With finals week closely approaching, this weekend snuck up on me quick and I was not able to get a good case together for the blog….my bad.
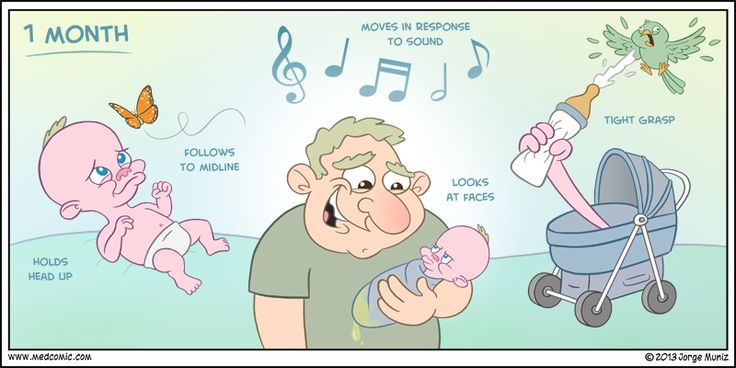
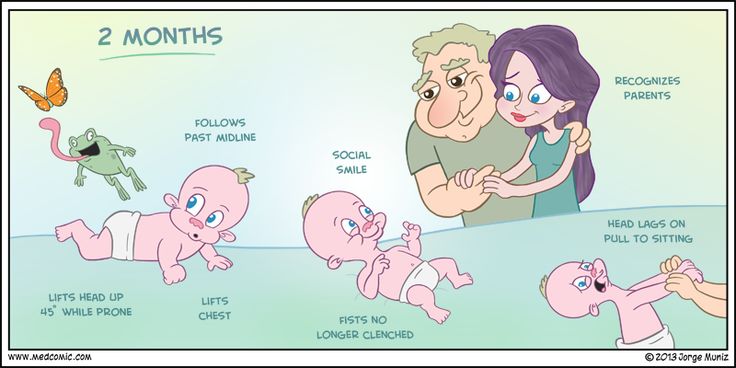
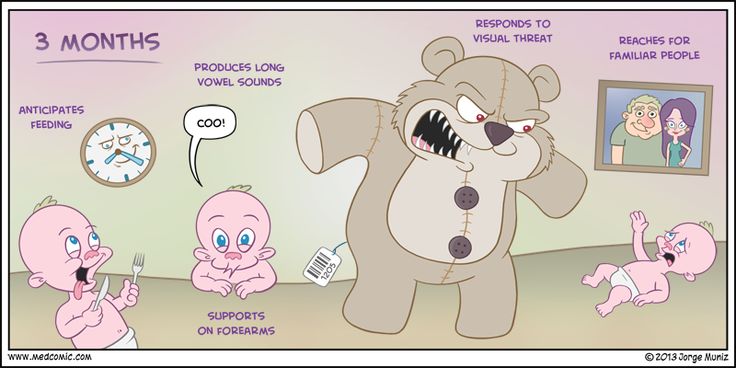
But, FEAR NOT!!!! What I thought I would do for the last post of pediatric month is review the pediatric developmental milestones by way of infographics.
If you haven’t already, you need to be following Jorge Muniz of Medcomic on Twitter and buy his book….it is awesome and he is a fellow PA. I try to incorporate as many of his images as possible when I teach.
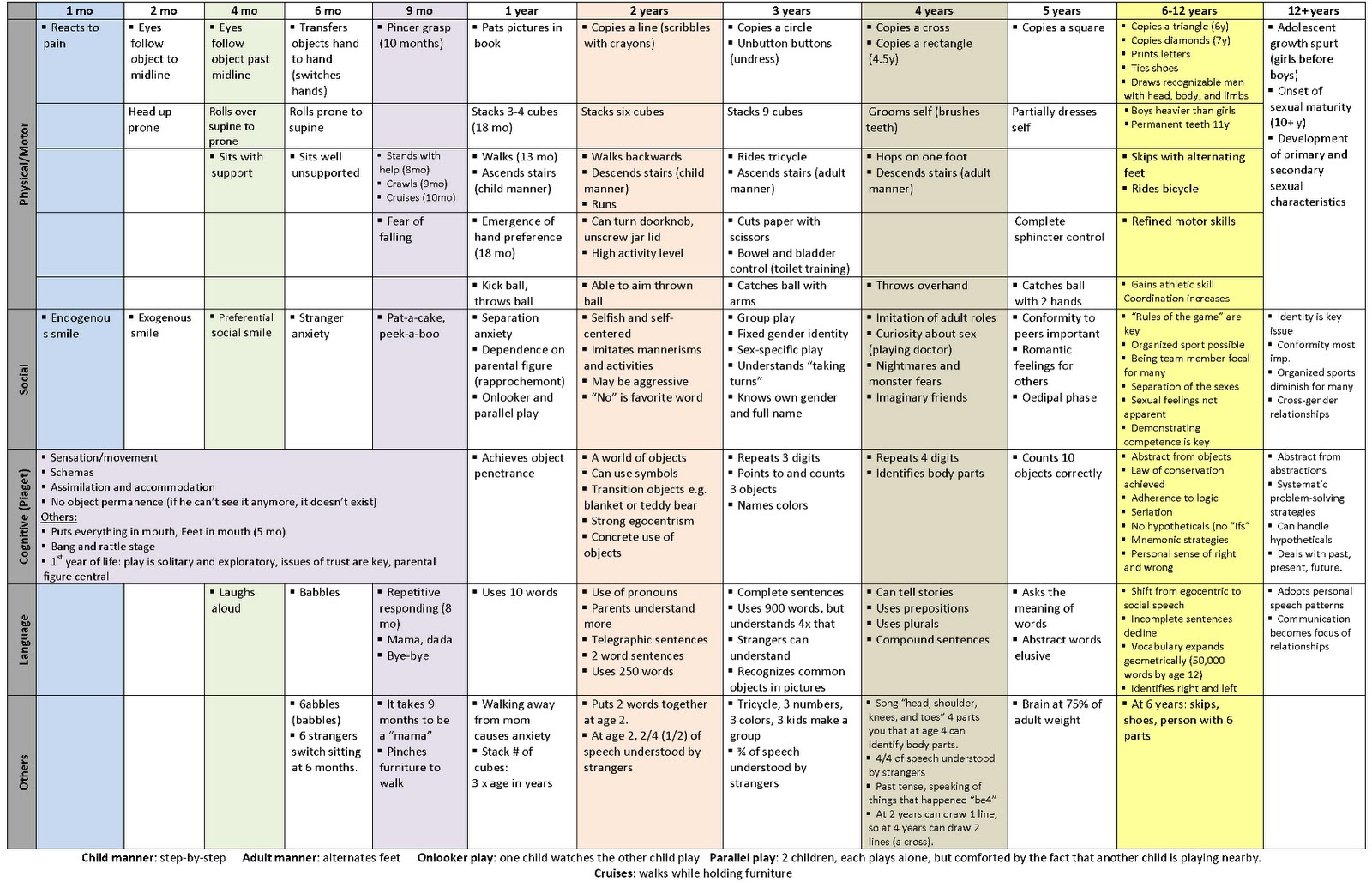
The last graphic is the THE BEST single graphic of developmental milestones (from 1 month to 12 years) I have ever found. Great resource for your pediatric rotation.
Comprise 15% of all CHD and 33% of potentially fatal CHD
