I have a multi-step question for you all today and they involve the below images:


- What are these two conditions called?
- Which is associated with other genetic conditions?
- Which has better associated outcomes?


I have a multi-step question for you all today and they involve the below images:

Other Known Aliases – progressive hepatolenticular degeneration
Definition – Autosomal recessive condition that causes impaired copper metabolism leading to intoxication due to a mutation in the chromosome 13q14 resulting in faulty ATP7B protein production.

Clinical Significance – A rare, but devastating, disease if not identified early in its course. It can effect multiple systems including:

History – Named after Samuel Alexander Kinnier Wilson (1878-1937), who was an American-born, British neurologist. He received his medical degree from the University of Edinburgh Medical School in 1902 and studied neurology with Joseph Babinsky at the Salpétriére Hospital in Paris before relocating back to London for the duration of his medical career. He is also credited with introducing the neuropsychiatric term “extrapyramidal” into the medical lexicon. He described his eponymous disease in his 1912 medical dissertation where it gained its notoriety, but was first recorded in 1854 by Friedrich Theodor von Freichs.

References
Other Known Aliases – Fallot’s tetrad, Fallot’s syndrome, Steno-Fallot tetralogy
Definition – Congenital cyanotic heart disease due to ventriculo-septal defect, pulmonary stenosis, right ventricular hypertrophy, and overiding aorta.
Clinical Significance – This is one of the six congenital cyanotic heart defects and is also the most common. Read/listen to an amazing review of “Congenital Cyanotic Heart Diseases” here.
History – The classic description of the tetrad was actually first described in 1672 by the Danish physician and anatomist, Neils Stenson (1638-1686). The namesake of this condition is Etienne-Louis Arthur Fallot (1850-1911), who was a French physician. He described the tetrad in 1888 using previous observations and building from the work of Stenson, but garned little contemporary appraise. It wasn’t until 1931 when Fallot’s work was rekindled and translated by Dr. Paul Dudley White.
References
What are the six (6) classic infectious exanthems of childhood and what organism causes each?
The chart below lists the classic exanthems of childhood, the organism that causes, and the “number” disease that were given to them in 1905.

