Other known aliases – atrioventricular bypass tract
Definition – As discussed in the WPW eponym, the Bundle of Kent is an accessory conduction pathway between the atrium and ventricle on either the right or left side of the heart.
Clinical Significance – this pathway occurs in up to 0.3% of patients and the cause of Wolff-Parkinson-White syndrome. It bypasses the traditional conduction system and allows for pre-excitation tachydysrthymias.
History – Named after Albert Frank Stanley Kent (1863-1958), an English physiologist who received his degree in 1886 from the Magdalen College of Oxford. He first described lateral atrioventricular connections in a monkey heart in 1893 and erroneously believed these were part of the normal specialized conduction system. These findings generated a lot of controversy at the time and were actually rejected by several notable anatomists and physiologists. In fact, in 1955, Lev and Learner dissected 33 neonatal hearts and found no evidence of “normal” lateral conduction systems.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Kent AF. Researches on the Structure and Function of the Mammalian Heart. The Journal of physiology. 1893; 14(4-5):i2-254. [pubmed]
LEV M, LERNER R. The theory of Kent; a histologic study of the normal atrioventricular communications of the human heart. Circulation. 1955; 12(2):176-84. [pubmed]
Other known aliases – ventricular pre-excitation with arrhythmia, auriculoventricular accessory pathway syndrome
Definition – paroxysmal supraventricular tachycardia caused by conduction through an abnormal accessory bypass tract between the atria and ventricles known as the Bundle of Kent. There are two types depending on the side of the heart it effects; Type A is between the right atrium and ventricle and Type B is between the left atrium and ventricle.
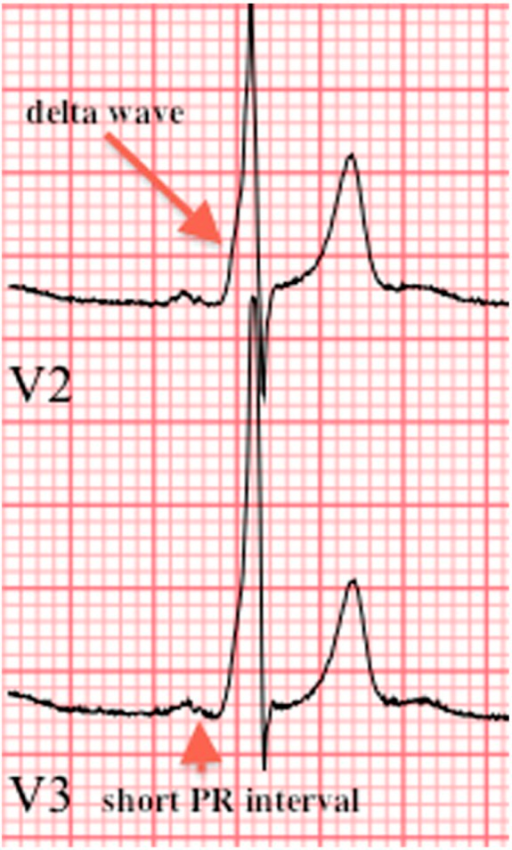
Clinical Significance – Patients with WPW can numerous cardiac dysfunction symptoms including tachydysrhythmias, palpitations, dyspnea, presyncope, syncope, and sudden cardiac arrest. It is characterized by the triad of abnormalities on EKG of widened QRS, shortened PR interval, and slurring of the initial part of the QRS (called a delta wave).
History – Named after Louis Wolff (1898-1972), Sir John Parkinson (1885-1976), and Paul Dudley White (1886-1973). Dr. Wolff was an American cardiologist who received his medical doctorate from Harvard Medical School in 1922. Dr. Parkinson was an English cardiologist who received his medical doctorate from University of Freiburg in 1910 and was also knighted by King George in 1948. Dr. White was an American cardiologist who received his medical doctorate from Harvard Medical School in 1911 and one of the founding presidents for the American Heart Association. He was a prominent advocate for preventive medicine receiving many national and international awards for his efforts to advance the importance of diet, exercise, and weight control in the prevention of cardiovascular disease. They collaborated to publish a series of 11 cases entitled “Bundle‐Branch Block with Short P‐R Interval in Healthy Young People Prone to Paroxysmal Tachycardia” in the American Heart Journal in 1930. It should be noted that Dr. Frank Norman Wilson and Dr. Alfred Wedd both described and published these findings in 1915 and 1921.