Physiology
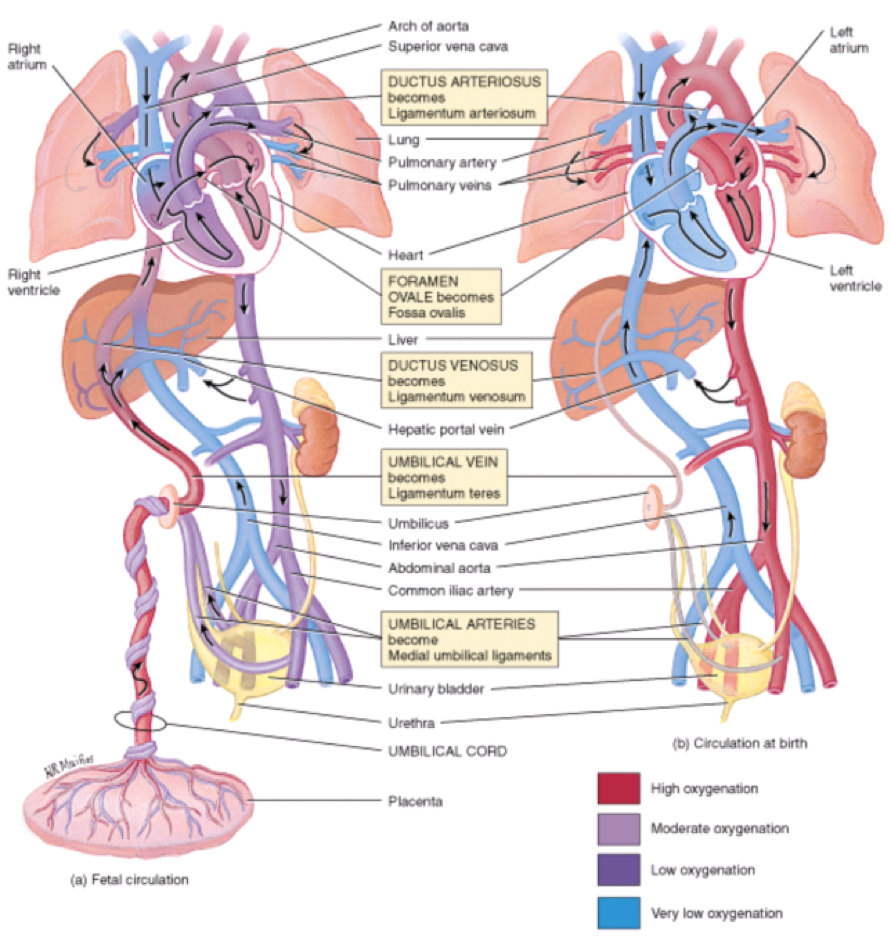
The cardiovascular system in-utero is a complicated machine that is designed to bypass the lungs and provide oxygenated blood from the placenta. There are two main structures that help maintain oxygenation when the fetus’ lungs are not used:
Ductus arteriosus
Connects the pulmonary artery to the descending aorta
Prostaglandin E1 and E2 are produced by the placenta and keep this open
Absolutely vital to remain patent in several of the cyanotic diseases to provide oxygenated blood
Foramen ovale
Communication between right and left atrium
Once the infant begins spontaneously breathing, increases in pulmonary blood flow and left atrial pressures mechanically seals the foramen ovale
Fetal circulation (a) in-utero and (b) during 1st 7 days of life
Khan Academy Tutorials
