A 5yo boy is brought to you clinic by his parents for reporting that his legs hurt “when he plays too much”. His parents corroborate this saying that when he is climbing on the playground for too long he complains that his legs hurt and he needs to stop and rest for awhile. Vaccinations are UTD and he has had a relatively healthy childhood without significant illnesses. He has no significant past medical history and mother reports that she was 38 weeks when he was born via NSVD without any complications. Cardiac auscultation reveals a normal S1 and S2 without murmurs, gallops, or rubs.
What would you expect to find on physical examination?
What other physical assessment can you perform at the bedside to help with the diagnosis?
What findings on diagnostics would also help with the diagnosis?
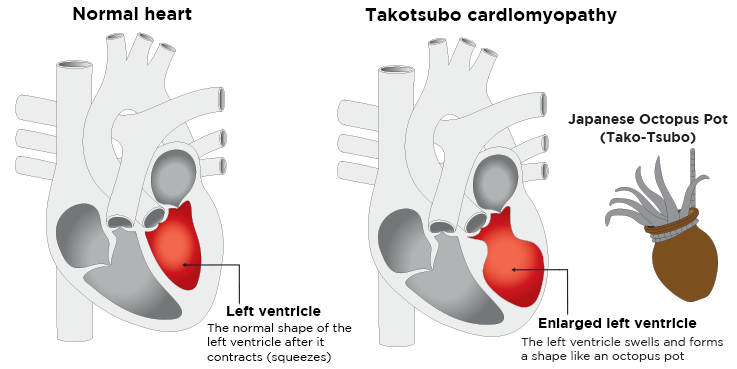
Clinical Significance – this syndrome is characterized by transient regional systolic dysfunction of the left ventricle, that mimics a myocardial infarction, but with an absence of angiographic evidence of coronary artery involvement.
History – Named after Japanese word for “octopus trap” as the left ventricle takes the shape of this unique hunting vessel. This condition was first studied in Japan by Hikaru Sato in 1991, but it was not “introduced” to the western medical world until 1997.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
73yo man, with a history of hypertension and coronary disease, is brought into the emergency room after a witnessed syncopal episode at home. He reported some mild exertional chest pain over the past few days, but states that it improved with rest. Vital signs are BP-180/98, HR-74, RR-12, and O2-100%. He is currently in no distress and not diaphoretic. Physical examination revealed a systolic murmur over the 2nd right intercostal space. A CT was ordered to rule-out PTE in the setting of chest pain and syncope and is below, along with the murmur.
What is the diagnosis?
How would you describe this murmur?
Where would you expect this murmur to radiate?
What is the classic triad associated with this condition?
Answer
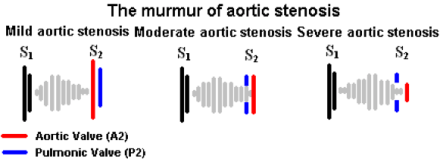
Aortic Stenosis due to a calcified aortic valve
High-pitched, crescendo-decrescendo (diamond shaped), midsystolic, ejection murmur with a soft S2
AS murmurs transmit well and equally to the carotid arteries
The classic triad of AS is exertional angina, exertional dyspnea, and dizziness/syncope
Definition – lines seen on chest radiography due to interstitial edema
Clinical Significance – Kerley lines are thin pulmonary opacities caused by fluid or cellular infiltration into the interstitial of the lungs. There are three distinct types that are seen:
Kerley A lines – linear opacities extending from the periphery to the hilum caused by distention of anastomotic channels between peripheral and central lymphatics
Kerley B lines – short horizontal lines situated perpendicularly to the pleural surface at the lung base and represent edema of the interlobar septa
Kerley C lines – reticular opacities at the lung base representing Kerley B lines en face
White Arrows (A lines); White Arrowheads (B lines); Black Arrowheads (C lines)
History – Named after Sir Peter James Kerley (1900-1979), who was an Irish radiologist and received his medical doctorate from Cambridge University in 1932. He went on to study in Vienna, which was the center of the new and blossoming specialty of heart and lung radiography. He assisted to editing “A Textbook of X-ray Diagnosis” in 1939, which was a major radiology textbook at the time, and later became director of radiology at Westminster Hospital in 1939. He first described his eponymonic findings in an article entitled “Radiology in heart disease” in 1933, and further elaborated on them in the second volume of his textbooks in 1951. During this year, he was also a key figure in the diagnosing of King George VI’s lung cancer due to his review of the King’s radiographs. He received several Royal awards for mass radiological screening for tuberculosis and his diagnosis of King George VI cancer, leading up to his Knight Commander of the Royal Victorian Order by Queen Elizabeth in 1972.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
73yo man, with a history of hypertension and coronary disease, is brought into the emergency room after a witnessed syncopal episode at home. He reported some mild exertional chest pain over the past few days, but states that it improved with rest. Vital signs are BP-180/98, HR-74, RR-12, and O2-100%. He is currently in no distress and not diaphoretic. Physical examination revealed a systolic murmur over the 2nd right intercostal space. A CT was ordered to rule-out PTE in the setting of chest pain and syncope and is below, along with the murmur.