Wolff
Parkinson
White
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Wolff L, Parkinson J, White PD. Bundle‐Branch Block with Short P‐R Interval in Healthy Young People Prone to Paroxysmal Tachycardia. American Heart Journal. 1930;5(6):985-704 [article]
Other known aliases – Langer’s lines of skin tension, cleavage lines
Definition – topographical lines on the human body that correspond to the natural orientation of the collagen fibers of the dermis and are parallel to the orientation of the underlying muscle fibers
Clinical Significance – Incisions made on the skin that run parallel with these lines produce much less tension on the wound, heal better with less scarring, and have a much better cosmetic appearance. This is important in cosmetic surgery applications, as well as elective surgical procedures when you can select where to make your incision.
History – Named after Karl Langer (1819-1887), an Austrian anatomist, who received his medical doctorate from the Universities of Vienna and Prague. He worked under Joseph Hyrtl as a prosector for the University of Vienna and later becoming the director in 1874. In his famous procedure discovering these tension lines, he punctured circular holes on the skin of cadavers and noticed that they would result in ellipisoidal wounds. By following the direction of these ellipses, he was able to topographically map these lines on the entire body. He did give credit to Baron Dupuytren as being the first to observe this phenomenon and published his findings in 1861 entitled “Zur Anatomie und Physiologie der Haut. Über die Spaltbarkeit der Cutis”
Karl Langer
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
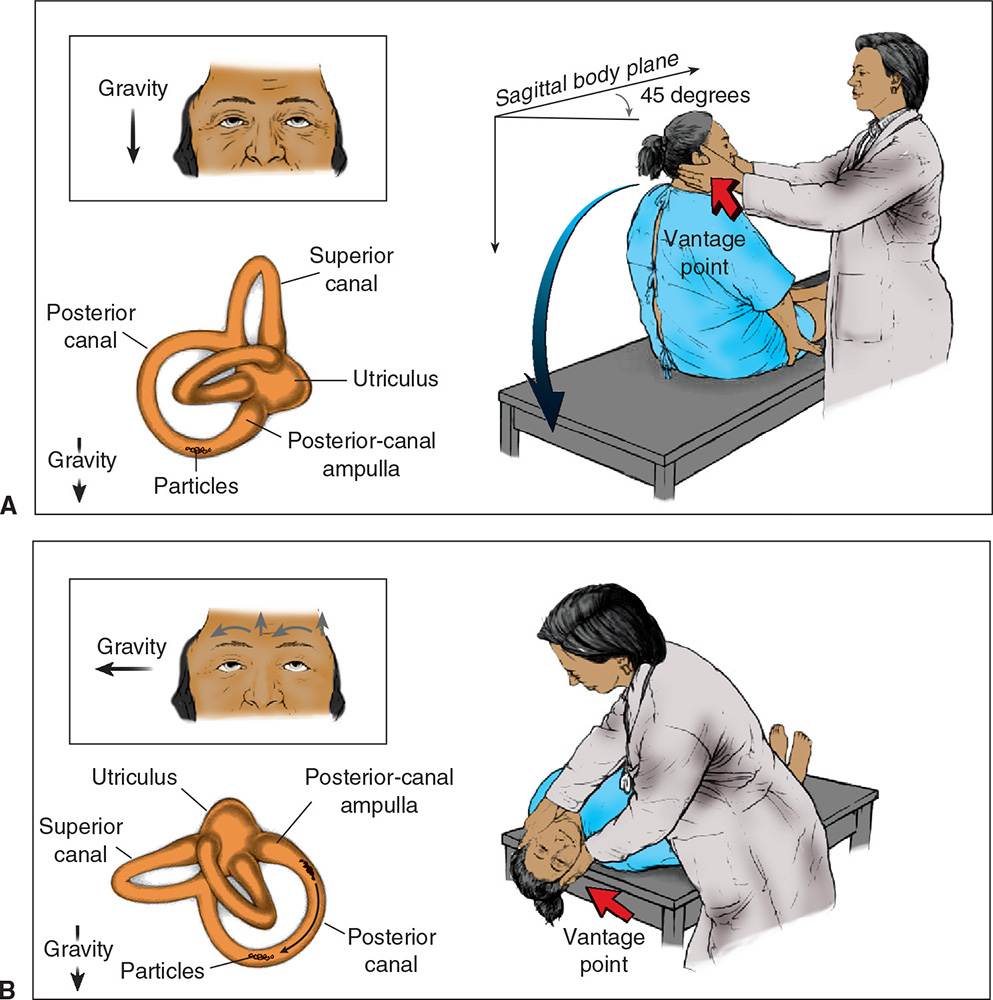
Definition – Starting supine, the patient’s head is rotated to one side and then quickly lowered to supine with the neck extended over the exam table. Patient is observed for nystagmus for 30 seconds and then returned to supine and observed for another 30 seconds. This is then repeated for the other side.
