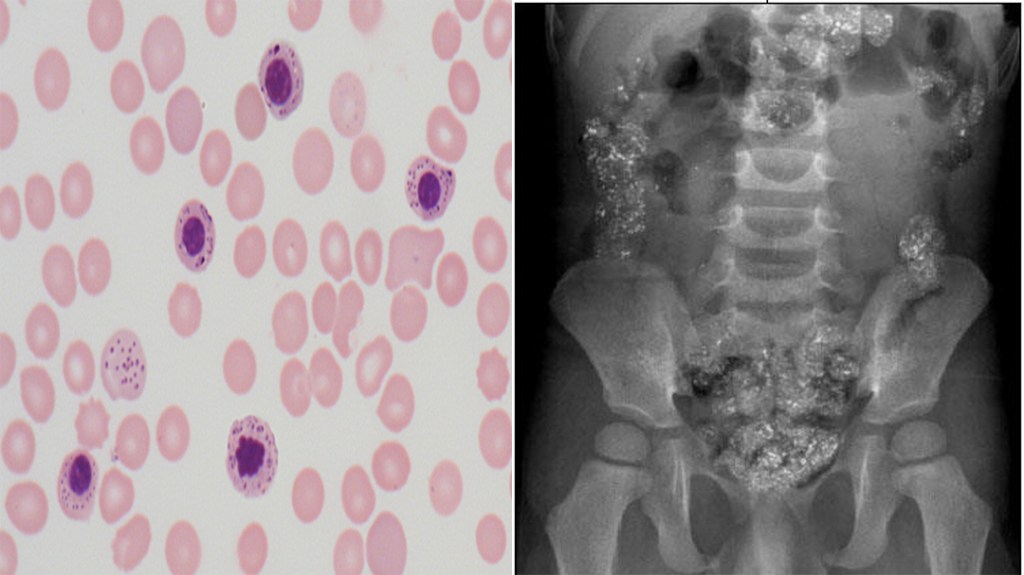
A 2yr old child is brought to the ED for altered mental status, vomiting, and leathargy. The parents states that this has been occurring since they moved into their grandmother’s home 2 months ago. Vitals signs are within normal limits and CBC reveals a hemoglobin – 10.1 mg/dL, mean corpuscular volume (MCV) – 71 fL/cell, and mean cell hemoglobin concentration (MCHC) – 29.1 g/dL. Peripheral smear and abdominal xray are below.
What is the most likely diagnosis?
What is the next diagnostic step?
What is the first step in the management of this patient?
Definition – shelf-like tumor of the anterior rectal wall (Pouch of Douglas) felt on rectal examination
Clinical Significance – palpation of this “shelf” indicates implantation metastases from primary abdominal malignancy
History – Names after George Blumer (1872-1962), who was an English-American physician and recieved his medical doctorate from the Cooper Medical College (forerunner of Stanford’s medical school) in 1891. He would go onto to train under William Halstead and William Osler at Johns Hopkins Hospital at house officer. In 1906, he became professor of medicine at Yale culminating in Dean of the medical school from 1910-1920. It was during this tenure (1909) when he described his eponymous finding in an article entitled “Rectal shelf: neglected rectal sign of value in diagnosis of obscure malignant and inflammatory disease within the abdomen”.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Most common type of acute leukemia and the second most common type in adults
32% of all adult leukemia cases
Only 1% of all adult cancers deaths in the US
Around 12,000 deaths per year in US
3-5 cases per 100,000 population
Around 20,000 patients per year in the US get diagnosed
2% annual increase in cases from 2007-2016
Mean age of diagnosis is 65 years and increases with age
Pathophysiology
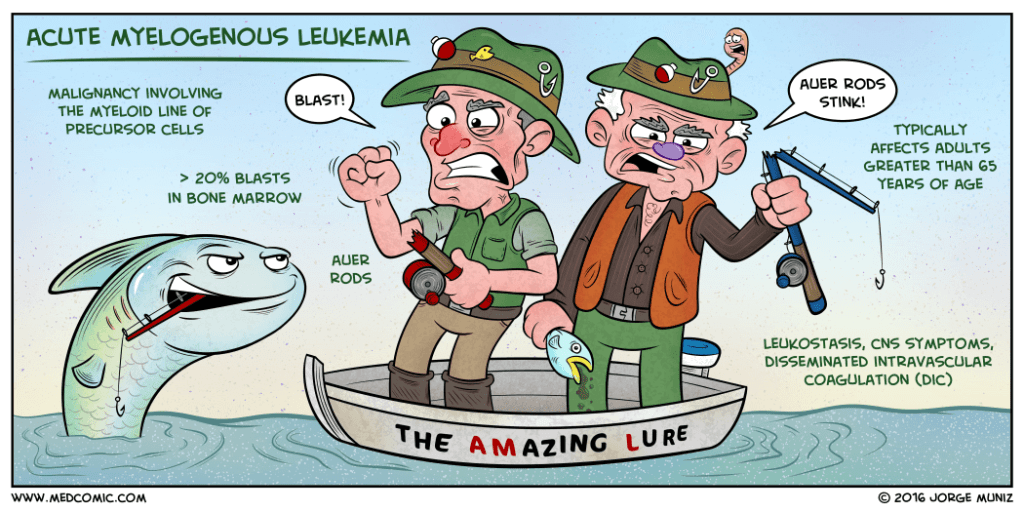
Malignancy of myeloid precursor cells
Multipotential hematopoietic stem cell –> common myeloid progenitor –> myeloblast
2 main models
Occurs at one of several developmental stages
