LISTEN TO THE PODCAST HERE
Epidemiology
Dyspnea is one of the more common complaints that will bring a patient to the ED for evaluation. The most recent data from the CDC shows more than 3.7 million visits to the ED in the United States for shortness of breath alone and more than 11 million for dyspnea-related complaints (cough, chest pain, etc.).

Pathophysiology
There are 3 global processes that have to function in series to prevent a patient from becoming short of breath:
- Ventilation
- Airflow through the tracheobronchial tree to the terminal alveoli
- Ventilation without perfusion = Dead space
- Anatomic = trachea, main bronchi
- Physiologic = terminal alveoli
- Perfusion
- Blood flow through the pulmonary arteries to the terminal capillaries
- Perfusion without ventilation = Intrapulmonary shunt
- Anatomic = right-to-left shunt
- Physiologic = terminal alveoli
- Gas Exchange
- Capillary-alveoli interface to exchange oxygen and carbon dioxide
- Determined by arterial-alveoli gradient
- Capillary-alveoli interface to exchange oxygen and carbon dioxide

5 Main Causes of Hypoxemia
- V/Q Mismatch (most common)
- PNA, PTE, pulmonary edema, asthma, COPD
- Hypoventilation
- Drug overdose, neuromuscular disease (GBS, ALS, MG)
- Right-to-Left Shunt
- Intracardiac
- PFO, ASD, VSD
- Vascular
- PTE, AVM
- Alveolar
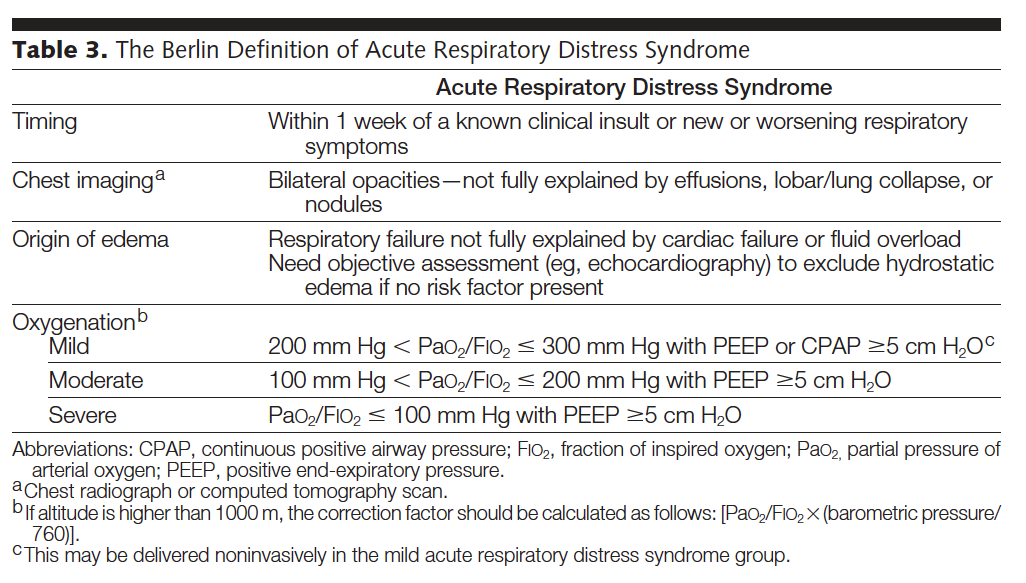
- PNA, atelectasis, pulmonary edema, ARDS
- Intracardiac
- Low Inspired Oxygen
- Altitude, fire,
- Diffusion Abnormality
- COPD, interstitial lung disease

