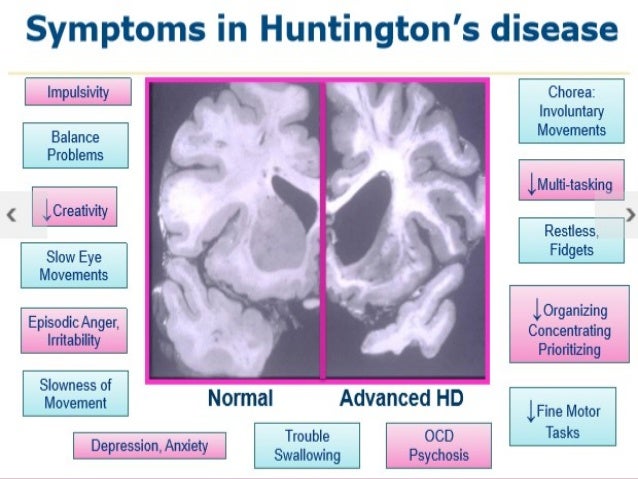
Definition – Autosomal dominant condition caused by expansion of the cytosine-adenine-guanine (CAG) trinucleotide repeats in the HD gene located on short arm of chromosome 4p16.3 that encodes the protein huntingtin.
Clinical Significance – This condition affects 4-15 in 100,000 peoples of European descent and is extremely rare in non-European lineage. The classic manifestations of the disease include chorea, psychiatric illness, and dementia. These symptoms begin very slow and are often missed for a period of time, but always progress to severe deterioration of neuromuscular function. It is uncurable and treatment is directed towards support and planning of care. Average length of survival after symptoms onset is 10-20 years
History –Named after George Huntington (1850-1916), an American physician who received his medical doctorate from Columbia University in 1871 at the age of 21. He came from a long line of physicians dating back to 1797, when his grandfather opened the family practice in East Hampton. He took meticulous notes on the disease that bears his name from going on house calls with his father early in his childhood, as well as reading and transcribing notes from his father and grandfather. He only published two papers in his career, the first of which was on this disease. He read this manuscript before the Meigs and Mason Academy of Medicine in Middleport, Ohio in 1872 (just 1 year after graduating medical school) and received such acclaim that it was published in the Medical and Surgical Reporter of Philadelphia just 2 months later. This paper was published in the German literature later that year and his name was forever attached to this disease. Even William Osler read and commented on this paper in 1908 saying ” In the history of medicine there are few instances in which a disease has been more accurately, more graphically, or more briefly described.”