Cardiac Causes of Cyanosis
3 Main Physiologic Categories
Decreased pulmonary blood flow
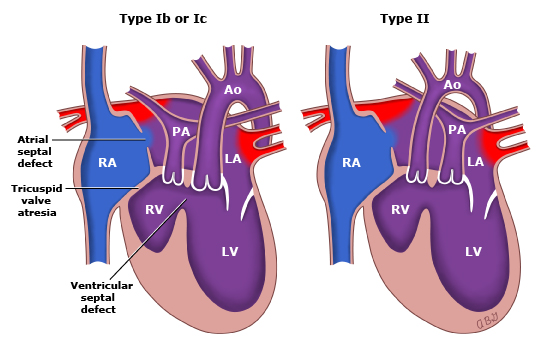
Tetralogy of Fallot, tricuspid atresia
Increased pulmonary blood flow
Transposition of great vessels, truncus arteriosis, total anomalous pulmonary venous connection
Severe heart failure
Hypoplastic left heart, coarctation of the aorta
Timing of Presentation
Within 48 hours of birth
Transposition of great vessels, tricuspid atresia
With 7 days of birth
Truncus arteriosus, total anomalous pulmonary venous connection, Tetralogy of Fallot
Screening
Hyperoxia Test
100% oxygen via hood for 10 minutes
Radial artery (preductal) PaO2 is measured
PaO2 > 150 mmHg suggests pulmonary disease
Pulse Oximetry Screening
Measuring the difference in SpO2 between preductal (right hand) and postductal (either foot) flow
