract symptoms: an overview for the practicing clinician. BJU International. 2004;94(5):738-44. [pubmed]
McVary KT, Roehrborn CG, Avins AL. Update on AUA guideline on the management of benign prostatic hyperplasia. The Journal of Urology. 2011;185(5):1793-803. [pubmed]
Nickel JC, Gilling P, Tammela TL, Morrill B, Wilson TH, Rittmaster RS. Comparison of dutasteride and finasteride for treating benign prostatic hyperplasia: the Enlarged Prostate International Comparator Study (EPICS). BJU International. 2011;108(3):388-94. [pubmed]
McConnell JD, Roehrborn CG, Bautista OM. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of benign prostatic hyperplasia. NEJM. 2003;349(25):2387-98. [pubmed]
Roehrborn CG, Siami P, Barkin J. The effects of combination therapy with dutasteride and tamsulosin on clinical outcomes in men with symptomatic benign prostatic hyperplasia: 4-year results from the CombAT study. European Urology. 2010;57(1):123-31. [pubmed]
The Urology Book. urologybook.com. Accessed September 12, 2016.
Gómez Sancha F, Bachmann A, Choi BB, Tabatabaei S, Muir GH. Photoselective vaporization of the prostate (GreenLight PV): lessons learnt after 3500 procedures. Prostate Cancer and Prostatic Diseases. 2007;10(4):316-22. [pubmed]
22yo male presents to emergency department with a 2-hour history of increasingly intense testicular pain. He reports being sexually active with multiple partners and intermittent condom use. He is a very active person and completed a triathlon the day before presentation. He denies dysuria, urethral discharge, or flank pain, but did have an episode of vomiting prior to arrival. He is in visible distress and can not seem to get comfortable. Evaluation of the scrotum reveals a tender, swollen left testicle.
What are some bedside maneuvers you can perform to help with the differential?
Epididymitis
Point tenderness over the superior aspect of the testicle
(+) Prehn Sign
Manual elevation of the testicle improves pain
Testicular Torsion
High-riding and/or horizontal lie of testicle (“Bell Clapper Deformity)
Absent cremesteric reflex
Normal = pinching/stroking the thigh causes ipsilateral elevation of testicle
(-) Prehn Sign
Torsion of Appendix Testes
More common in children
(+) Blue Dot Sign
What should be the initial management of this patient?
If suspected epididymitis:
Urinalysis, urine culture, and gonorrhea/chlamydia testing
Antibiotics are directed towards:
C. trachomatis or N. gonorrhoeae
Ceftriaxone 250mg IM and doxycycline 100mg PO BID x 10 days
Gram-negative enteric pathogens
Levofloxacin 500mg PO daily x 10 days
If suspected testicular torsion:
Manual detorsion may be attempted
2/3 torse medially and detorsion is performed by rotating testicle outwards laterally
Ultrasound may be performed if immediately available (this should not delay surgical consult or evaluation)
Surgical evaluation and management is the preferred initial management of patients with suspected testicular torsion
If suspected torsion of appendix testes:
Ultrasound is performed to rule-out other pathologies.
Management is conservative with rest, ice, and NSAIDs.
Surgical removal may be required if pain does not improve with conservative management.
References
Tracy CR, Steers WD, Costabile R. Diagnosis and management of epididymitis. The Urologic Clinics of North America. 35(1):101-8; vii. 2008. [pubmed]
Galejs LE. Diagnosis and treatment of the acute scrotum. American Family Physician. 59(4):817-24. 1999. [pubmed]
Workowski KA, Bolan GA, . Sexually transmitted diseases treatment guidelines, 2015. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports / Centers for Disease Control. 64(RR-03):1-137. 2015. [pubmed]
Sessions AE, Rabinowitz R, Hulbert WC, Goldstein MM, Mevorach RA. Testicular torsion: direction, degree, duration and disinformation. The Journal of Urology. 169(2):663-5. 2003. [pubmed]
Palestro CJ, Manor EP, Kim CK, Goldsmith SJ. Torsion of a testicular appendage in an adult male. Clinical Nuclear Medicine. 15(7):515-6. 1990. [pubmed]
22yo male presents to emergency department with a 2-hour history of increasingly intense testicular pain. He reports being sexually active with multiple partners and intermittent condom use. He is a very active person and completed a triathlon the day before presentation. He denies dysuria, urethral discharge, or flank pain, but did have an episode of vomiting prior to arrival. He is in visible distress and can not seem to get comfortable. Evaluation of the scrotum reveals a tender, swollen left testicle.
What are some bedside maneuvers you can perform to help with the differential?