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
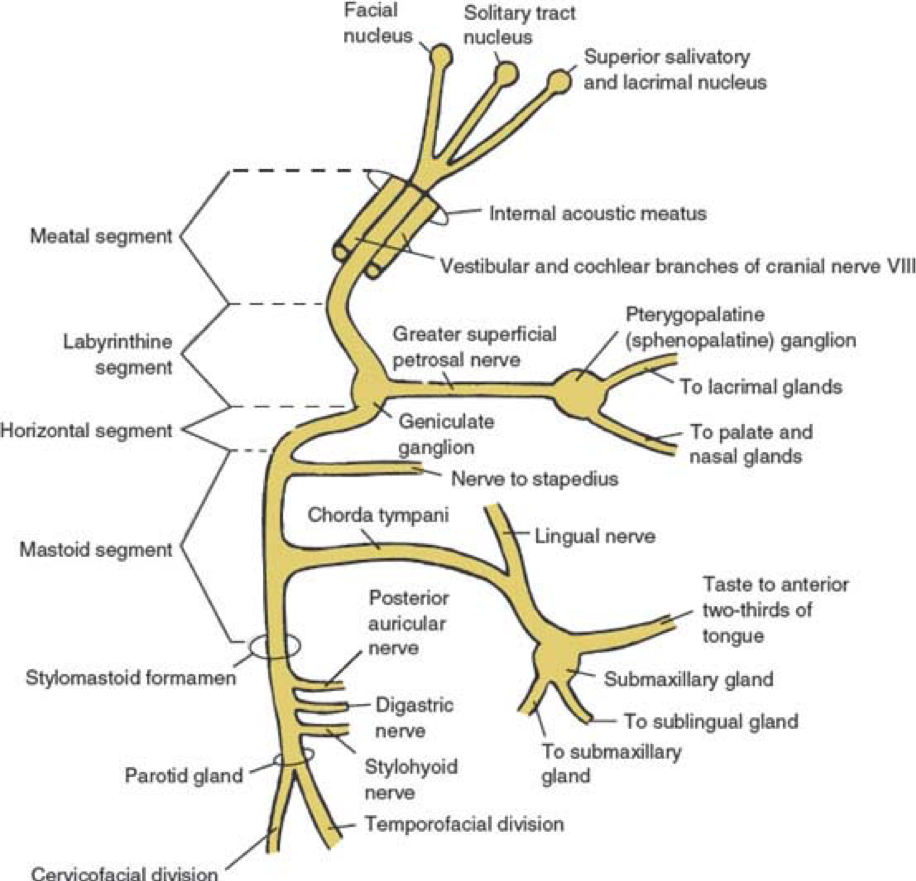
Tympanic (geniculate ganglion to pyramidal eminence)
Stapedius nerve
Mastoid (pyramidal eminence to stylomastoid foramen)
Chorda tympani à tongue, salivary glands, lingual nerve
Extratemporal (stylomastoid foramen to post parotid branches)
5 major facial branches
Temporal
Zygomatic
Buccal
Mandibular
Cervical
Definition and Epidemiology
Bell’s Palsy is an acute peripheral nerve palsy of unknown etiology and makes up almost half of such cases. It is estimated that the annual incidence is around 20 patient per 100,000 population. There is no race, geographic, or gender correlation., though there is some old data on increased risk during 3rd trimester of pregnancy.
Pathogenesis
Had been hotly debated for many years as to the cause of this condition and is generally considered to be caused by Herpes Simplex virus due to associated serologic evidence in effected patients. Newer data has been published, but is not entirely conclusive. Most agree that is due to some viral pathogen with herpes being the most common, but also implicating CMV, EBV, adenovirus, and coxsackievirus. Specifically, the signs and symptoms are a result of viral mediated inflammatory demyelination of the nerve.
Signs and Symptoms
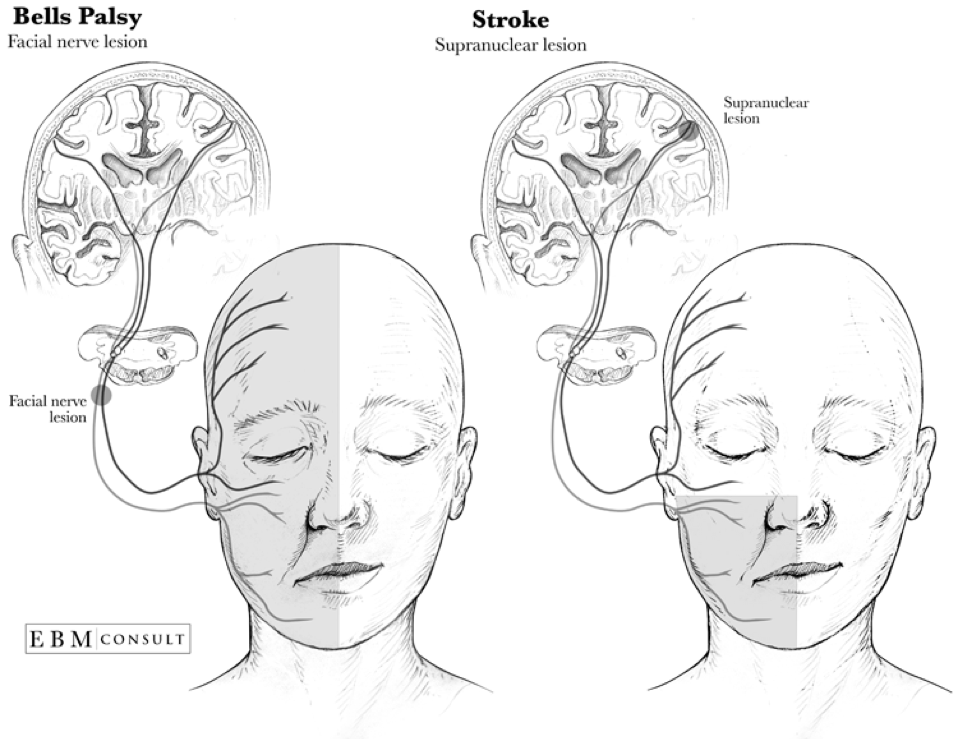
Most common presentation is acute (over several hours) unilateral facial paralysis with:
Motor
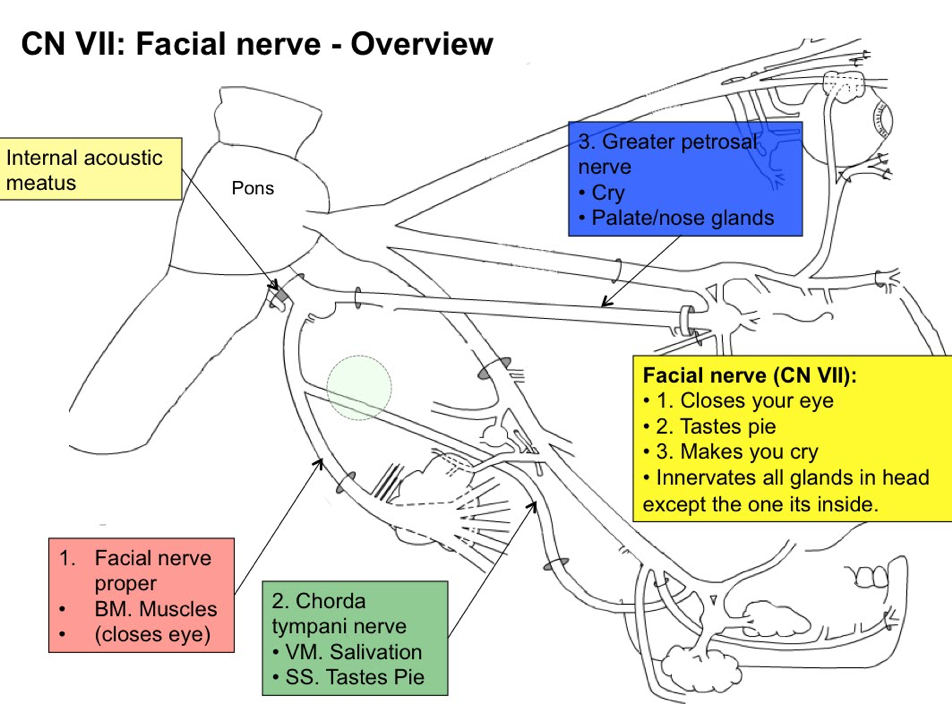
Inability to close the eye
Eyebrow sagging with inability to wrinkle the forehead
Obliteration of the nasolabial fold