Occurs within the primitive multipotent cells
Two-hit hypothesis of leukemogenesis
Class I mutation
Confers a proliferative advantage
Class II mutation
Impairs hematopoietic differentiation
Mechanisms of Genetic Damage
Chemotherapy
3-5 years after alkylating agent-induced damage
Ionizing radiation
Induces double strand breaks
Typically > 20 Gy (grays)
Chemical exposure
Benzene is classically associated with AML
Infections
Human T-lymphocyte virus type I (HTLV-1
Signs and Symptoms
Constitutional
Fatigue, weakness, dyspnea
Fever
Skin (13% of patients)
Easy bruisability, ecchymoses
Pallor
HEENT
Gingival bleeding, oral candidiasis
Papilledema, retinal infiltrates
Lymphadenopathy
Abdomen (10% of patients)
Organomegaly
Spleen and liver
Musculoskeletal (4% of patients)
Polyarthritis and arthralgias
Bone pain
Emergency Presentations
Pancytopenia
Tumor lysis syndrome
Hyperkalemia, hyperphosphatemia, hyperuricemia, AKI
Bleeding
New onset CNS symptoms
Diagnostic Studies
CBC
Leukocytosis or leukopenia
20% of patients have > 100,000 cells/microL
25-40% of patients have < 5,000 cells/microL
Thrombocytopenia
75% of patients have < 100,000 cells/microL
25% of patient have < 25,000 cells/microL
Peripheral Blood
95% of patients will have circulating myeloblasts
Immature cells with large, prominent nuclei and variable amount of pale blue cytoplasms
May have Auer rods present
Myeloperoxidase reaction
Simple means of determining if the blasts are myeloid
Flow Cytometry
Can assist in detecting circulating myeloblasts
Bone Marrow Biopsy
This is the key component in the diagnosis of AML
It gives a general overview of the degree of involvement, allows for cell differential count to determine the percentage of blasts in the marrow, and provides a detailed cytologic evaluation of the blasts
Cell Origin
Identifies if myeloid, monocytic, erythroid, or megakaryocytic
Differentiates the blasts of lymphoid lineage
Infiltration
Diagnosis of AML is > 20% blasts of the total cellularity
HLA Typing in patients who are potential candidates for bone marrow transplantation
Diagnosis
Requires both of the following criteria:
Documentation of bone marrow infiltration