What is the diagnosis?
How would you describe this murmur?
Where would you expect this murmur to radiate?
What is the classic triad associated with this condition?
Definition – intravenous catheter that is maneuvered through the right side of the heart into the pulmonary artery.
Clinical Significance – This catheter can directly measure several important hemodynamic variables in critical illness:
right atrial pressures
right ventricular pressures
pulmonary artery pressures
left atrial filling pressures (wedge pressure)
cardiac output/cardiac index
systemic vascular resistance
pulmonary vascular resistance
It is “floated” through the right side of the heart using the flow of the blood to carry it into the pulmonary artery. This migration has a very characteristic pressure pattern to know where the catheter is in the vascular system.
History – Named after two physicians from Cedars-Sinai Medical Center, Jeremy Swan (1922-2005), an Irish American cardiologist, and William Ganz (1919-2009), a Slovak American cardiologist. Dr. Swan received his medical doctorate from Castleknock College and went on to become faculty at the Mayo Clinic before joining the faculty at Cedars-Sinai Hospital in Los Angeles. Dr. Ganz attended Charles University School of Medicine in Prague in 1938, but was closed in 1940 after the Nazi occupation of Czechoslovakia. Being jewish, he was then sent to a Hungarian Nazi labor camp and was actually scheduled to be sent to Auschwitz in 19944 before his escape. After hiding and waiting out the war, Dr. Ganz returned and graduated from Charles University in 1947 at the top of his class. He practiced in communist Czechslovakia until 1966 when he secretly defected to the US with his wife and sons. His first and only position as a physician in the US was at Cedars-Sinai Hospital, where he met Dr. Swan who got the idea of the catheter from watching the wind play with the sails of boats in the marina. Dr. Ganz had already published research on the use of thermodilution as a way to measure cardiac output and in 1970, they published their landmark article in the NEJM. It should be noted that German surgeon Werner Forssmann first demonstrated the safety of this type of catheter, by doing it on himself in 1929.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Swan HJ, Ganz W, Forrester J, Marcus H, Diamond G, Chonette D. Catheterization of the heart in man with use of a flow-directed balloon-tipped catheter. The New England journal of medicine. 1970; 283(9):447-51. [pubmed]
FRONEK A, GANZ V. [Local thermodilution method of measuring minute volume and circulation rate in the peripheral vessels]. Ceskoslovenska fysiologie. 1959; 8(3):189. [pubmed]
W. Forssmann. Die Sondierung des Rechten Herzens. Klinische Wochenschrift, Berlin, 1929, 8: 2085.
Other Known Aliases – J-wave, camel-hump, hypothermic hump
Definition – positive deflection occurring at the junction between the QRS complex and ST segment, commonly referred to as the J point
Clinical Significance – Osborn waves are classically seen in hypothermia with a core body temperature < 32°C (90°F), but also can be present in severe hypercalcemia, traumatic brain injury, and pericarditis. It is usually most prominent in the precordial leads.