Dropping of the affected corner of the mouth
Sensory
Hyperacusis
Loss of taste on the anterior 2/3rd of tongue
Symptoms are progressive and usually reach peak involvement within 3 weeks of onset. Patients should begin to have return of function within 2-4 months.
Diagnostic Studies
Bell’s palsy is a clinical diagnosis and diagnostic studies are generally not indicated unless the presentation is atypical, still progressing at 3 weeks, or there is no return of function by 4 months. History of facial twitching or spasms preceding the paralysis raises suspicion of compressive neuropathy from tumor or mass.
Electromyography (EMG)
The most simplest of the electrodiagnostic tests that can be used to show action potentials on active volition. Some degree of potential infers that the nerve is still intact and therefor, can improve.
Nerve Conduction Studies (NCS)
Supramaximal stimulation near the parotid gland with measured evoked potentials over the orbicularis oculi, nasalis, and lower facial muscles can measure the degree of axonal loss. Studies have shown >75% is the critical cutoff for low likelihood of full recovery. Ideally, this should be performed within 2 weeks of symptom onset for a more accurate prognosis.
Facial Nerve Stimulation
Should be considered with 2 weeks of symptoms onset if surgical decompression is considered due to potential for reversibility.
Needle EMG
Utilized after 3 weeks to assess the degree of axonal damage and evidence of subclinical reinnervation for recovery
Imaging
High-resolution, contrast-enhanced CT (for bony pathology) or gadolinium-enhanced MRI (for soft tissue structures) of the brain, temporal bone, and parotid gland.
Lyme serology should be entertained in patients from endemic regions.