> 20% blasts in bone morrow
Myeloid origin
Presence of Auer rods, (+) myeloperoxidase reaction, or presence of myeloid markers on immunophenotyping
Treatment
Goals
Complete remission (<5% blasts)
Appropriate goal for most AML patients
Pretreatment evaluation
Comorbid conditions
Heart disease, renal insufficiency, liver disease
Physical function and performance status
ECOG Scale most commonly used
Two distinct treatment phases
Induction
Combination therapy (7 and 3 regimen)
Cytarabine
Interferes with DNA synthesis
7 day continuous infusion
Anthracycline
Daunorubicin, idarubicin
Inhibition of topoisomerase II
Leads to DNA breaks
Day 1, 2, and 3
Bone marrow biopsy 7-10 days after induction to re-assess
Postremission management
Continuing chemotherapy
Hematopoietic cell transplant
Prognosis
Overall 5-year survival is 15%
Decreases with age
53% 5-year survival in 15-24yo to 13% in 70-79yo
Genetic subtypes
Karyotypes
Gene mutations
The Cottage Physician (1893)
References
Acute myeloid leukemia statistics. Cancer.net. Accessed on 03/22/2020 [link]
Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA: a cancer journal for clinicians. 2017; 67(1):7-30. [pubmed]
Reilly JT. Pathogenesis of acute myeloid leukaemia and inv(16)(p13;q22): a paradigm for understanding leukaemogenesis? British journal of haematology. 2005; 128(1):18-34. [pubmed]
Levine EG, Bloomfield CD. Leukemias and myelodysplastic syndromes secondary to drug, radiation, and environmental exposure. Seminars in oncology. 1992; 19(1):47-84. [pubmed]
Shuryak I, Sachs RK, Hlatky L, Little MP, Hahnfeldt P, Brenner DJ. Radiation-induced leukemia at doses relevant to radiation therapy: modeling mechanisms and estimating risks. Journal of the National Cancer Institute. 2006; 98(24):1794-806. [pubmed]
Austin H, Delzell E, Cole P. Benzene and leukemia. A review of the literature and a risk assessment. American journal of epidemiology. 1988; 127(3):419-39. [pubmed]
Shah A, Andersson TM, Rachet B, Björkholm M, Lambert PC. Survival and cure of acute myeloid leukaemia in England, 1971-2006: a population-based study. British journal of haematology. 2013; 162(4):509-16. [pubmed]