What should be the initial management of this patient?
This patient is ready for extubation. Everyone has their own magic numbers they want to see on the vent before they think about extubating a patient, but mine are:
Pressure support mode
every breath is initiated by the patient and only supported by the vent
Pressure support ≤ 8 cmH2O
This will be enough support to overcome the resistance in the circuit.
PEEP ≤ 7 cmH2O
Physiologic PEEP of the epiglottis is 5 cmH2O
FiO2 ≤ 40%
No more supplemental oxygen than what would be given via nasal cannula or open face mask
Stable ABG on these settings for at least 2 hours
A&Ox3 and following commands
Patients need to be able to participate in pulmonary toilet after the tube comes out
These are basic principles and there are many variables that go into deciding to extubate a patient. LITFL does a great review here and goes through a very systematic approach.
Once this is all good, then you can perform a few bedside tests or measurements that can help predict success of extubation.
Rapid Shallow Breathing Index (RSBI)
Respiratory Rate / Vt (L)
< 105 predicts successful extubation
Negative Inspiratory Force (NIF)
Measurement of the maximal inspiratory pressure
This is a great measurement of a patient’s ability to generate an adequate tidal volume once extubated.
> -20 cmH2O predicts successful extubation
Prediction of Successful Extubation. The ICU Book.
Yang KL, Tobin MJ. A prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilation. N Engl J Med. 1991;324(21):1445–50. [PubMed]
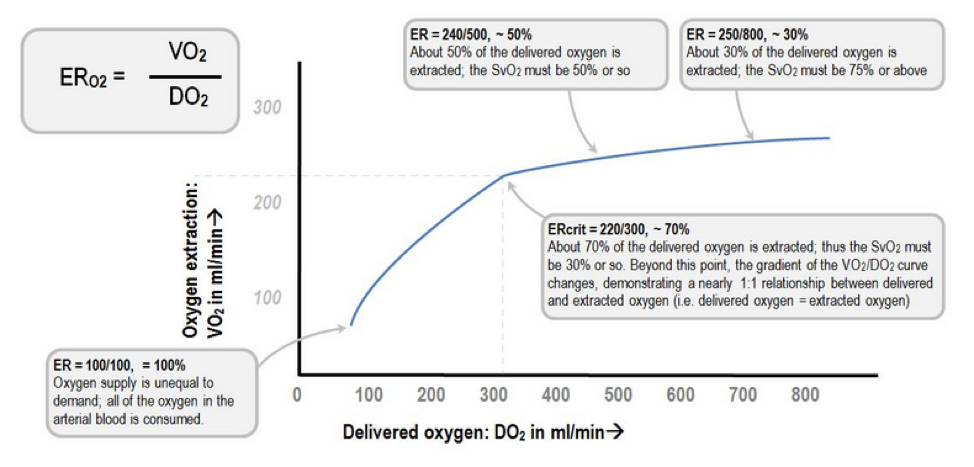
The definition of shock is a clinical state of cellular and tissue hypoxia/perfusion due to:
Reduced oxygen delivery
Increased oxygen consumption
Inadequate oxygen utilization
It basically comes down to the ratio between oxygen delivery (DO2) and oxygen extraction (VO2).
Extraction Ratio (ER)
Deranged Physiology
At the cellular level, shock hypoxemia causes cell membrane dysfunction leading to intracellular edema and leakage, as well inability to regulate cellular pH. This causes progressive acidemia, which in turn, have severe systemic effects on multiple organ systems.
Kherallah M.
Pathophysiology of Shock
BP = (HR x SV) x SVR
Factors effecting HR:
Autonomic regulation
Hormones
Fitness levels
Age
Medications
Factors effecting SV:
Preload
Contractility
Afterload
Factors effecting SVR:
Vessel length
Vessel diameter
Blood viscosity
Signs and Symptoms of Shock
As perfusion decreases and hypoxia starts, the body begins to compensate and the signs and symptoms of shock are generally a result of this compensation.
Classifications and Causes of Shock
UpToDate
How to Diagnose Shock
Laboratory studies should be performed very early in the screening process for a patient with suspected shock as it will help you determine the degree of end organ perfusion. These include:
Lactate (> 2 mmol/L)
Creatinine
LFTs
ABG or VBG
There has been a tremendous amount of advancement in the diagnosis and management of patients in acute shock. For years, the pulmonary artery catheter was the gold standard for critically ill patients admitted to the ICU. It allowed for serial “measurements” of almost all the hemodynamic parameters you needed (PACWP, CO, CI, SVR, PAP, SvO2), but it was not without serious complications. It still has it’s place for certain disease management, but it is no longer indicated for diagnosing the different types of shock. I bring this up only because these parameters can be helpful when learning the different shock states as you can focus on 3 main variables: PACWP, CO/CI, and SVR.