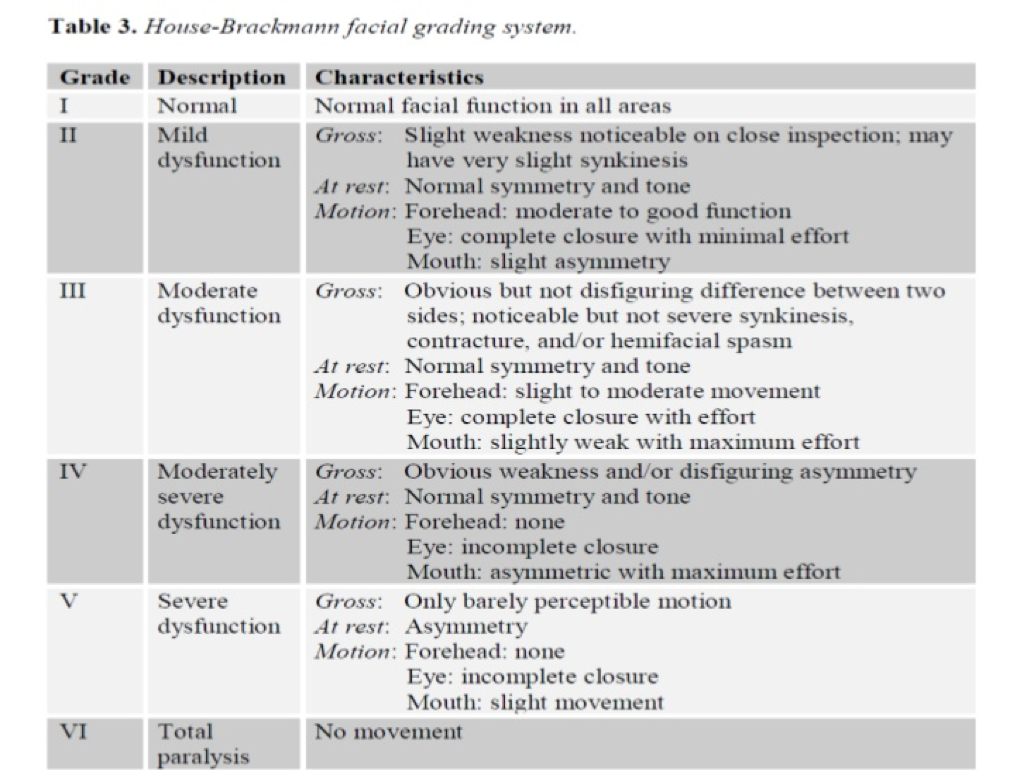
Severity Grading
The House-Brackman scale is the most common grading scale that uses objective criteria to score the severity, mark progression, and track return of function.
Treatment
Mainstay of therapy for Bell’s palsy is corticosteroids (for the inflammation) and antivirals (for the viral pathogens). Current recommendations are:
Prednisone 60-80mg daily for 7 days
Valacyclovir 1000mg TID for 7 days
Within 72 hours of symptoms onset
Eye care should include artificial tears and an eye patch for sleeping.
Prognosis
Favorable prognosis if any recovery is seen within 21 days of symptom onset with data showing 71% with complete resolution, 13% with slight residual sequelae, and 16% with residual weakness, synkinesis, or contracture. 94% of patients with incomplete involvement have full resolution, while only 60% of complete involvement returned to normal function.
References
Monkhouse WS. The anatomy of the facial nerve. Ear, nose, & throat journal. 1990; 69(10):677-83, 686-7. [pubmed]
May M, Klein SR. Differential diagnosis of facial nerve palsy. Otolaryngologic clinics of North America. 1991; 24(3):613-45. [pubmed]
Hilsinger RL, Adour KK, Doty HE. Idiopathic facial paralysis, pregnancy, and the menstrual cycle. The Annals of otology, rhinology, and laryngology. ; 84(4 Pt 1):433-42. [pubmed]
Peitersen E. Bell’s palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta oto-laryngologica. Supplementum. 2002; [pubmed]
Schirm J, Mulkens PS. Bell’s palsy and herpes simplex virus. APMIS : acta pathologica, microbiologica, et immunologica Scandinavica. 1997; 105(11):815-23. [pubmed]
Kennedy PG. Herpes simplex virus type 1 and Bell’s palsy-a current assessment of the controversy. Journal of neurovirology. 2010; 16(1):1-5. [pubmed]
Morgan M, Nathwani D. Facial palsy and infection: the unfolding story. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 1992; 14(1):263-71. [pubmed]
Liston SL, Kleid MS. Histopathology of Bell’s palsy. The Laryngoscope. 1989; 99(1):23-6. [pubmed]
Valls-Solé J. Electrodiagnostic studies of the facial nerve in peripheral facial palsy and hemifacial spasm. Muscle & nerve. 2007; 36(1):14-20. [pubmed]
May M, Klein SR, Taylor FH. Indications for surgery for Bell’s palsy. The American journal of otology. 1984; 5(6):503-12. [pubmed]
Gilden DH. Clinical practice. Bell’s Palsy. The New England journal of medicine. 2004; 351(13):1323-31. [pubmed]
House JW, Brackmann DE. Facial nerve grading system. Otolaryngology–head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 1985; 93(2):146-7. [pubmed]
Gronseth GS, Paduga R, . Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012; 79(22):2209-13. [pubmed]
Baugh RF, Basura GJ, Ishii LE, et al. Clinical practice guideline: Bell’s palsy. Otolaryngology–head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2013; 149(3 Suppl):S1-27. [pubmed]
Schwartz SR, Jones SL, Getchius TS, Gronseth GS. Reconciling the clinical practice guidelines on Bell’s palsy from the AAO-HNSF and the AAN. Otolaryngology–head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2014; 150(5):709-11. [pubmed]