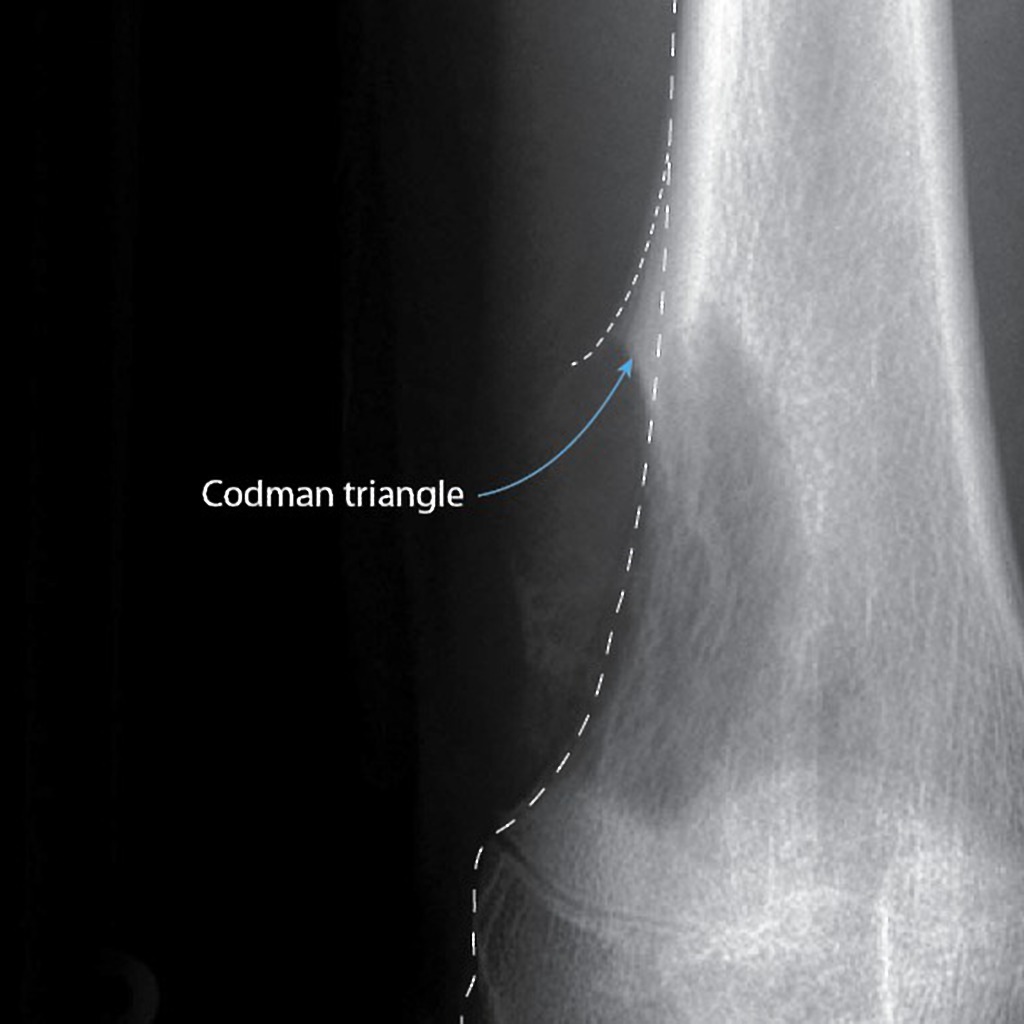
Definition – triangular area of new subperiosteal bone that is created when a bone tumor raises the periosteum away from the healthy bone
Clinical Significance – this occurs because the tumor is growing at a faster rate than the periosteum can expand, which leads to the periosteum tearing away and providing a second edge of ossification (thus making the triangle). Presence of this finding is highly suggested of a fast growing, malignancy.
History – Names after Ernest Amory Codman (1869-1940), who was an American surgeon and received his medical doctorate from Harvard University in 1895. Aside from being an accomplished surgeon, he fought for hospital reform and was an early adopter and advocate for patient-based outcomes. In fact, he created “End Result Cards” for his patients which included all diagnosis, procedures, and treatment for every one of his patients that he tracked for at least one year. He was also the first physician at Massachusetts General Hospital to institute a morbidity and mortality conference. Unfortunately, he lost his surgical privileges when he wanted to institute a plan for evaluating surgical competence. He went on to found his own hospital based on end-results and published these findings to the general public in 1916. He established the first bone tumor registry in the US and helped lead the founding of the American College of Surgeons and its Hospital Standardized Program, which eventually became the Joint Commission on Accreditation of Healthcare Organizations.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
You get a page from a gastroenterologist asking for a consult for platelet transfusion prior to an elective colonoscopy scheduled for tomorrow. The patient is a 56yo male, with a history of ITP and HTN. This procedure is for screening purposes only and the patient has not had any melena, hematochezia, or rectal bleeding. Platelet count is 97 x 109 per liter and the rest of the CBC is within normal limits.
Does this patient meet the platelet transfusion threshold?
If so, how much would you transfuse?