A positive test warranting further investigation includes any of the following:
SpO2 < 90% in either extremity
SpO2 90-94% in both locations on three measurements one hour apart
SpO2 difference > 3% on three measurements one hour apart
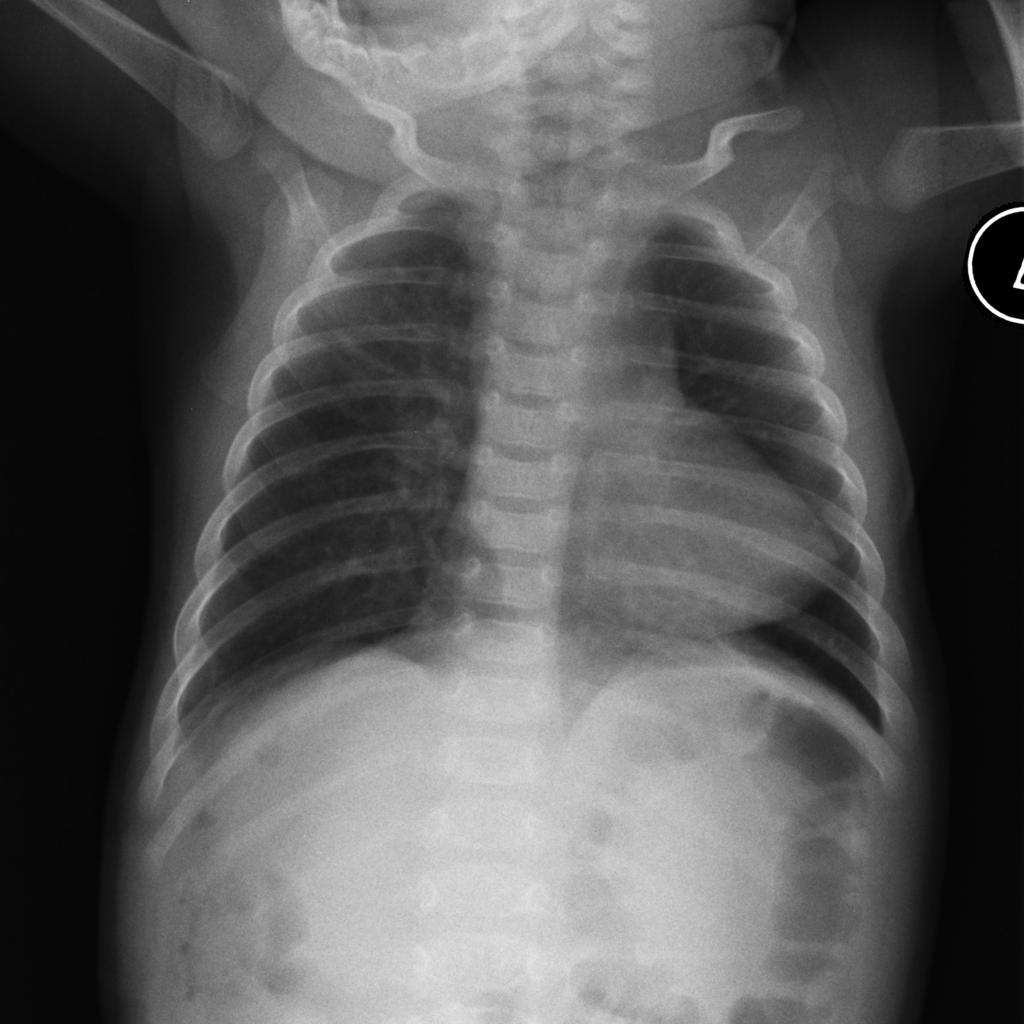
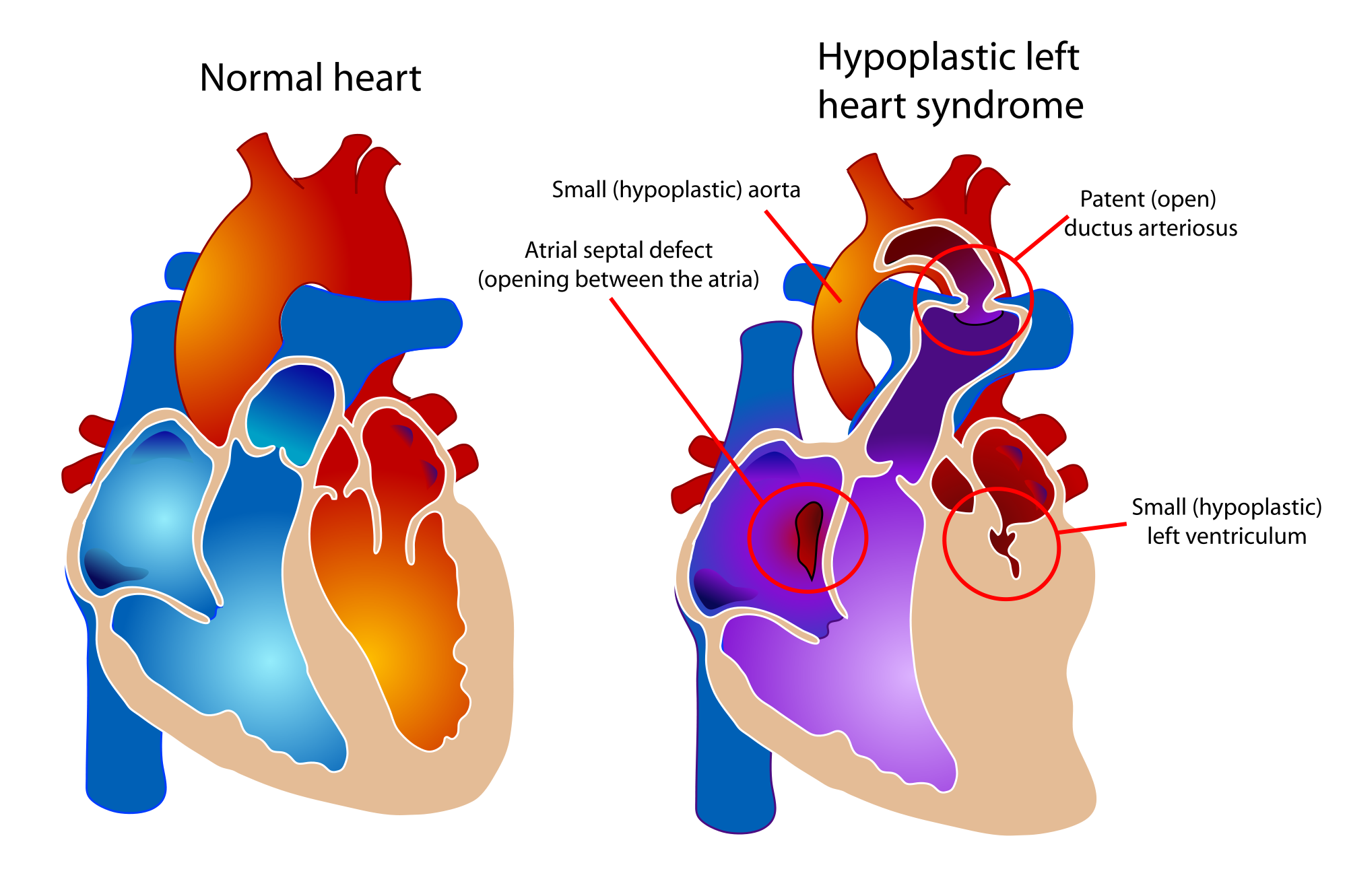
Spectrum of cardiac malformations characterized by underdevelopment of the left ventricle with atresia, stenosis, or hypoplasia of aortic and/or mitral valve, and hypoplasia of ascending aorta and arch
Survival is dependent on PDA and ASD
Signs and Symptoms
Prenatal
Can be diagnosed by fetal ultrasound between 18-24 weeks
Postnatal
“Honeymoon” period while PDA is open and ASD is unrestricted
May be discharged and present after 3-5 days
If ASD is restricted –> rapid decompensation as PDA closes
Single S2 heart sound
No murmur
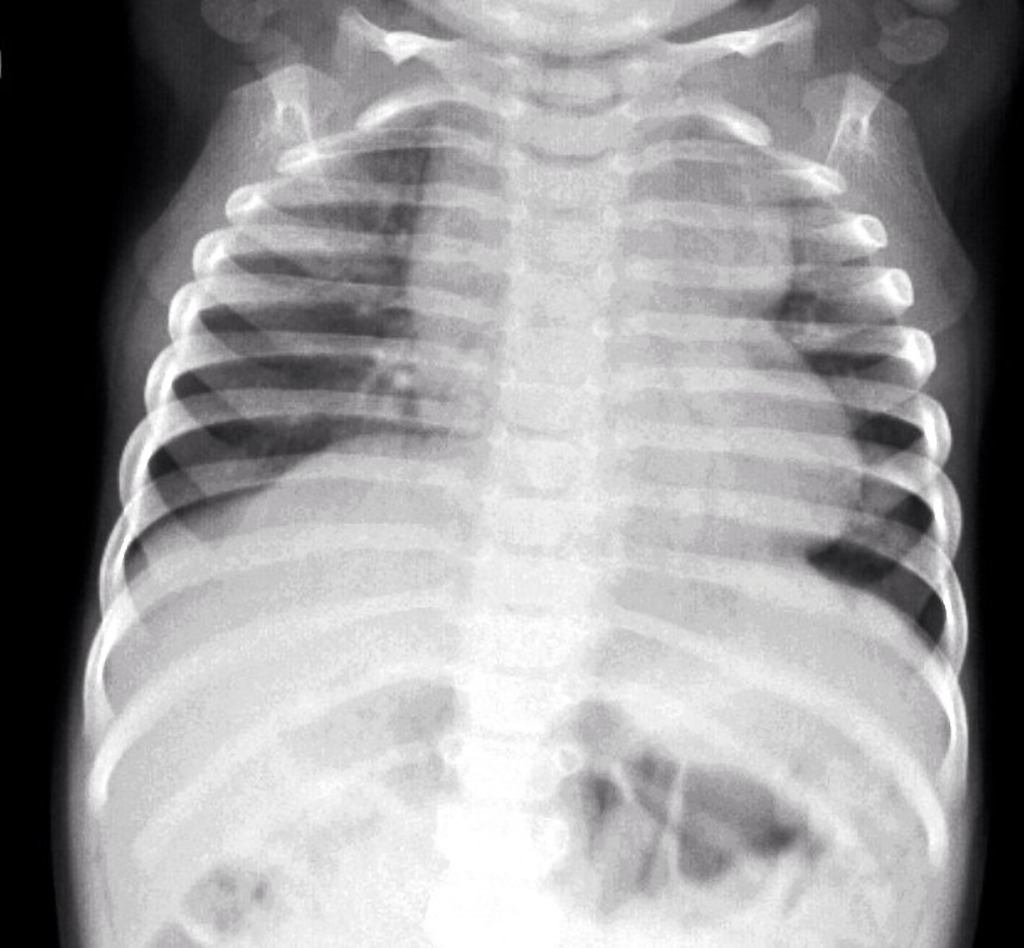
