A 5yo boy is brought to you clinic by his parents for reporting that his legs hurt “when he plays too much”. His parents corroborate this saying that when he is climbing on the playground for too long he complains that his legs hurt and he needs to stop and rest for awhile. Vaccinations are UTD and he has had a relatively healthy childhood without significant illnesses. He has no significant past medical history and mother reports that she was 38 weeks when he was born via NSVD without any complications. Cardiac auscultation reveals a normal S1 and S2 without murmurs, gallops, or rubs.
What would you expect to find on physical examination?
What other physical assessment can you perform at the bedside to help with the diagnosis?
What findings on diagnostics would also help with the diagnosis?
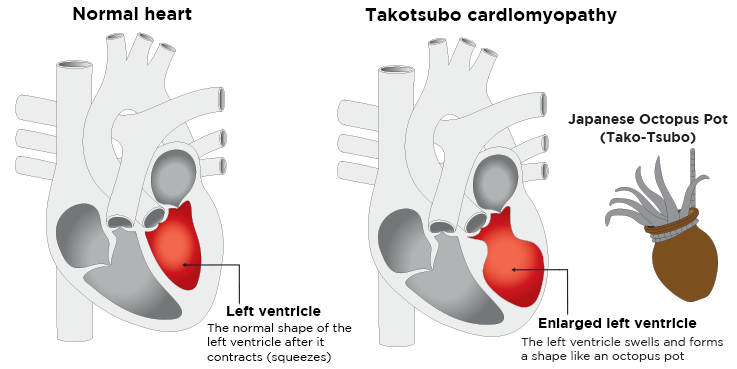
Clinical Significance – this syndrome is characterized by transient regional systolic dysfunction of the left ventricle, that mimics a myocardial infarction, but with an absence of angiographic evidence of coronary artery involvement.
History – Named after Japanese word for “octopus trap” as the left ventricle takes the shape of this unique hunting vessel. This condition was first studied in Japan by Hikaru Sato in 1991, but it was not “introduced” to the western medical world until 1997.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
73yo man, with a history of hypertension and coronary disease, is brought into the emergency room after a witnessed syncopal episode at home. He reported some mild exertional chest pain over the past few days, but states that it improved with rest. Vital signs are BP-180/98, HR-74, RR-12, and O2-100%. He is currently in no distress and not diaphoretic. Physical examination revealed a systolic murmur over the 2nd right intercostal space. A CT was ordered to rule-out PTE in the setting of chest pain and syncope and is below, along with the murmur.
What is the diagnosis?
How would you describe this murmur?
Where would you expect this murmur to radiate?
What is the classic triad associated with this condition?
Answer
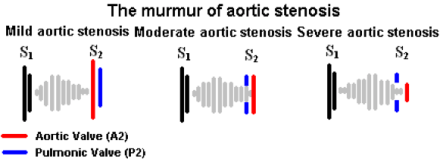
Aortic Stenosis due to a calcified aortic valve
High-pitched, crescendo-decrescendo (diamond shaped), midsystolic, ejection murmur with a soft S2
AS murmurs transmit well and equally to the carotid arteries
The classic triad of AS is exertional angina, exertional dyspnea, and dizziness/syncope
Definition – lines seen on chest radiography due to interstitial edema
Clinical Significance – Kerley lines are thin pulmonary opacities caused by fluid or cellular infiltration into the interstitial of the lungs. There are three distinct types that are seen:
Kerley A lines – linear opacities extending from the periphery to the hilum caused by distention of anastomotic channels between peripheral and central lymphatics
Kerley B lines – short horizontal lines situated perpendicularly to the pleural surface at the lung base and represent edema of the interlobar septa
Kerley C lines – reticular opacities at the lung base representing Kerley B lines en face
White Arrows (A lines); White Arrowheads (B lines); Black Arrowheads (C lines)
History – Named after Sir Peter James Kerley (1900-1979), who was an Irish radiologist and received his medical doctorate from Cambridge University in 1932. He went on to study in Vienna, which was the center of the new and blossoming specialty of heart and lung radiography. He assisted to editing “A Textbook of X-ray Diagnosis” in 1939, which was a major radiology textbook at the time, and later became director of radiology at Westminster Hospital in 1939. He first described his eponymonic findings in an article entitled “Radiology in heart disease” in 1933, and further elaborated on them in the second volume of his textbooks in 1951. During this year, he was also a key figure in the diagnosing of King George VI’s lung cancer due to his review of the King’s radiographs. He received several Royal awards for mass radiological screening for tuberculosis and his diagnosis of King George VI cancer, leading up to his Knight Commander of the Royal Victorian Order by Queen Elizabeth in 1972.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
73yo man, with a history of hypertension and coronary disease, is brought into the emergency room after a witnessed syncopal episode at home. He reported some mild exertional chest pain over the past few days, but states that it improved with rest. Vital signs are BP-180/98, HR-74, RR-12, and O2-100%. He is currently in no distress and not diaphoretic. Physical examination revealed a systolic murmur over the 2nd right intercostal space. A CT was ordered to rule-out PTE in the setting of chest pain and syncope and is below, along with the murmur.