Bedside Evaluation
Vitals
- Blood Pressure
- Often hypertensive due to stress
- Can also be the precipitating factor
- Heart Rate
- Often tachycardic due to stress and system trying to increase cardiac output for oxygen demand
- If bradycardic à think overdose
- Respiratory Rate
- Will be tachypnic
- > 40 bpm is ominous and respiratory failure could be imminent
- if bradypnic à think overdose
- Will be tachypnic
- Temperature
- If febrile, then infectious causes go up on differential
- Pulse oximetry
- Common practice is to give all dyspneic patients oxygen
- Lots of research on oxygen in ACS
- Common practice is to give all dyspneic patients oxygen
History
- Onset
- Severity
- Events leading up to this episode
- Triggers, compliance with medications
- Allergies
- Past History
- Medical problems, previous episodes
- Chest pain
- Trauma
- Fever
- Hemoptysis
- Cough
- Tobacco history
- Medications
Physical Exam
Rapid examination should be performed (often while getting the history) to evaluate for impending respiratory collapse:
- Altered mental status
- Lethargy to combative
- Fatigue of breathing
- Audible stridor
- Cyanosis
- Tripod position
- Retractions or accessory muscle use
- Fragmented speech
- Inability to lie supine
- Diaphoresis
Any of the above findings should raise your threshold to intubate.
Once these have been evaluated and ruled-out, you can begin a focused physical exam to address the causes of acute dyspnea:
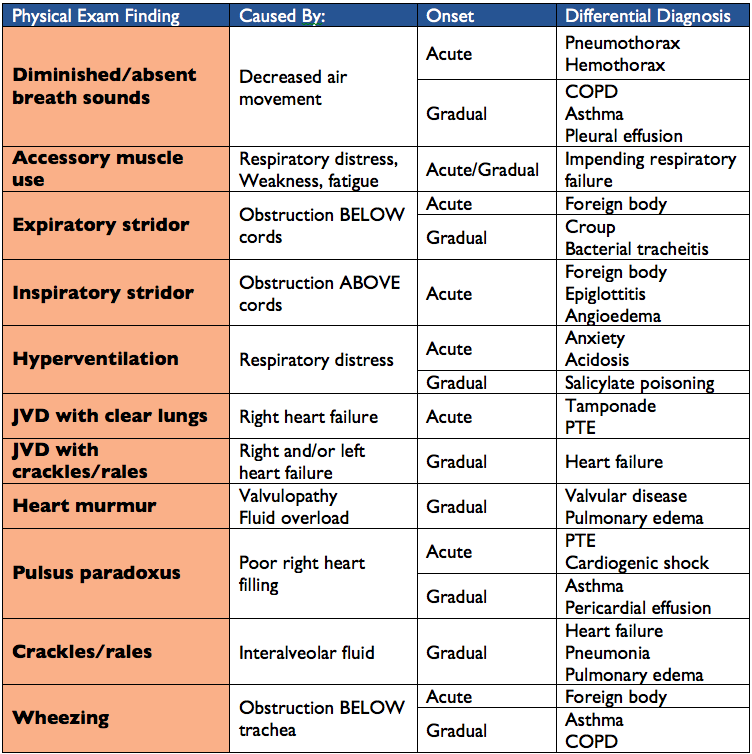
- Pulmonary
- Breath sounds
- Wheezing, diminished, equal, crackles, rales
- Breath sounds
- Cardiovascular
- Rhythm
- Tachycardia, irregular
- Murmurs
- S3/S4
- Distant/muffled heart sounds
- Edema/JVD
- Rhythm
- Skin
- Diaphoresis
- Capillary refill
- Urticaria
Work-Up
- Chest Radiograph
- EKG
- Ultrasound
- Labs
- D-Dimer
- Brain Naturetic Peptide (BNP)
- If < 100 pg/mL à > 90% NPV for CHF
- If > 500 pg/L à > 90% PPV for CHF
- ABG
- Needed to calculate the A-a gradient
Differential Diagnosis
- Upper Airway
- Angioedema
- Foreign body
- Anaphylaxis
- Infections
- Trauma
- Pulmonary
- PTE
- COPD
- Asthma
- Edema
- PTX
- Pneumonia
- Trauma
- Hemorrhage
- Effusion
- Cardiac
- Acute decompensated heart failure
- ACS
- Cardiomyopathy
- Dysrhythmias
- Valvulopathies
- Effusion/tamponade
- Neurologic
- Neuromuscular
- GBS, MG, ALS
- Neuromuscular
- Metabolic/Toxic
- Overdose
- Carbon monoxide poisoning
- Acute chest syndrome in sickle cell disease
- Miscellaneous
- Anxiety
- Ascites
Management
Three main primary goals for the emergent management of acute dyspnea:
- Optimize arterial oxygenation
- Provide supplemental oxygen
- Continuous cardiac and pulse oximetry monitoring
- Determine need for emergent airway management
- Bring airway supplies to the bedside
- Non-invasive ventilation is an option
- Include difficult airway adjuncts as well
- Bring airway supplies to the bedside
- Determine most likely cause and initiate treatment
- Start work-up (as outlined above)
- Don’t let a definitive diagnosis preclude starting treatment
References
- National Hospital Ambulatory Medical Care Survey: 2011 Emergency Department Summary. http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2011_ed_web_tables.pdf. Accessed on November 15th,2016.
- Petersson J, Glenny RW. Gas exchange and ventilation-perfusion relationships in the lung. The European Respiratory Journal. 2014;44(4):1023-41. [pubmed]
- Simon PM, Schwartzstein RM, Weiss JW, Fencl V, Teghtsoonian M, Weinberger SE. Distinguishable types of dyspnea in patients with shortness of breath. The American Review of Respiratory Disease. 1990;142(5):1009-14. [pubmed]
- Schabowski S, Lin C. Dyspnea. In: Sherman SC, Weber JM, Schindlbeck MA, Rahul G. P. eds. Clinical Emergency Medicine, 1e. New York, NY: McGraw-Hill; 2014. http://accessemergencymedicine.mhmedical.com/content.aspx?bookid=991&Sectionid=55139128 . Accessed November 16, 2016.
- Fertel BS. Respiratory Distress. In: Cydulka RK, Cline DM, Ma O, Fitch MT, Joing S, Wang VJ. eds. Tintinalli’s Emergency Medicine Manual, 8e. New York, NY: McGraw-Hill; 2016. http://accessemergencymedicine.mhmedical.com/content.aspx?bookid=1759&Sectionid=128948449 . Accessed November 16, 2016.
- Schneider HG, Lam L, Lokuge A. B-type natriuretic peptide testing, clinical outcomes, and health services use in emergency department patients with dyspnea: a randomized trial. Annals of Internal Medicine. 2099;150(6):365-71. [pubmed]
- Ahmed A, Graber MA. Evaluation of the adult with dyspnea in the emergency department. In: UpToDate, edited by Hockberger RS, Grayzel J. UpToDate, Waltham, MA. 2016. https://www.uptodate.com/contents/evaluation-of-the-adult-with-dyspnea-in-the-emergency-department?source=see_link#H29. Accessed November 16, 2016.