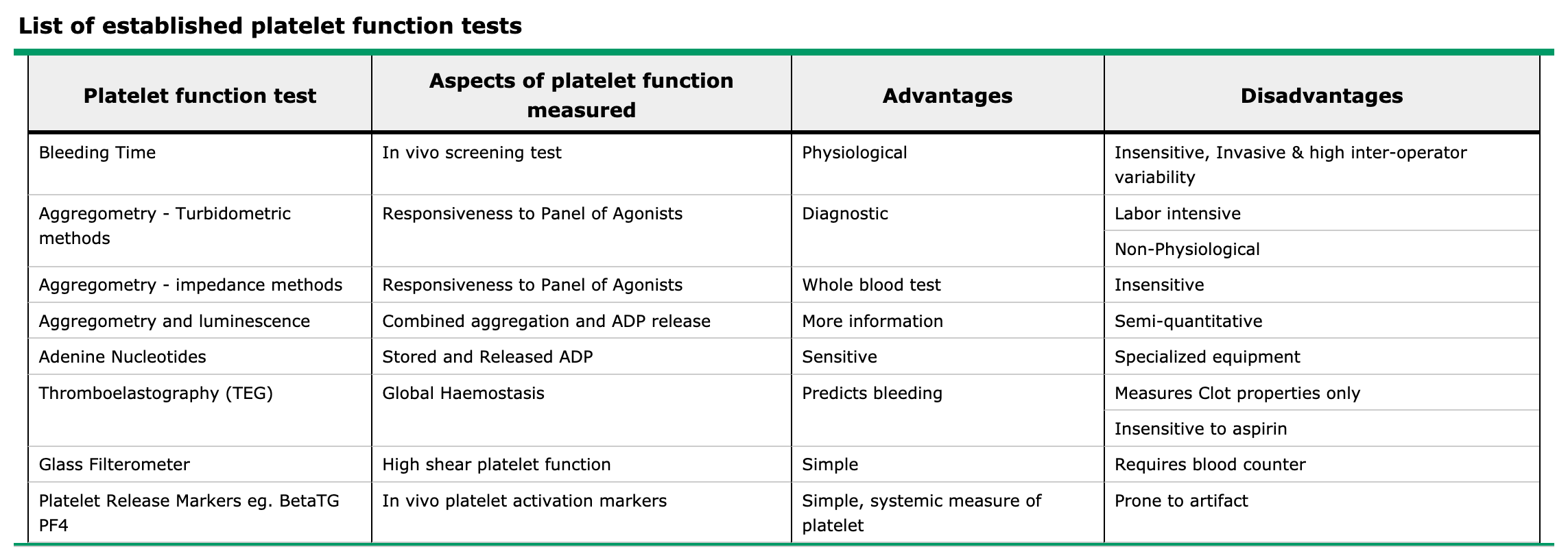
If you were worried about bleeding, what are the other tests you could order to assess platelet function?
Answer
The short answer is no, as he is not actively bleeding nor has any signs of anemia from chronic blood loss. Guidelines for platelet transfusions in preparation of invasive procedures is as follows:
< 100,000/microL for neurosurgery or ocular surgery
< 50,000/microL for most major surgery
< 50,000/microL for therapeutic endoscopic procedures
< 20,000/microL for low risk diagnostic endoscopic procedures
< 30,000/microL for bronchoscopy
< 20,000/microL for central line placement
< 20,000/microL for lumbar puncture with hematologic malignancy
< 50,000/microL for lumbar puncture without hematologic malignancy
< 80,000/microL for epidural anesthesia
< 20,000/microL for bone marrow biopsy
The best way to assess platelet function is from a platelet function assay. This is generally determined by your facility’s lab, so it would be a good idea to talk with your lab to see what they use and how to interpret.