Clinical Significance – The Dix-Hallpike maneuver is the diagnostic maneuver to induce vertigo and nystagmus in patients with benign paroxysmal positional vertigo by relocating canaliths to the posterior semicircular canals.
History – Named after Margaret Ruth Dix (1902-1991), a British neuro-otologist, and Charles Skinner Hallpike (1900-1979), an English otologist. Dr. Dix earned her medical doctorate in 1937 from the Royal Free Hospital School of Medicine and Dr. Hallpike earned his from the University of London in 1926. Dr. Dix was training to become a surgeon when she was injured during the World War II air raids of London and suffered facial and ocular injuries which forced her to change her medical career path. It was during this time she was hired by Dr. Hallpike to pursue the field of neuro-otology. Their work resulted in a landmark series in the Proceedings of the Royal Society of Medicine and Annals of Otology, Rhinology, and Laryngology. It was this series in 1952 where one of the papers describing their eponymous finding entitled “The Pathology, Symptomatology, and Diagnosis of Certain Common Disorders of the Vestibular System” was published.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
DIX MR, HALLPIKE CS. The pathology symptomatology and diagnosis of certain common disorders of the vestibular system. Proceedings of the Royal Society of Medicine. 1952; 45(6):341-54. [pubmed]
Margaret Ruth Dix – Royal College of Surgeons [link]
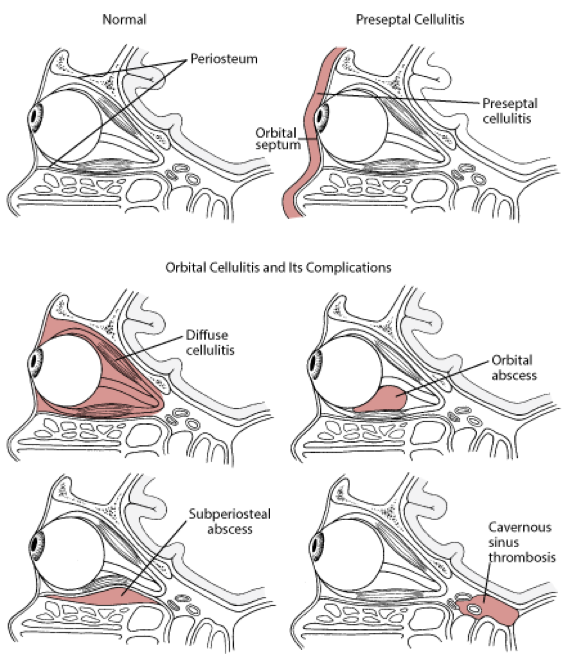
Both present with unilateral eyepain, erythema, and edema, but:
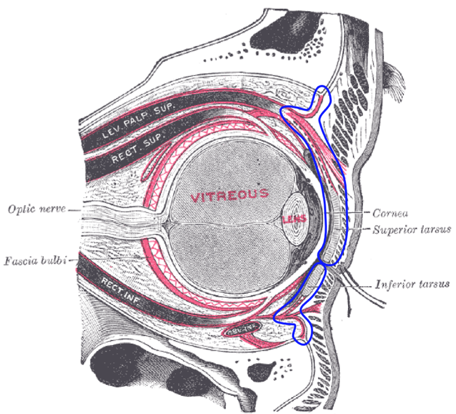
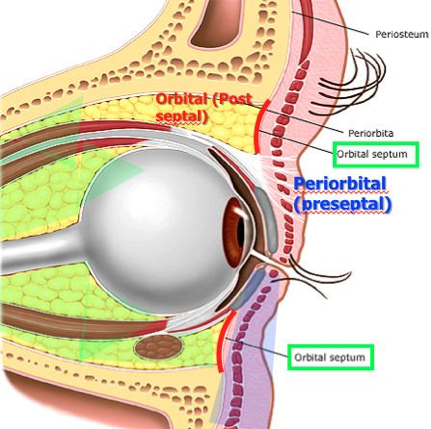
Preseptal
No pain with eye movement
Sclera is white
Preseptal Cellulitis (sclera is white and quiet)
Orbital
Painful eye movement
Vision changes (acuity, diplopia)
Proptosis
Sclera injection and chemosis
Decreased pupillary response
Orbital cellulitis (notice sclera is red and angry with chemosis)
Complications
Complications of preseptal cellulitis are rare, but orbital cellulitis can lead to:
Vision loss (3-11%)
Subperiosteal abscess
Orbital abscess
Cavernous sinus thrombosis
Diagnostic Studies
CBC with differential may be helpful in risk stratification or atypical presentation
Preseptal
None! –> Clinical diagnosis