NEJM. 2015
History – Named after John J. Osborn (1917-2014), who was an American intensivist, and received his medical doctorate from Johns Hopkins University in 1943. He completed a nine-month residency in pediatrics before serving as an Army medical officer in World War II in the Pacific Theatre. He first published his preliminary animal research on hypothermia in 1943 before his military service, and picked it back up after returning stateside. He practiced from New York University to Stanford University and was a founding member of the Society of Critical Care Medicine. His research fostered the initial golden age of intensive care medicine and he worked on heart-lung machine designs, as well as hemodynamic monitoring devices. His eponymous paper was published in 1953 entitled “Experimental hypothermia; respiratory and blood pH changes in relation to cardiac function”
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
OSBORN JJ. Experimental hypothermia; respiratory and blood pH changes in relation to cardiac function. The American journal of physiology. 1953; 175(3):389-98. [pubmed]
Partin C. Profiles in Cardiology: John J Osborn. Clin Cardiol. 1998;21;66-68 [link]
Other Known Aliases – Fallot’s tetrad, Fallot’s syndrome, Steno-Fallot tetralogy
Definition – Congenital cyanotic heart disease due to ventriculo-septal defect, pulmonary stenosis, right ventricular hypertrophy, and overiding aorta.
History – Named after Etienne-Louis Arthur Fallot (1850-1911), who was a French physician and received his medical doctorate from the University of Marseille in 1867. He described this tetrad in 1888 in an article entitled “Contribution à l’anatomie pathologique de la maladie bleue (cyanose cardiaque)” using previous observations from the work of Dutch anatomist Neils Stenson (1638-1686). Unfortunately, Fallot’s work garnered little contemporary acclaim and it wasn’t until Dr. Paul Dudley White (of WPW fame) translated and republished Fallot’s work in his landmark textbook “Heart Disease” in 1931.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Definition – systolic precordial crunching sound that occurs with each contraction of the heart that is best heard over precordium in the left lateral decubitus position
Clinical Significance – this is one of the classic physical examination findings in pneumomediastinum or pneumopericardium as a result of trauma to the bronchial tree, bleb rupture, or esophageal rupture.
History – Named after Louis Virgil Hamman (1877-1946), an American internists who received his medical doctorate from Johns Hopkins University in 1902. He was considered one of the great physicians of his era and made significant progress in the management of tuberculosis as the head of the Phipps Tuberculosis Clinic at Johns Hopkins. He described this finding in patients with spontaneous mediastinal emphysema in two separate articles, first in 1939 in The Bulletin of Hopkins Hospital, and then in JAMA in 1945.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Angiotensin converting enzyme (ACE) inhibitors are one of the more common medications used in the management of primary hypertension. What are some potential adverse reactions from and contraindications to using ACE inhibitors?
Answer
Cough
10% of patient experience a dry, hacking cough
Hypotension
2% of patients can experience hypotension, weakness, or dizziness from excessive reduction in blood pressure
Reduction in GFR
2% of patients can see a doubling in creatinine due to decreased intrarenal perfusion as a result of increased efferent arteriole resistance
Hyperkalemia
3% of patients can have a potassium > 5.5 mEq/L by reducing urinary potassium excretion
Angioedema
0.3% of patients can experience potentially life-threatening angioedema
Pregnancy
Associated with cardiac malformations in the first trimester and renal malformations in the second/third trimesters
References
Israili ZH, Hall WD. Cough and angioneurotic edema associated with angiotensin-converting enzyme inhibitor therapy. A review of the literature and pathophysiology. Annals of internal medicine. 1992; 117(3):234-42. [pubmed]
Bangalore S, Kumar S, Messerli FH. Angiotensin-converting enzyme inhibitor associated cough: deceptive information from the Physicians’ Desk Reference. The American journal of medicine. 2010; 123(11):1016-30. [pubmed]
ONTARGET Investigators – Yusuf S, Teo KK, et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. The New England journal of medicine. 2008; 358(15):1547-59. [pubmed]