References
Kumar A, Mhaskar R, Grossman BJ, et al. Platelet transfusion: a systematic review of the clinical evidence. Transfusion. 2015; 55(5):1116-27; quiz 1115. [pubmed]
Warner MA, Woodrum D, Hanson A, Schroeder DR, Wilson G, Kor DJ. Preprocedural platelet transfusion for patients with thrombocytopenia undergoing interventional radiology procedures is not associated with reduced bleeding complications. Transfusion. 2017; 57(4):890-898. [pubmed]
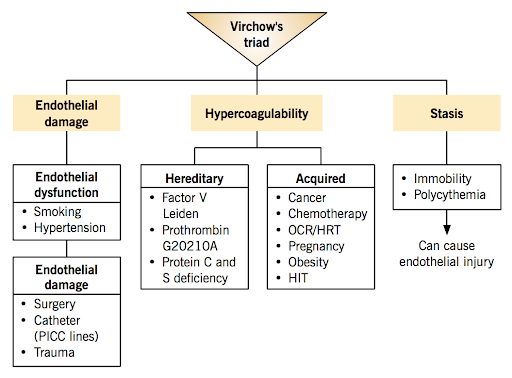
Definition – triad of broad categories of factors that contribute to thrombosis: hypercoaguability, endothelial injury, and stasis of blood flow
Clinical Significance – These factors should always be considered in patients with suspected DVT, PTE, or acute arterial occlusion. Thought broad, they represent a simplistic mindmap to think of differential diagnoses and causes for patients with suspected conditions.
History – Names after Rudolf Ludwig Carl Virchow (1821-1902), who was a German physician and received his medical doctorate from the Friedrich-Wilhelms Institute in 1843. He had an interesting career in that he was a prolific writer (producing more than 2000 scientific manuscript), but also very politically charged and challenged not only the government, but also the status quo of medical education and dogmatism. This fervor allowed him to push the boundaries of what was known and being taught in medical schools and made him a well-known teacher, orator, and leader in the field of pathology. He first published his treatise on thrombosis in 1856 where he described his triad, but the eponym was not attributed to him until the mid-1900s.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
You get a page from a gastroenterologist asking for a consult for platelet transfusion prior to an elective colonoscopy scheduled for tomorrow. The patient is a 56yo male, with a history of ITP and HTN. This procedure is for screening purposes only and the patient has not had any melena, hematochezia, or rectal bleeding. Platelet count is 97 x 109 per liter and the rest of the CBC is within normal limits.
Does this patient meet the platelet transfusion threshold?
If so, how much would you transfuse?
If you were worried about bleeding, what are the other tests you could order to assess platelet function?
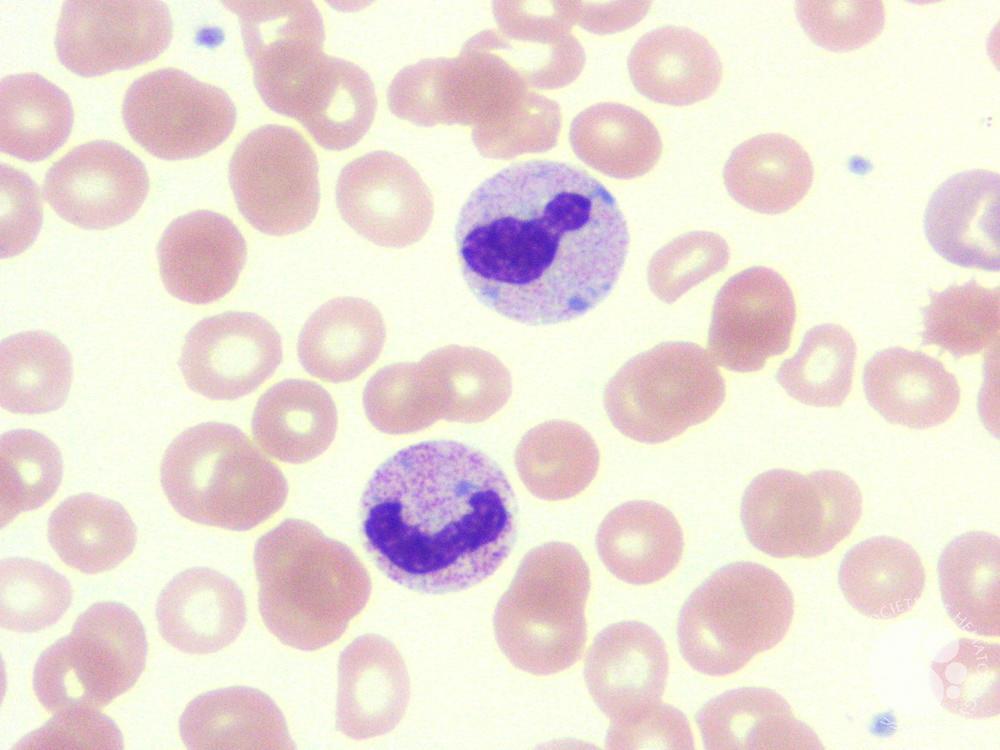
Definition – light, blue-gray intra-cytosplasmic structures composed of agglutinated ribosomes most commonly found on neutrophils
Clinical Significance – These inclusions are thought to be the remnants of the rough endoplasmic reticulum and represent defects in cell production and maturation during granulocytopoesis. As a result, Döhle bodies are seen in patients with infection, inflammation, and/or high physiologic stress, but may also be seen in pregnancy.
