***LISTEN TO THE PODCAST HERE***
Anatomy and Physiology of Cranial Nerve VII
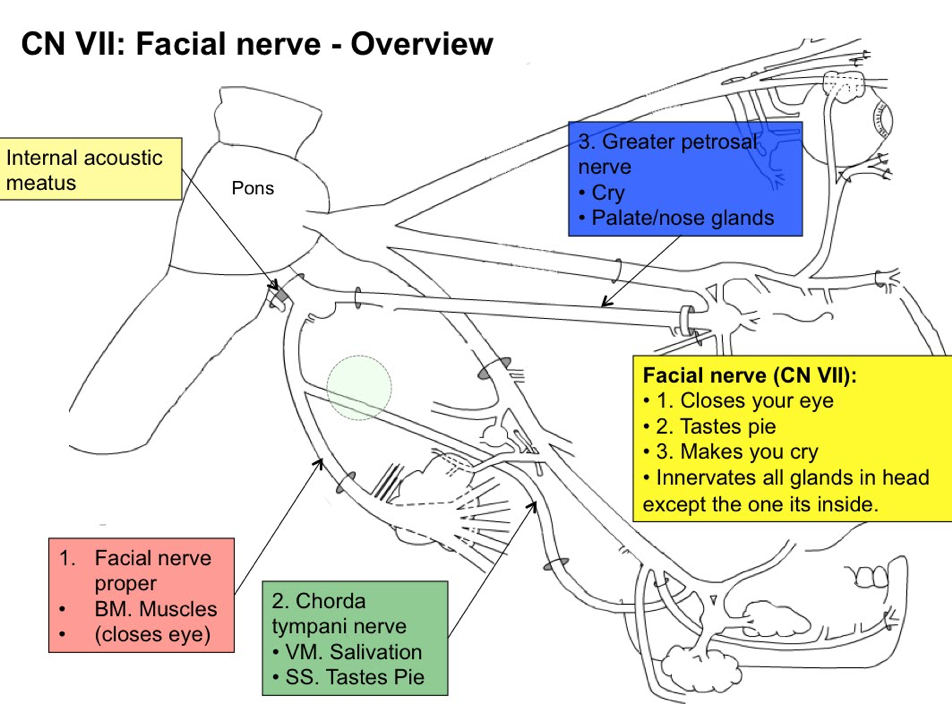
Cranial Nerve VII (the facial nerve) is a mixed nerve (having both sensory and motor function) with:
- Somatic afferents from the external auditory canal
- Afferent fibers from taste receptors from the anterior 2/3rds of the tongue
- Parasympathetic fibers innervating lacrimal, submandibular, and sublingual salivary glands
- Motor fibers innervating the facial muscles

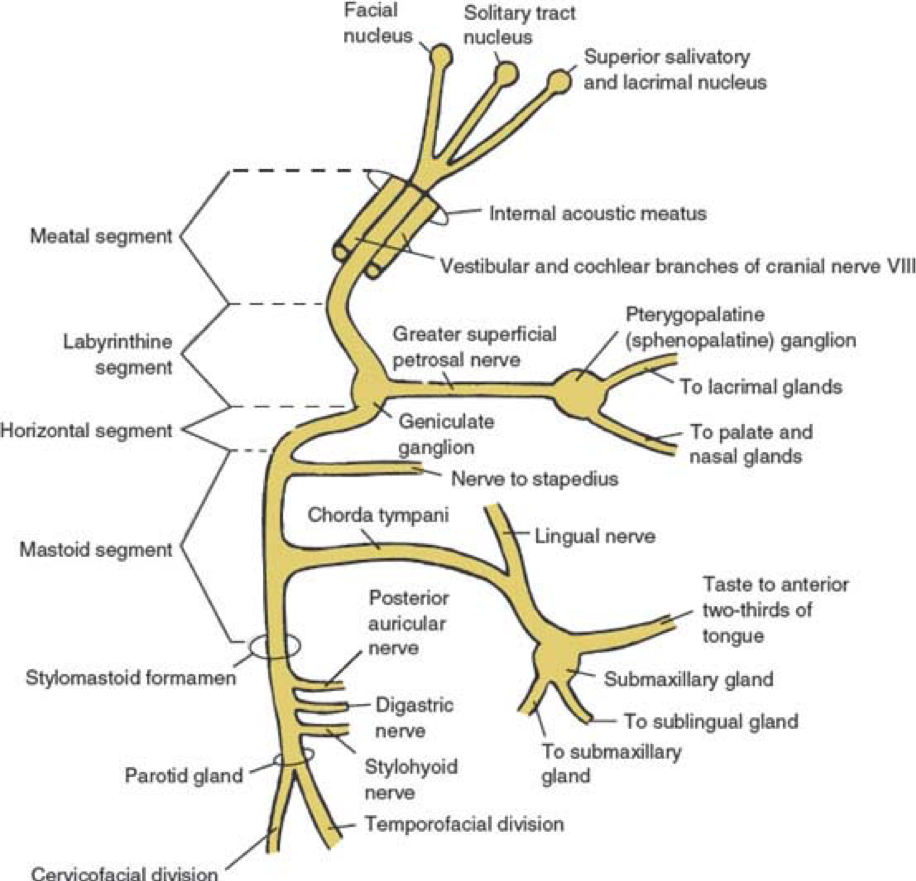
There are six (6) segments of the nerve after it emerges from the pons of the brainstem:
- Intracranial (cisternal)
- Meatal (from brainstem to internal auditory canal)
- Labyrinthine (internal auditory canal to geniculate ganglion)
- Lacrimal gland, nasal/palate, pterygopalatine ganglion
- Tympanic (geniculate ganglion to pyramidal eminence)
- Stapedius nerve
- Mastoid (pyramidal eminence to stylomastoid foramen)
- Chorda tympani à tongue, salivary glands, lingual nerve
- Extratemporal (stylomastoid foramen to post parotid branches)
- 5 major facial branches
- Temporal
- Zygomatic
- Buccal
- Mandibular
- Cervical
- 5 major facial branches
Definition and Epidemiology
Bell’s Palsy is an acute peripheral nerve palsy of unknown etiology and makes up almost half of such cases. It is estimated that the annual incidence is around 20 patient per 100,000 population. There is no race, geographic, or gender correlation., though there is some old data on increased risk during 3rd trimester of pregnancy.