Point-of-Care ultrasonography (POCUS) has really become the test of choice for an undifferentiated shock patient, as it provides fast, vital information of the different causes of shock and allows for rapid rule-out of life-threatening conditions. There are several different types of POCUS algorithms used depending on the history and clinical context of the patient.
Rapid Ultrasound in Shock (RUSH) is used for undifferentiated patients. Scott Weingart does a great podcast on this technique here and Sinae EM Ultrasound did a step-by-step review here.
Another approach to undifferentiated shock is the Abdominal and Cardiac Evaluation with Sonography (ACES) protocol. It is used primarily in the UK and a good review can be found here.
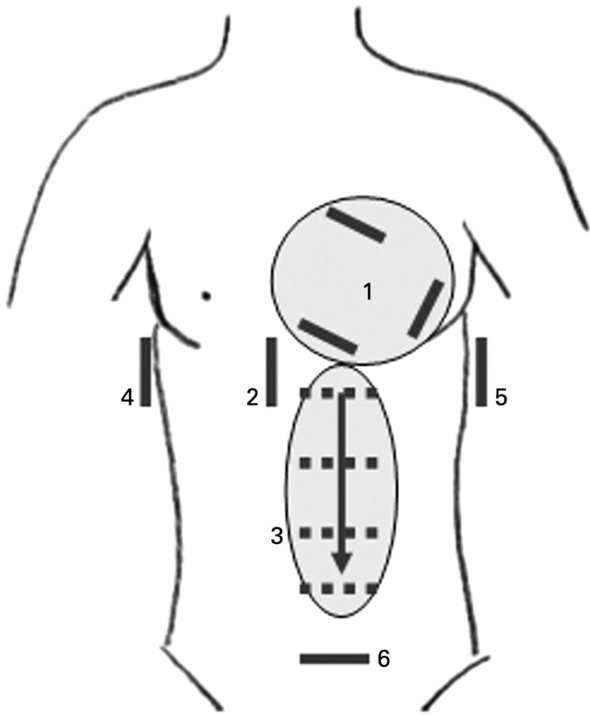
ACES Exam
Focus Assessed Transthoracic Echo (FATE) is a more detailed look at the heart to identify specific cardiac abnormalities.
If you have a trauma patient, you would use the Focused Assessment with Sonography for Trauma (FAST) exam to rapidly identify traumatic causes for hemorrhage and need for operative intervention.
Once you diagnose a patient with a specific type of shock, the management is pretty straight forward. If the patient is in hypovolemic, distributive, or obstructive shock, IV fluids should be used to improve perfusion and hemodynamics. The amount depends on the conditions, but usually starting with 1-2L of crystalloids is a good bet and then you can re-evaluate and repeat your ultrasound to look at the effects. If you have a trauma patient, then blood products should be started early on in the course until definitive control can be performed.
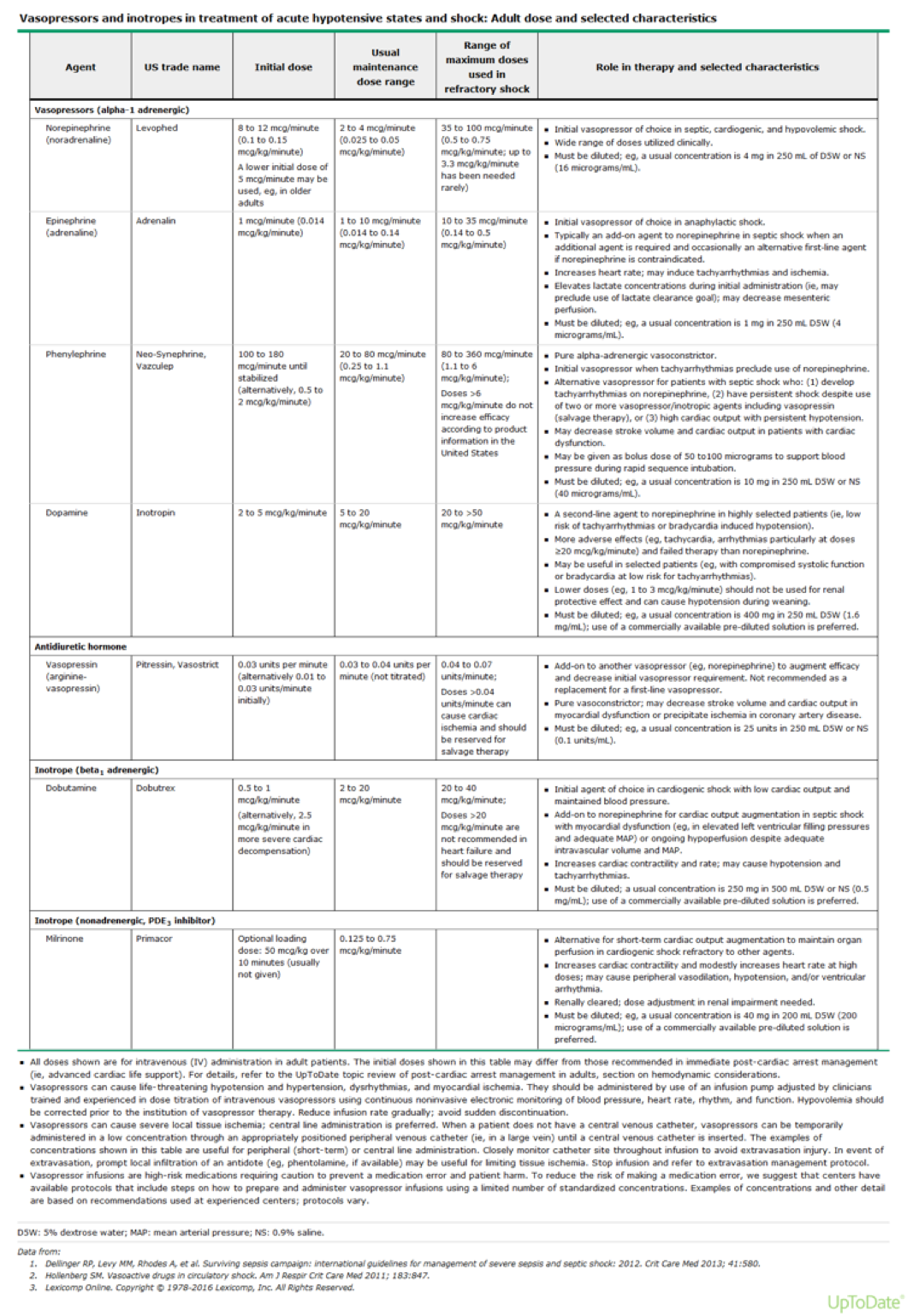
If adequate fluid resuscitation has not improved the hemodynamics or clinical picture, then pharmacologic agents are needed to improve perfusion. These can be broken down into vasopressors (increase vasomotor tone) and inotropes (increase contractility).
UpToDate