Chest radiograph may show small cardiac silhouette
Electrocardiogram shows RAD, RAE, RVH
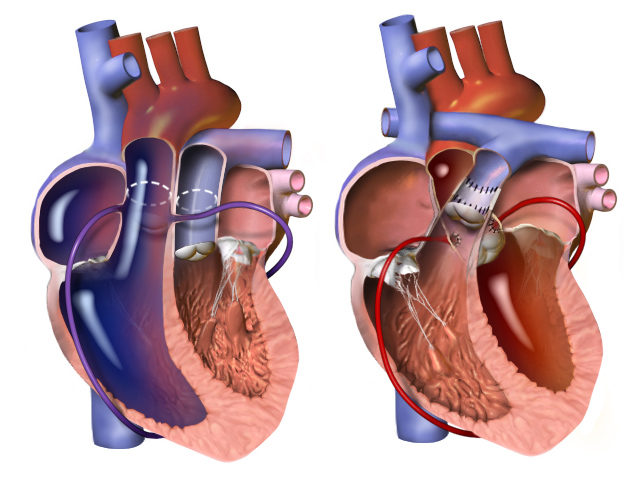
Surgical repair performed in 3 stages
1st stage performed immediately
Norwood procedure (3 parts)
Creation of neoaorta
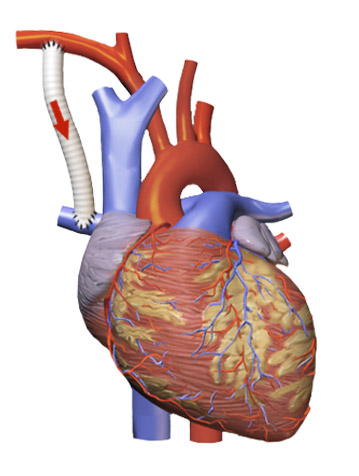
Blalock-Taussig shunt
Resection of atrial septum
Norwood Procedure
2nd stage performed at 3-6 months
Bidirectional Glenn procedure
Bidirectional Glenn Procedure
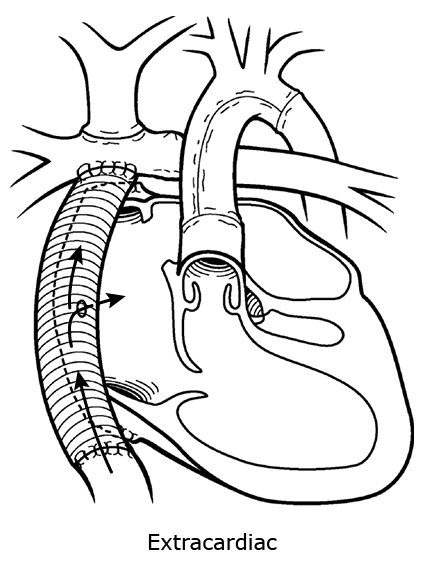
3rd stage performed at 2-3 years
Fontan procedure
Hybrid approach and heart transplant are emerging treatment options
PAINE Pearls to Remember
6 “Ts” of Congenital Cyanotic Heart Defects
Tetralogy of Fallot
Transposition of Great Vessels
Tricuspid Atresia
Truncus Arteriosus
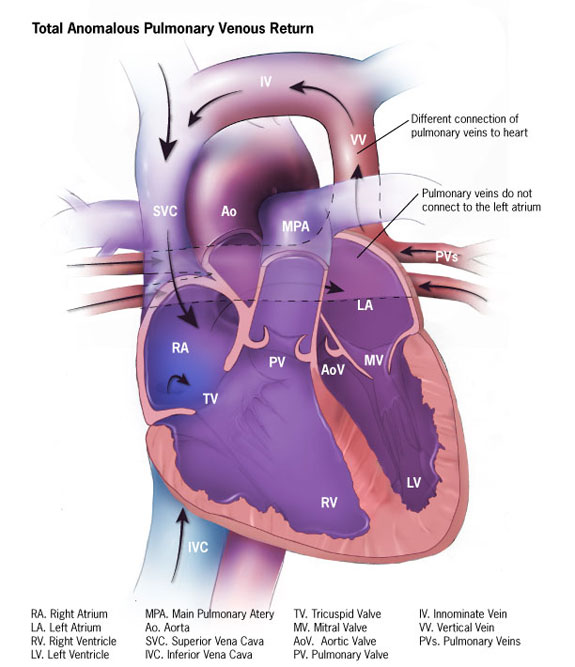
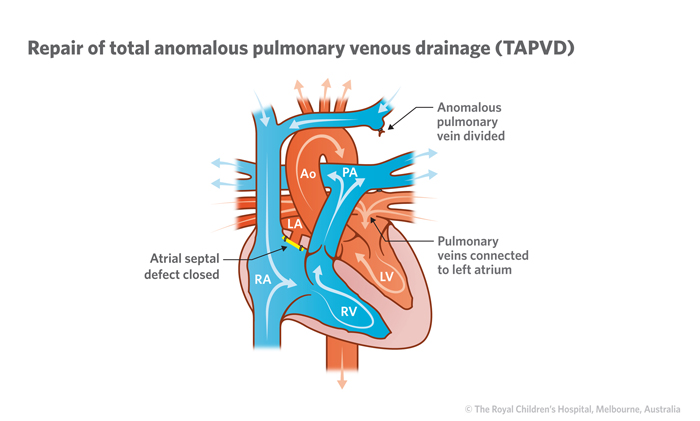
Total Anomalous Pulmonary Venous Connection
“Tiny” (Hypoplastic) Left Heart Syndrome
Numbers of Congenital Cyanotic Heart Defects
1 trunk (truncus arteriosus)
2 great vessels (transposition)
3 “tri” (tricuspid atresia)
4 “tetra” (Tetralogy of Fallot)
5 words (Total Anomalous Pulmonary Venous Connection)
VI – the left “I” is half as big as the right “V” (hypoplastic left heart)
Cottage Physician Reference
Nothing directly related to congenital heart defects, but I did find this quote interesting. It says:
“ The general rule as to tying the cord , with the exceptions above noticed, is, that it is the safest to delay the tying of it, until it has entirely ceased to pulsate”
The OB realm is still debating delayed cord clamping…It looks like everything in medicine always comes full circle
Which of the following genetic mutations is seen with chronic myelogenous leukemia?