Orbital
Indications for CT scan
Inability to assess vision or deteriorating vision
Double vision
Inability to examine due to age
Proptosis
Restricted, limited, and/or painfuleye movement
Edema extending beyond eyelid margin
Lack of improvement in 24 hours on antibiotics
Cyclical fevers
Signs of CNS involvement
ANC > 10,000 cell/microL
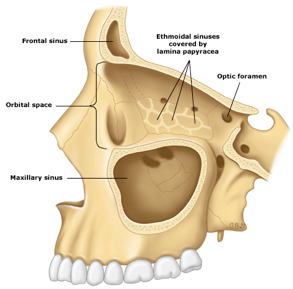
a.proptosis, b.soft tissue inflammation, c.choroidal detachment, d. retrobulbar inflammation, e. optic nerve sheet enhancementmedial orbital subperiosteal abscess with left sided ethmoid sinusitis
Blood cultures are not routinely recommended but should be entertained in ill appearing children prior to antibiotic administration
Treatment
Preseptal
Outpatient
> 1 year old and no signs of systemic toxicity
Treatment duration typically 5-7days, but treatment should continue until eyelid erythema and swelling have resolved
Inpatient
< 1 year old, children who can’t cooperate with exam, toxic appearance, or outpatient treatment failing to improve in 24-48 hours
Follow orbital cellulitis treatment
Orbital
Medical
Staphylococcal coverage
Vancomycin
Streptococcal coverage
Ceftriaxone
Cefotaxime
Anaerobic coverage
Metronidazole
Improvement should occur within24-48 hours
Transition to oral therapy when:
Afebrile and periorbital signs are resolving
Typically 3-5 days
Follow culture data (if obtained) or follow outpatient preseptal cellulitis regimen
Treat for a total of 2-3 weeks
Surgical indications
Radiographically identified abscess
Typically > 10mm, though small abscesses respond to antibiotics well
Intracranial extension
Failure to respond to antibiotic treatment
Threat to vision
References
Hauser A, Fogarasi S. Periorbital and orbital
cellulitis. Pediatrics in review. 2010; 31(6):242-9. [pubmed]
Botting AM, McIntosh D, Mahadevan M. Paediatric
pre- and post-septal peri-orbital infections are different diseases. A
retrospective review of 262 cases. International journal of pediatric
otorhinolaryngology. 2008; 72(3):377-83. [pubmed]
Chaudhry IA, Shamsi FA, Elzaridi E, Al-Rashed W,
Al-Amri A, Arat YO. Inpatient preseptal cellulitis: experience from a tertiary
eye care centre. The British journal of ophthalmology. 2008; 92(10):1337-41. [pubmed]
Moran GJ, Krishnadasan A, Gorwitz RJ, et al.
