Beck’s Triad
Other Known Aliases – none
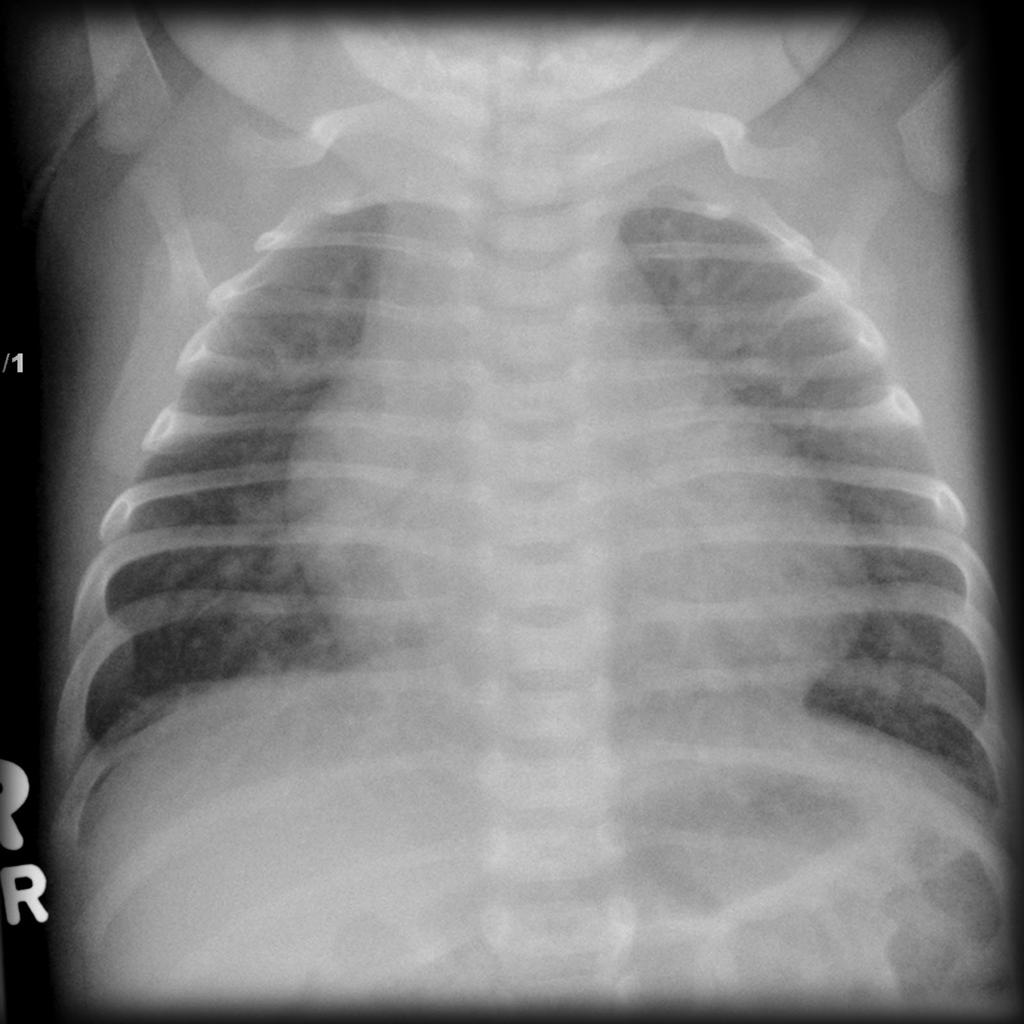
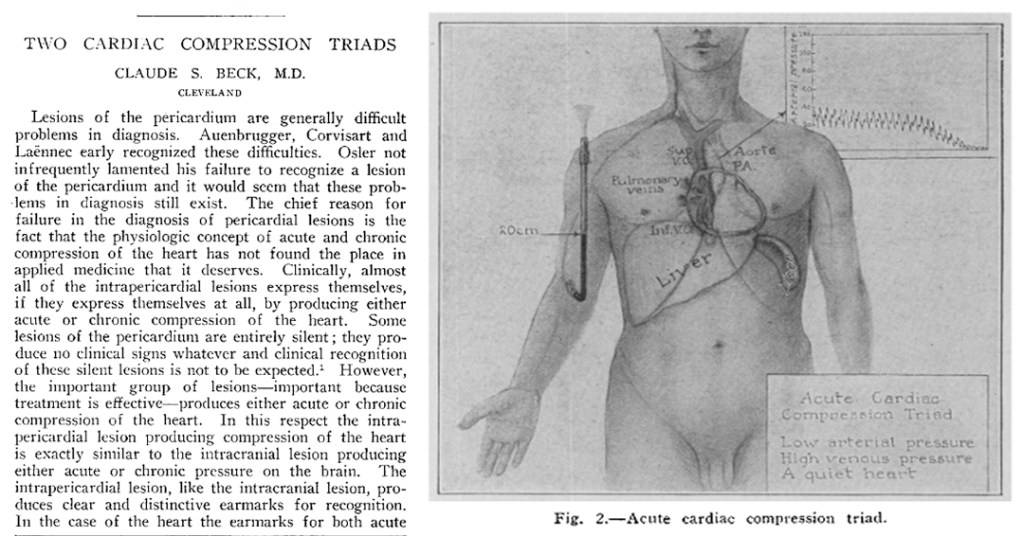
Definition – classic physical examination findings associated with critical cardiac tamponade
Clinical Significance – although not seen in every patient with cardiac tamponade, it is a common question on boards and certification examinations. These include: 1) hypotension, 2) JVD, and 3) muffled/distant heart sounds.

History – Named after Claude Schaeffer Beck (1894-1971), an American cardiac surgeon who recieved his medical doctorate from Harvard University in 1921. He would attend surgical residency at Case Western University, where he would spend his entire career. He developed a novel re-circulation technique for cardiac ischemia called the Beck Procedure, where pectoral muscle was implanted in the pericardium, and later placing a vein graft between the aorta to the coronary sinus. He also pioneered the first successful use of a defibrillator in 1947 to restore ROSC in a 14yo patient he was operating on for a congenital heart defect. His eponymous triad was first described in 1935 in an article entitled “Two cardiac compression triads” in the Journal of the American Medical Association.

References
- Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
- Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
- Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
- Whonamedit – dictionary of medical eponyms. http://www.whonamedit.com
- Up To Date. www.uptodate.com
- Beck CS. Two Cardiac Compression Triads. JAMA. 1935;104(9):714-716. [link]
- Theruvath P, Ikonomidis JS. Historical perspectives of The American Association for Thoracic Surgery: Claude S. Beck (1894-1971). JTCVS. 2015;149(3):655-660. [link]