History – Named after Karl Gottfried Paul Döhle (1885-1928), who was a German pathologist and received his medical doctorate from the University of Kiel in 1882. He joined the faculty at his alma mater (where he would remain for his entire career) as an assistant to Arnold Ludwig Heller in 1883. He was an introvert by nature and rarely attended medical conferences and published very little of his work, but was well-renowned across his university. His work with Heller on describing syphilitic aortitis was groundbreaking and what eventually brought him contemporary fame in the field of histopathology. He published his findings on his eponymous cells in an article in 1892
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Döhle KGP. Vorläufige Mittheilung über Blutbefunde bei Masern. Zentralblatt für allgemeine Pathologie und pathologische Anatomie. Jena. 1892;3:150-152.
Other Known Aliases – Polycystic Ovarian Syndrome (PCOS)
Definition – clinical syndrome of hyperandrogenism, oligoanovulation, and polycystic ovaries.
Clinical Significance – PCOS is the most common cause of female infertility and should be investigated in women as part of the infertility workup. Women with PCOS can also have acne, hirsutism, menstrual irregularity, virilization, obesity, insulin-resistance, and metabolic syndrome. It is typically diagnosed in adolescents due to the phenotypic syndromic features.
History – Named after Irving F. Stein, Sr. (1887-1976) and Michael L. Leventhal (1901-1971) and both received their medical doctorates from Rush Medical College in 1912 and 1924 respectively. Both met while practicing at Michael Reese Hospital in early to mid-1900s. They presented a case report of 7 cases of amenorrhea, hirsutism, obesity, and enlarged polycystic ovarias in 1934 at the Central Association of Obstetrics and Gynecologists. They published these findings one year later in 1935 in an article entitled “Amenorrhea associated with bilateral polycystic ovaries” in the Americal Journal of Obstetrics and Gynecology. It should be noted that Russian gynecologist S.K. Lesnoy first described polycystic ovaries in 1928, but not the complete syndrome.
Stein
Leventhal
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
31yo, G0P000, is being evaluated in your clinic for infertility. She and her partner have been trying for 3 years to conceive and have not been successful. She report her partner has already had a semen analysis performed and was within normal limits. She reports a regular menstrual cycle, with little to no variability, and normal flow. She has not been on any form of contraception for 3 years. The rest of her past medical history and family history is benign.
What are types of studies that can be used in her infertility work-up?
Answer
Assessment of Ovulatory Function
Mid-luteal phase serum progesterone typically drawn seven days prior to the start of her menstrual cycle
> 3 ng/mL = recent ovulation
Assessment of Ovarian Reserve
Anti-müllerian hormone (AMH) reflects the size of the follicle pool
Clomiphene citrate challenge test (CCCT)
100mg clomiphene on day 5-9 and measurement of day 3 and day 10 FSH and day 3 estradiol
Assessment of Fallopian Tube Patency
Hysterosalpingogram
Assessment of Uterine Cavity
can be assessed via HSG, but can also be assessed with a saline-infusions sonohysterography or hysteroscopy