What is the diagnosis?
How would you describe this murmur?
Where would you expect this murmur to radiate?
What is the classic triad associated with this condition?
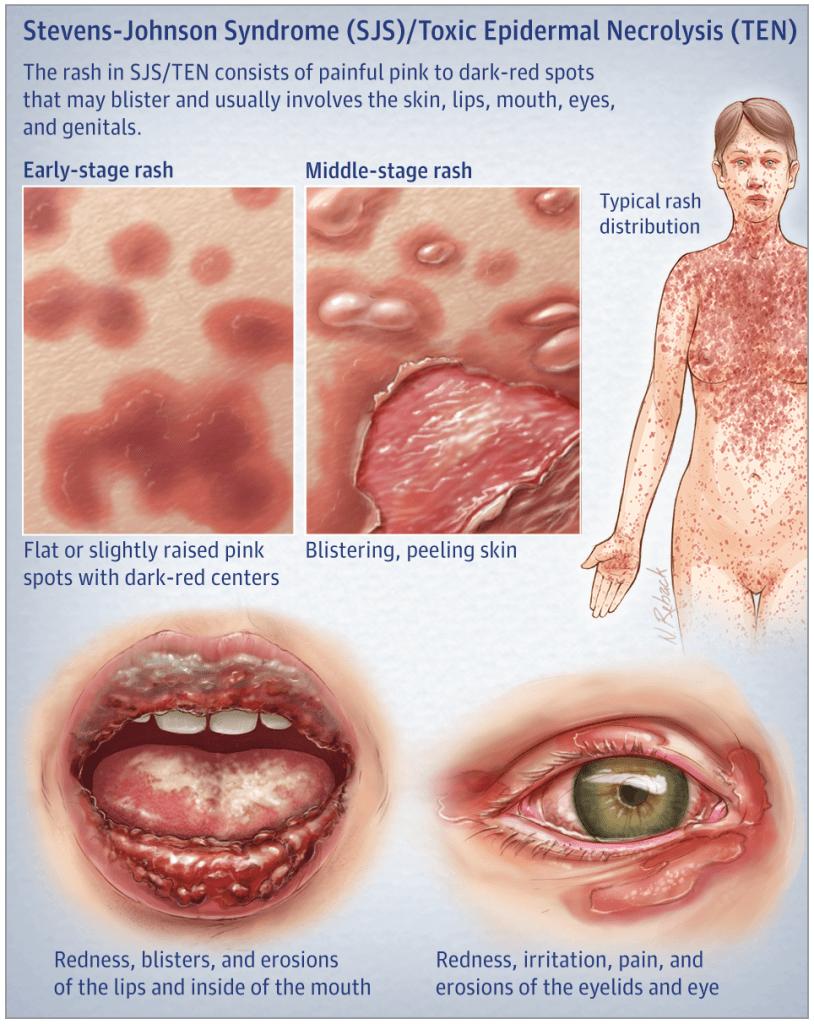
A 29yo patient is seen for a severe drug reaction after starting lamotrigine (Lamictal) for new-onset epilepsy. She has significant desquamation of her mucous membranes as well as large patches of denuded epidermis with multiple bullae present.
What is the clinically distinguishing feature between Steven-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN)?
Answer
The main clinical difference between SJS and TEN is the severity and degree of involvement. SJS classically is < 10% TBSA involvement, where as TEN is > 30% TBSA.
Definition – Exfoliation of the outermost layer and elicitation of blistering as a result of gentle mechanical pressure on the skin
Clinical Significance – This sign is classically associated with pemphigus vulgaris and is used to differentiate vulgaris (where it is present) and bullous (where it is absent). It is also present in Stevens-Johnson Syndrome, Toxic Epidermal Necrolysis, and scalded skin syndrome.