de Almeida JR, Guyatt GH, Sud S, et al. Management of Bell palsy: clinical practice guideline. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne. 2014; 186(12):917-22. [pubmed]
Peitersen E. The natural history of Bell’s palsy. The American journal of otology. 1982; 4(2):107-11. [pubmed]
Other Known Aliases – 47XXY, Klinefelter-Reifenstein-Albright Syndrome
Definition – Genetic condition resulting from two (or more) X chromosomes in a male patient. It is the most common sex chromosome abnormality causing hypogonadism.
Clinical Significance – This condition affects 1 in 500-1000 newborn males in the United States. Symptoms can range from subtle (sometimes not even noticed) to severe learning, developmental, and cognitive deficiencies. The most prominent features are sterility, small testes, taller stature, less androgenic body hair, and gynecomastia. Due to these developmental abnormalities, it is often not diagnosed until after puberty
History –Named after Harry Fitch Klinefelter, Jr. (1912-1990), an American rheumatologist and endocrinologist, who earned is medical doctorate from Johns Hopkins University. He worked in the prestigious clinic of Dr. Fuller Albright at Massachusetts General Hospital where he studied a group of nine boys who all had similar features of gynecomastia, aspermatogenesis, and increased follicle-stimulating hormone. He credits Dr. Albright with this discovery, as it was his clinic and he first noticed the pattern, but Albright wanted Klinefelter to do the research work on it as a new fellow attending. The group (with Dr. Edward Reifenstein) published this cases series in 1942 and Dr. Albright insisted that Klinefelter take lead authorship.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Klinefelter HF, Reifenstein EC, Albright F. Syndrome Characterized by Gynecomastia, Aspermatogenesis without A-Leydigism, and Increased Excretion of Follicle-Stimulating Hormone. JCEM. 1942;2(11):615-627 [article]
Loriau DL. Chapter 89: Harry F. Klinefelter (1912-1990). A Biographical History of Endocrinology. 2016. [article]
A 3yo girl has been diagnosed with acute bacterial otitis media in your clinic and requires amoxicillin for treatment. The parents say she doesn’t take medicine every well and would appreciate the lowest VOLUME per dose. She weighs 32 lbs. What are the different dosing strategies using the current formulation of liquid amoxicillin?
Answer
Amoxicillin comes in 125mg/5mL, 200mg/5mL, 250mg/5mL, and 400mg/5mL and the recommended daily dose for bacterial acute otitis media is 90mg/kg/day twice daily for 7 days. She weighs 32lbs, which is 14.5kg, so she would need 1305mg per day, or 650mg per dose. For the different concentrations it could be:
For 125mg/5mL – 26mL per dose
For 200mg/5mL – 16mL per dose
For 250mg/5mL – 13mL per dose
If you want to have the LOWEST volume, then using the 400mg/5mL concentration would be 8.1mL per dose and you would need to dispense 115mL for a 7 day prescription.