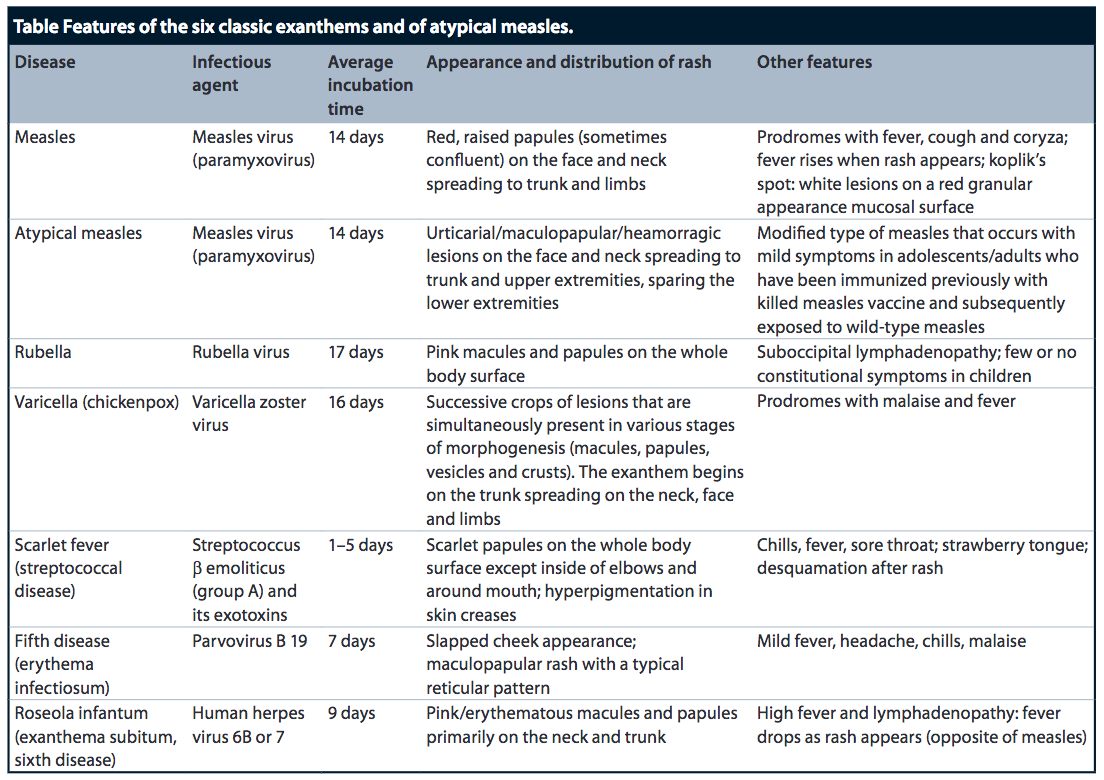
It should be noted that Duke’s Disease (fourth disease) is not widely accepted as a true infectious exathem.
References
Other Known Aliases – Reye’s sequence, Reye-Morgan-Baral syndrome, Reye-Johnson syndrome
Definition – Rare disease of acquired encephalopathy and fatty liver filtration in children under 15 years of age
Clinical Significance – Classically, this condition follows a viral upper respiratory illness (influenza B, varicella) in children who were given aspirin for fever therapy. Symptoms include vomiting, confusion, AMS, seizures, and LOC. Children under 5 years of age frequently have hyperglycemia as well. Mortality is as high as 40% and many that survive are left with significant brain damage.
History – First described in 1929 by Dr. W.R. Brain, D. Hunter, and H.M. Turnbull, but not established as clinical diagnosis until published in The Lancet in 1963 by Dr. Ralph Douglass K. Reye, Dr. Graeme Morgan, and Dr. James Baral,. Later that same year (1963), an outbreak of this condition occurred in North Carolina and was published by Dr. George Johnson.
References
Epidemiology
Acute otitis media (AOM) is the most frequent diagnosis in ill children and the most common reason for antibiotic prescriptions (which is debatable). Children < 2 years-old are at the highest risk, with nearly 80% of children in the US having at least one documented episode of AOM annually. Incidence has been declining in the US since 2009 with the widespread use of the 13-valent pneumococcal vaccine.
Risk Factors
Pathogenesis
The development of AOM follows a predictable series of events:

Microbiology
Signs and Symptoms
Physical Exam
The diagnosis of AOM requires:

Acute Management
Analgesia
Antibiotics vs Observation

Antimicrobial Therapy
Oral therapy is preferred if perforation is present.
If a child has acute onset of otorrhea with known tympanostomy tubes in place:
Treatment Failure
This is defined as lack of improvement by 72 hours in patients treated with antibiotics.
Recurrent AOM
This defined as development of AOM after successful treatment and treatment depends on the timeframe:
Tympanostomy Tube Placement Indications
References
We are going to stay on the pediatric infectious disease kick…….

Definition – Upward pressure applied to the angle of mandible produces pain with parotitis, but not with adenitis
Clinical Significance – This particular sign could be positive before any significant parotid gland swelling occurred and would aid in the early detection and diagnosis of mumps.
History – First described by a Lieutenant Hatchcock in 1918. Honestly, I can’t find much on this Lieutenant Hatchcock……
References
What are the organisms that you must think of in a sick neonate that can be transmitted in utero from mother to fetus?
There are 10 organisms that are most commonly transmitted in utero from mother to fetus and are remembered by the mnemonic: TORCHESCLAP
References
Definition – Congenital syndrome with three main features:
Clinical Significance – Occurs almost exclusively in females and clinical findings can include:
History – Named after Dr. Jean Fraçois Marie Aicardi, who is a French pediatrician, and first published and described this disorder in two girls in 1965.
References