History – Named after Pyotr Vaseilyevich Nikolsky (1858-1940), who was a Russian dermatologist and received his medical doctorate from the Saint Vladimir Imperial University of Kiev in 1884. His doctoral dissertation and thesis was on pemphigus foliaceus, where he described his now famous eponym. He went on to have a career in academic medicine becoming professor at the Imperial University of Warsaw and establishing the Department of Dermatology and Venerology at the future Southern Federal University.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Grando SA, Grando AA, Glukhenky BT, Doguzov V, Nguyen VT, Holubar K. History and clinical significance of mechanical symptoms in blistering dermatoses: a reappraisal. Journal of the American Academy of Dermatology. 2003; 48(1):86-92. [pubmed]
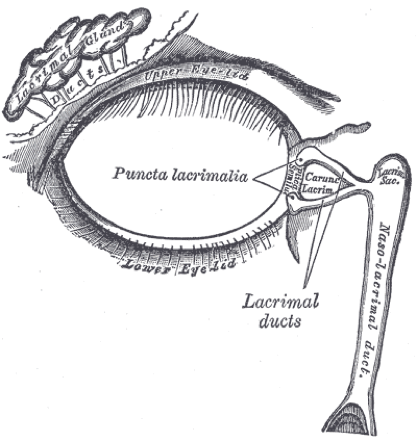
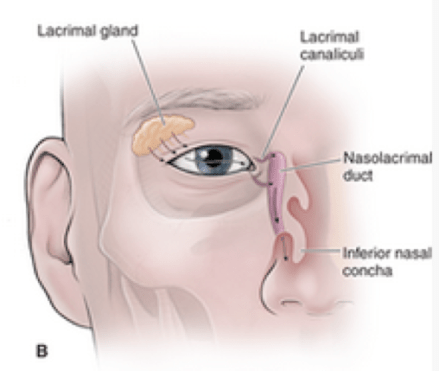
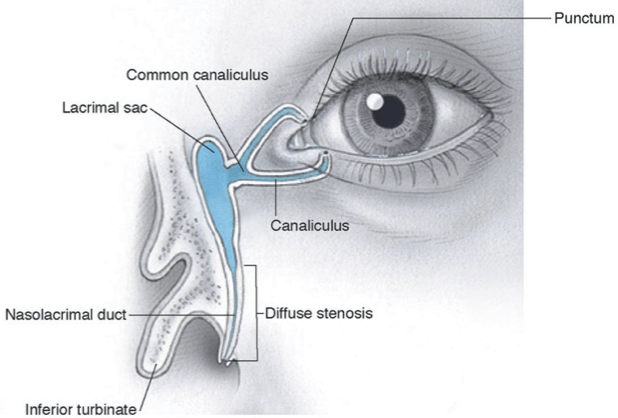
Dacryocystorhinostomy is required to prevent recurrence
Permanent fistula formed between lacrimal sac and the nose
The Cottage Physician (1893)
References
Duncan JL, Parikh NB, Seitzman GD, Riordan-Eva P. Disorders of the Lids & Lacrimal Apparatus. In: Papadakis MA, McPhee SJ, Rabow MW. eds. Current Medical Diagnosis and Treatment 2020. New York, NY: McGraw-Hill
Orbit. In: Morton DA, Foreman K, Albertine KH. eds. The Big Picture: Gross Anatomy, 2e New York, NY: McGraw-Hill;
Vagefi M. Lids & Lacrimal Apparatus. In: Riordan-Eva P, Augsburger JJ. eds. Vaughan & Asbury’s General Ophthalmology, 19e New York, NY: McGraw-Hill
Horton JC. Disorders of the Eye. In: Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. eds. Harrison’s Principles of Internal Medicine, 20e New York, NY: McGraw-Hill
Hoffmann J, Lipsett S. Acute Dacryocystitis. The New England journal of medicine. 2018; 379(5):474. [pubmed]
Campolattaro BN, Lueder GT, Tychsen L. Spectrum of pediatric dacryocystitis: medical and surgical management of 54 cases. Journal of pediatric ophthalmology and strabismus. ; 34(3):143-53; quiz 186-7. [pubmed]
Qian Y, Traboulsi EI. Lacrimal sac compression, not massage. Journal of pediatric ophthalmology and strabismus. ; 46(4):252. [pubmed]
Örge FH, Boente CS. The lacrimal system. Pediatric clinics of North America. 2014; 61(3):529-39. [pubmed]
A 29yo patient is seen for a severe drug reaction after starting lamotrigine (Lamictal) for new-onset epilepsy. She has significant desquamation of her mucous membranes as well as large patches of denuded epidermis with multiple bullae present.
What is the clinically distinguishing feature between Steven-Johnson Syndrome and Toxic Epidermal Necrolysis?
