Diagnosis: Acute rheumatic fever
Criteria: Jones criteria
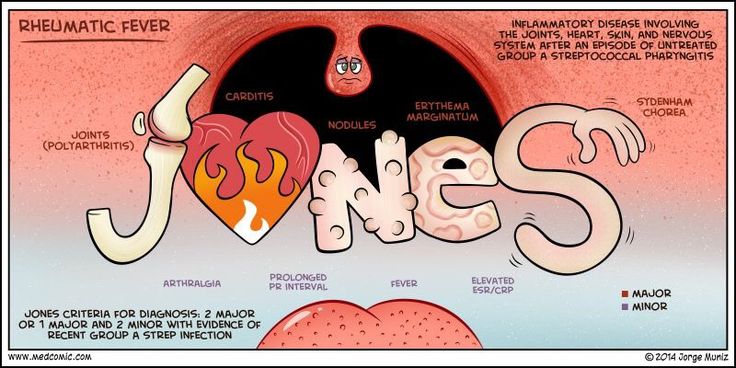
Acute rheumatic fever (ARF) is a sequella of symptoms that typically occur 2-4 weeks after an untreated bout of group A Streptoccocal (GAS) pharyngitis. Symptoms include arthritis, carditis, erythema marginatum, CNS symptoms, and subcutaneous nodules.
Jones criteria is constellation of symptoms of ARF and are subdivided into major and minor manifestations.
Major
Carditis
Arthritis
CNS involvement
Subcutaneous nodules
Erythema marginatum
Minor
Arthralgia
Fever
Elevated acute phase reactants
Prolonged PR interval
The diagnosis of ARF is made using the Jones criteria and is positive if the patient has evidence of a preceding GAS infection and:
- Two major manifestations
or
- One major and two minor manifestations