Answer:
Translocation of chromosome 9 and 22. This new chromosome 22 is called “Philadelphia chromosome” after the city where the two hospitals that first identified the gene mutation in 1960 were both located.
The textbook definition of anemia is a reduction of the absolute number or mass of circulating red blood cells. This then causes a global reduction in the oxygen carrying capacity of the patient’s circulatory system. Clinically, we use hemoglobin and hematocrit as the surrogate markers and define anemia as 2 SD below the mean for gender:
Men
Hemoglobin < 13.5 g/dL
Hematocrit < 41%
Women
Hemoglobin < 12.0 g/dL
Hematocrit < 36%
Patel KV. Haematologica. 2008;93(9):1281-1283.
Special Populations
Athletes
May have a baseline anemia due to:
Dilution from increased plasma volume
Hemolytic breakdown from exercise
Exercise induced cytokines decreases RBC production
A normal H/H in a competitive athlete may suggest performance enhancing drugs
High altitudes
May have elevated hemoglobin concentration as baseline
Smokers
Baseline higher hemoglobin due to carboxyhemoglobin
General Causes of Anemia
There are two general approaches you can use to help identify the cause of anemia in adults.
The Kinetic Approach (the mechanisms responsible for the low hemoglobin)
3 independent mechanisms
Decreased RBC production
Lack of nutrients
Bone marrow failure
Decreased erythopoetic stimulation factors
Erythropoietin, T3, androgens
Inflammation
Increased RBC destruction
Hemolysis, hypersplenism
Blood loss
The Morphologic Approach (categories based on RBC size and reticulocyte response)
Any history of weight loss, night sweats, fever, anorexia?
Infection or malignancy
Past medical history for chronic illness
PUD, renal disease, autoimmune conditions, liver disease, past malignancies
Family history for hemoglobinopathies
Social history for alcohol use
Occupational exposures
Physical Exam Findings
Pallor
Palms, nail beds, face, conjunctiva
Jaundice
Hepatosplenomegaly
Lymphadenopathy
Petechiae, purpura, bruising
Bone tenderness
Laboratory Testing
Anemia is usually first diagnosed by CBC. Once you have a documented low H/H, then you need order follow-up studies to help differentiate the cause of the anemia. These include:
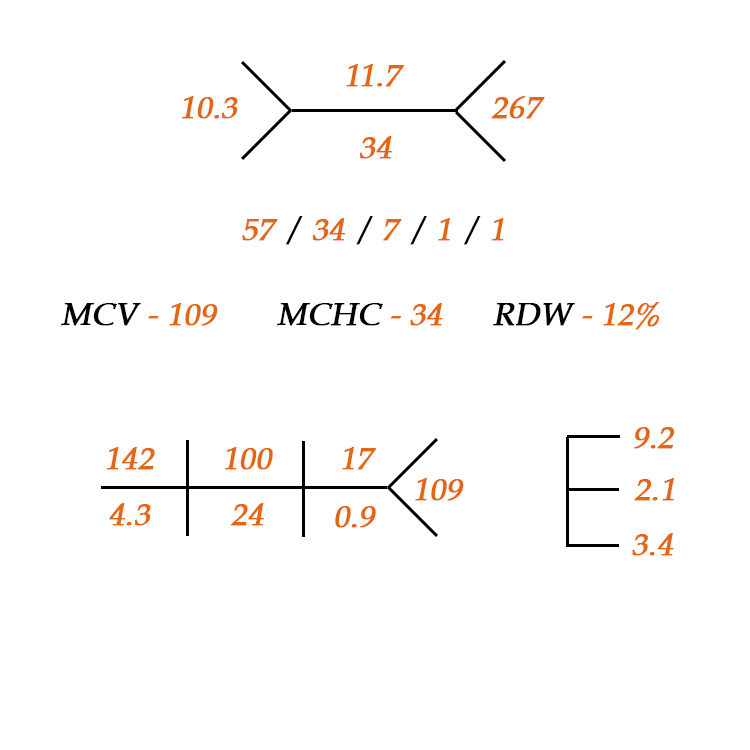
RBC indices
MCV, MCH, MCHC, RDW
Reticulocyte count and index
Peripheral smear
Helmet cells or schistocytes à microangiopathic hemolysis
Microspherocytes à autoimmune hemolysis
Tear drop RBC à myelofibrosis
Bite cells à oxidative hemolysis
Parasites à malaria, babeosis
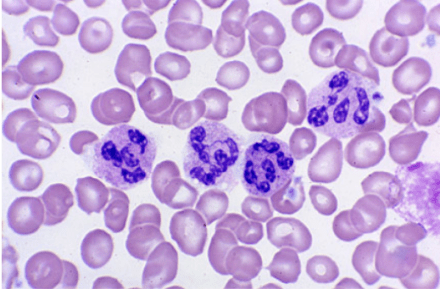
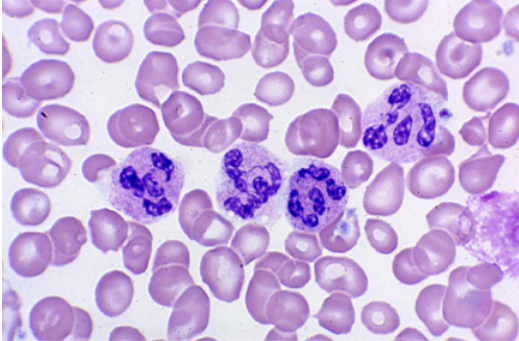
Hypersegmented neutrophils à Vitamin B12 or folate deficiency