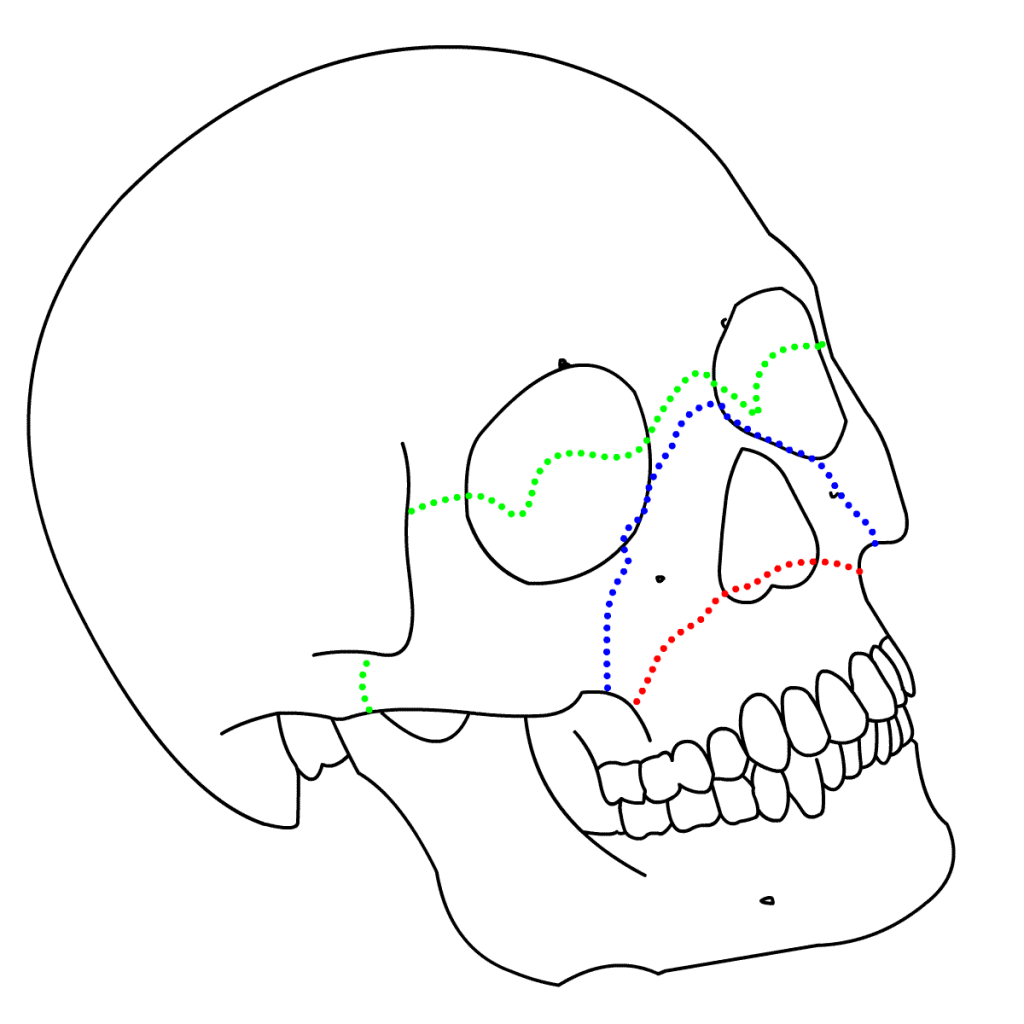
Other Known Aliases – transfacial fracture of the midface
Definition – These fractures involve the maxillary bone and are graded based on their direction and involvement of surrounding structures. The key distinguishing feature of this type of fracture is separation of the pterygoid plates from the maxillary sinuses.
Clinical Significance – Continuity of the pterygoid plates is essential for midface structural stability and any disruption requires surgical fixation. There are three types of Le Fort fractures:
Type I – Horizontal fracture – involves the lateral bony margin of the nasal opening
Type II – Pyramidal fracture – involves the inferior orbital rim
Type III – Transverse fracture – involves the zygomatic arch, vomer, and across the orbital floor and walls
History – Named after René Le Fort (1869-1951), who was a French surgeon and received his medical doctorate at the age of 21 while serving in the French military. He taught and practice in Lille, France for the majority of his career. He served his country numerous times when called to serve as a military physician, as well as coming out of retirement during World War II to teach at the University of Lille to replace colleagues called to the war effort. He published the findings of his eponymous conditions in 1901 in a treatise entitled “Étude expérimentale sur les fractures de la mâchoire supérieure”, where he described his experiments of dropping cannon balls from varying directions and heights on the faces of cadavers to describe the predictable injury patterns
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Gartshore L. A brief account of the life of René Le Fort. The British journal of oral & maxillofacial surgery. 2010; 48(3):173-5. [pubmed]
Patterson R. The Le Fort fractures: René Le Fort and his work in anatomical pathology. Canadian journal of surgery. Journal canadien de chirurgie. 1991; 34(2):183-4. [pubmed]
Le Fort R. Étude expérimentale sur les fractures de la machoire supérieure. Revue de chirurgie, Paris 1901; 23: 208-27; 360-79; 479-507