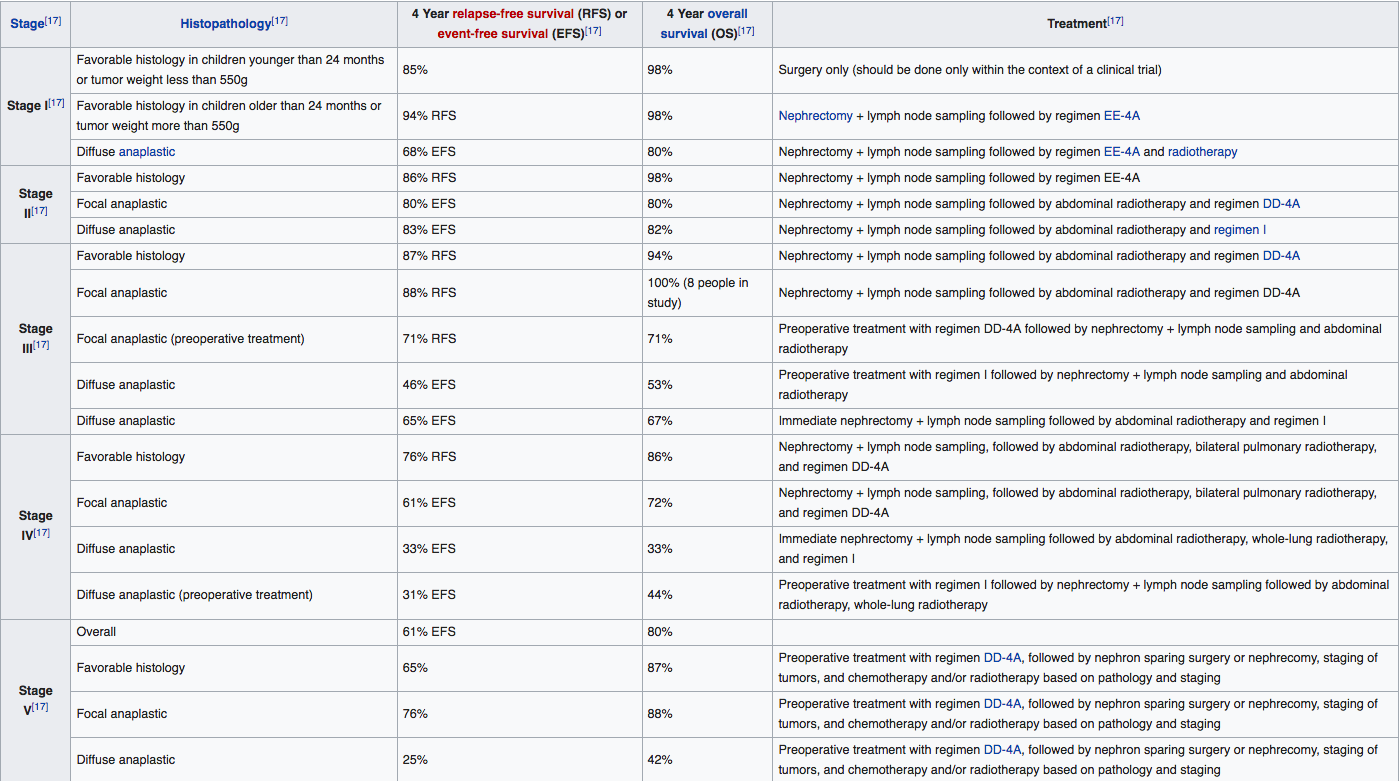
Definition – The most common childhood primary renal tumor and can occur due to a mutation in the WT-1 cancer suppressor gene on 11p13. There are five clinical stages depending on anatomical findings and tumor cell pathology.
Clinical Significance – Current estimates are around 500 new cases in the US per year and can be associated with several other genetic conditions including, WAGR syndrome, Denys-Drash syndrome, and Beckwith-Wideman syndrome. Most children, who are later diagnosed with a Wilm’s tumor, present with an asymptomatic abdominal mass easily palpable by the provider. Ultrasound is the initial screening test of choice, though MRI can be help in staging. A renal biopsy will confirm the diagnose and definitively stage the disease in order to select the best treatment modalities.
History –Named after Carl Max Wilhem Wilms (1867-1918), a German pathologist and surgeon, who earned his medical doctorate from the University of Bonn in 1890. He was a prolific surgeon and medical educator rising to the ranks of chair of surgery at the University of Heidelberg in 1910. He published his findings of the renal tumor that bears his name in 1899 in the article entitled “Die Mischgeschwülste der Niere”. There is some controversy on who identified this tumor first as Thomas Rance may have written on it in 1814, but it was not very specific and could be attributed to other renal malignancies. Felix Birch-Hirschfeld and colleagues also identified and wrote on what they believed to the first description of this tumor, but Wilms’ manuscript seemed to be more broadly noted in the literature and eventually came to bear his name.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
A 3yo girl has been diagnosed with acute bacterial otitis media in your clinic and requires amoxicillin for treatment. The parents say she doesn’t take medicine every well and would appreciate the lowest VOLUME per dose. She weighs 32 lbs. What are the different dosing strategies using the current formulation of liquid amoxicillin?