Methicillin-resistant S. aureus infections among patients in the emergency
department. The New England journal of medicine. 2006; 355(7):666-74. [pubmed]
Brook I, Frazier EH. Microbiology of
subperiosteal orbital abscess and associated maxillary sinusitis. The
Laryngoscope. 1996; 106(8):1010-3. [pubmed]
Erickson BP, Lee WW. Orbital Cellulitis and
Subperiosteal Abscess: A 5-year Outcomes Analysis. Orbit (Amsterdam,
Netherlands). 2015; 34(3):115-20. [pubmed]
Howe L, Jones NS. Guidelines for the management
of periorbital cellulitis/abscess. Clinical otolaryngology and allied sciences.
2004; 29(6):725-8. [pubmed]
Rudloe TF, Harper MB, Prabhu SP, Rahbar R,
Vanderveen D, Kimia AA. Acute periorbital infections: who needs emergent
imaging? Pediatrics. 2010; 125(4):e719-26. [pubmed]
Tanna
N, Preciado DA, Clary MS, Choi SS. Surgical treatment of subperiosteal orbital
abscess. Archives of otolaryngology–head & neck surgery. 2008;
134(7):764-7. [pubmed]
Greenberg
MF, Pollard ZF. Medical treatment of pediatric subperiosteal orbital abscess
secondary to sinusitis. Journal of AAPOS : the official publication of the
American Association for Pediatric Ophthalmology and Strabismus. 1998;
2(6):351-5. [pubmed]
Benign paroxysmal positional vertigo (BPPV) can be quite a debilitating condition for patient it effects. What are the two maneuvers that are used at the bedside for this condition and how do they differ?
Answer
The two maneuvers used clinically in the evaluation and treatment of BPPV are:
Dix-Hallpike Maneuver (diagnosis)
This is used to diagnosis BPPV and is performed by having the patient starting sitting upright. The head is then turned to one side and the patient is rapidly lowered to the supine position with their extended over the examination table. The provider then watches for nystagmus or vertigo symptoms. If this side is negative, then the maneuver is repeated on the other side.
Dix-Hallpike
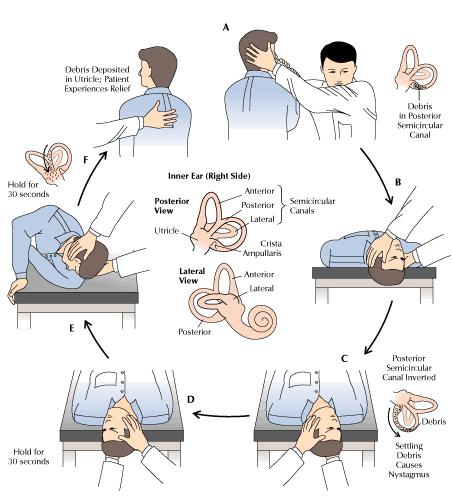
Epley Maneuver (treatment)
This is used to treat active vertigo in BPPV by attempting to relocate the canalith back into the utricle by using a series of repositioning techniques.
Epley
References
Shim DB, Ko KM, Kim JH, Lee WS, Song MH. Can the affected semicircular canal be predicted by the initial provoking position in benign paroxysmal positional vertigo? The Laryngoscope. 2013; 123(9):2259-63. [pubmed]
Furman JM, Cass SP. Benign paroxysmal positional vertigo. The New England journal of medicine. 1999; 341(21):1590-6. [pubmed]
Woodworth BA, Gillespie MB, Lambert PR. The canalith repositioning procedure for benign positional vertigo: a meta-analysis. The Laryngoscope. 2004; 114(7):1143-6. [pubmed]
White J, Savvides P, Cherian N, Oas J. Canalith repositioning for benign paroxysmal positional vertigo. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2005; 26(4):704-10. [pubmed]