References
Vincent JL, De Backer D. Circulatory shock. NEJM. 369(18):1726-34. 2013. [pubmed]
Barber AE, Shires GT. Cell damage after shock. New horizons (Baltimore, Md.). 4(2):161-7. 1996. [pubmed]
Shah MR, Hasselblad V, Stevenson LW. Impact of the pulmonary artery catheter in critically ill patients: meta-analysis of randomized clinical trials. JAMA. 294(13):1664-70. 2005. [pubmed]
Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in Shock in the evaluation of the critically lll. Emergency medicine clinics of North America. 28(1):29-56, vii. 2010. [pubmed]
Weingart SD, Duque D, Nelson B. EmCrit Blog. Rapid Ultrasound for Shock and Hypotension – the RUSH Exam. Accessed 08/17/16. http://emcrit.org/rush-exam/
Labovitz AJ, Noble VE, Bierig M. Focused cardiac ultrasound in the emergent setting: a consensus statement of the American Society of Echocardiography and American College of Emergency Physicians. Journal of the American Society of Echocardiography. 23(12):1225-30. 2010. [pubmed]
Atkinson PR, McAuley DJ, Kendall RJ. Abdominal and Cardiac Evaluation with Sonography in Shock (ACES): an approach by emergency physicians for the use of ultrasound in patients with undifferentiated hypotension. Emergency medicine journal : EMJ. 26(2):87-91. 2009. [pubmed]
AIUM practice guideline for the performance of the focused assessment with sonography for trauma (FAST) examination. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 33(11):2047-56. 2014. [pubmed]
You are rounding on a ICU patient who has been on the ventilator for the past 4 days due to respiratory failure from community acquired pneumonia. She has been gradually weaned down to the following settings:
Pressure Support Mode
PEEP – 6 cmH2O
Pressure Support – 8 cmH2O
Oxygen – 0.40
She is A&Ox3 and follows commands. Vital signs show BP – 122/72 mmHg, HR – 78, RR – 15, O2 – 100%, Temp – 99.8.
What is your next step?
What bedside measurements or tests can you do to help with your decision?