Other Known Aliases – familial/hereditary nonhemolytic unconjugated hyperbilirubinemia
Definition – Rare, familial condition resulting in congenital hyperbilirubinemia secondary to a deficiency of glucuronyl transferase. There two types, with type I being very rare and severe (absolute absence) and type II being more common and less severe (relative deficiency)
Clinical Significance – Congenital hyperbilirubinemia can have catastrophic effects on the infant including jaundice, lethargy, failure to thrive, hypotonia, kernicterus, and acute bilirubin encephalopathy once it saturates and binds to the brain tissue.
History – Named after:
1) John Fielding Crigler (1919-), who is an American pediatrician who earned his medical doctorate at Duke University in 1943 and practiced at the Children’s Hospital of Boston.
2) Victor Assad Najjar (1914-), who is a Lebonese-born, American pediatrician who earned his medical doctorate at the American University in Beirut and practiced at Johns Hopkins, Vanderbilt, and Tufts University.
They published their findings of a new disease causing congenital familial nonhemolytic jaundice with kernicterus in 1952.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
CRIGLER JF, NAJJAR VA. Congenital familial nonhemolytic jaundice with kernicterus; a new clinical entity. A.M.A. American journal of diseases of children. 1952; 83(2):259-60. [pubmed]
Which is associated with other genetic conditions?
Which has better associated outcomes?
Answer
The condition on the left is an omphalocele and on the right is a gastroschisis.
Omphalocele is a midline abdominal wall defect where the contents are covered by a membrane of amnion and peritoneum. It occurs at the base of umbilical cord.
Gastroschisis (more common) is a full-thickness, paraumbilical abdominal wall defect with free-evisceration of abdominal contents
The majority of infants with an omphalocele have associated congenital anomalies including Beckwith-Wiedemann syndrome, Trisomy 13 and 18, and numerous other subsystem involvement. Gastroschisis generally has no other abnormalities, but can have associated intestinal atresia in up to 10%
Gastroschisis has statistically better overall outcomes since it is not associated with any other genetic conditions.
References
Carlo WA. The Umbilicus. In: Nelson Textbook of Pediatrics. 20th ed. 2016. Chapter 105: 890-891.
Definition – 1-3mm, grey/green/brown pigmented ring in the Descemet membrane of the cornea. It first appears at the 12 o’clock position in early disease, then a second crescent forms at 6 o’clock, and then finally completely encircling the cornea.
Clinical Significance – This is pathognomonic for Wilson’s disease, but does not cause any symptoms with the patient. They are often identified on good ophthalmic examinations.
History – Named after Bernhard Kayser (1869-1954) and Bruno Fleischer (1874-1965), who were both German ophthalmologists and contemporaries of each other. Dr. Kayser received his medical doctorate at the University of Berlin in 1893 and practiced as a specialized ophthalmologist in Stuttgart, Germany for the majority of his career. Dr. Fleischer received his medical doctorate at the University of Tübingen in 1898 and practiced there earning a reputation as an extraordinary professor. Each published their findings in Klinische Monatsblätter für Augenheilkunde within a year of each other (1902 and 1903), but erroneously posited that it was due to silver accumulation. The first published report of copper being the causative agent was in 1934 by Dr. Werner Gerlach and Willhelm Rohrschneider.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Schrag A, Schott JM. Images in clinical medicine. Kayser-Fleischer rings in Wilson’s disease. NEJM. 2012; 366(12):e18. [pubmed]
Dusek P, Litwin T, Czlonkowska A. Wilson disease and other neurodegenerations with metal accumulations. Neurologic clinics. 2015; 33(1):175-204. [pubmed]
Kayser B. “Über einen Fall von angeborener grünlicher Verfärbung des Cornea”. Klin Monatsbl Augenheilk. 1902;40(2):22–25.
Fleischer B. “Zwei weitere Fälle von grünlicher Verfärbung der Kornea”. Klin Monatsbl Augenheilk. 1903;41(1):489–491
Gerlach W, Rohrschneider W. “Besteht das Pigment des Kayser-Fleischerschen Hornhautringes aus Silber?”. Klin Wochenschr. 1934;13: 48–49