Schrier SL, et al. Approach to adults with anemia. In: Up To Date. Waltham, MA (Accessed 03/23/2016)
The Cottage Physician Management
Something new I thought I would bring to the PAINE Podcast. As you all know, I am quite a fan of medicine and antiquity. Shortly after I married my wife, her grandfather past away from a progressive esophageal cancer. One of the things I was able to keep when helping clean out his house, was a copy of The Cottage Physician printed in 1893. It was basically a handbook on how to treat common ailments of the time. I will try to add excerpts from this book when appropriate so you can have a sense of how medicine was practiced in the late 19th century.
This patient has had a history of gastric cancer with a partial gastrectomy and now presents with a fatigue and gait disturbances. CBC reveals a macrocytic aneamia and peripheral smear shows multinucleated neutrophils. The gait disturbances are most likely due to the progressive peripheral neuropathy. This is most consistent with vitamin B12 deficiency. Intrinsic factor, which is secreted by the parietal cells of the stomach, is required for vitamin B12 absorption in the terminal ileum.
Work-Up for Vitamin B12 Deficiency
Serum B12 Level
< 300 pg/dL is diagnostic
Metobolites
Methylmalonic acid
< 70 nanomol/L is diagnostic
Homocysteine
< 5 micromol/L is diagnostic
Possible additional testing in the setting of macrocytic anemia:
If pernicious anemia is suspected:
Anti-intrinsic factor antibodies
If folate deficiency is suspected:
Serum folate level
< 2 ng/mL is diagnostic
RBC folate level (reserved for indeterminate serum levels)
< 280 ng/mL is diagnostic
Treatment for B12 Deficiency
Intramuscular
1mg daily x 7 days, then 1mg weekly for 4 weeks, then 1mg monthly
Oral
1000-2000mg daily
References
Antony AC. Megaloblastic anemias. In: Hematology: Basic principles and practice, 4th ed, Hoffman R, Benz EJ, Shattil SJ, et al. (Eds), Churchill Livingstone, New York 2005. p.519.
62-year-old male presents to primary provider’s office with a six-month history of fatigue and gait disturbance. He denies recent falls, weakness, pain, paralysis, or dizziness.
Medications
Lisinopril 10mg daily
Metformin 1000mg BID
Men’s multivitamin
Fish oil
Past Medical History
Diabetes Mellitus II
Hypertension
Gastric cancer
Past Surgical History
Cholecystectomy – 1997
Partial gastrectomy – 2004
Vitals
BP-128/79, HR-81, RR-14, O2-100%, Temp-98.9o
Physical Exam
General – WN/WD, NAD
Skin – scattered senile purpura, no petechiae
CV – RRR without M/G/R
Pulmonary – CTA bilaterally without adventitial breath sounds
Neurologic – A&Ox3, 5/5 strength throughout bilaterally, DTR 2+ and equal, FROM, vibratory sensation decreased in bilateral lower extremities



























{kind=link}