Pathogenesis
Had been hotly debated for many years as to the cause of this condition and is generally considered to be caused by Herpes Simplex virus due to associated serologic evidence in effected patients. Newer data has been published, but is not entirely conclusive. Most agree that is due to some viral pathogen with herpes being the most common, but also implicating CMV, EBV, adenovirus, and coxsackievirus. Specifically, the signs and symptoms are a result of viral mediated inflammatory demyelination of the nerve.
Signs and Symptoms
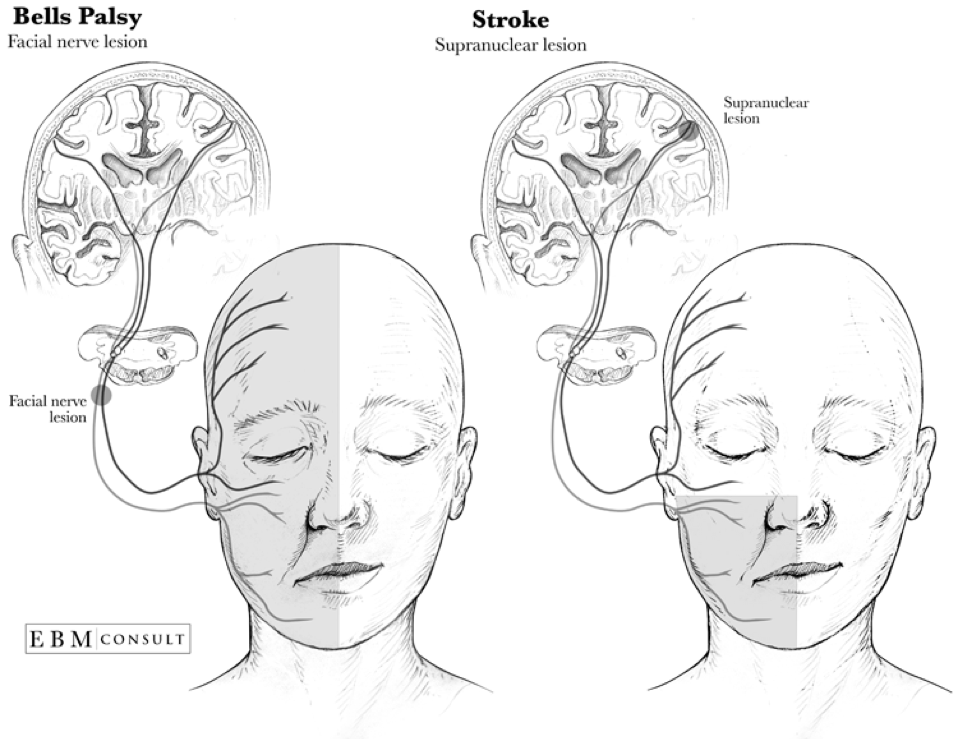
Most common presentation is acute (over several hours) unilateral facial paralysis with:
- Motor
- Inability to close the eye
- Eyebrow sagging with inability to wrinkle the forehead
- Obliteration of the nasolabial fold
- Dropping of the affected corner of the mouth
- Sensory
- Hyperacusis
- Loss of taste on the anterior 2/3rd of tongue
Symptoms are progressive and usually reach peak involvement within 3 weeks of onset. Patients should begin to have return of function within 2-4 months.

Diagnostic Studies
Bell’s palsy is a clinical diagnosis and diagnostic studies are generally not indicated unless the presentation is atypical, still progressing at 3 weeks, or there is no return of function by 4 months. History of facial twitching or spasms preceding the paralysis raises suspicion of compressive neuropathy from tumor or mass.
- Electromyography (EMG)
- The most simplest of the electrodiagnostic tests that can be used to show action potentials on active volition. Some degree of potential infers that the nerve is still intact and therefor, can improve.
- Nerve Conduction Studies (NCS)
- Supramaximal stimulation near the parotid gland with measured evoked potentials over the orbicularis oculi, nasalis, and lower facial muscles can measure the degree of axonal loss. Studies have shown >75% is the critical cutoff for low likelihood of full recovery. Ideally, this should be performed within 2 weeks of symptom onset for a more accurate prognosis.
- Facial Nerve Stimulation
- Should be considered with 2 weeks of symptoms onset if surgical decompression is considered due to potential for reversibility.
- Needle EMG
- Utilized after 3 weeks to assess the degree of axonal damage and evidence of subclinical reinnervation for recovery
- Imaging
- High-resolution, contrast-enhanced CT (for bony pathology) or gadolinium-enhanced MRI (for soft tissue structures) of the brain, temporal bone, and parotid gland.
- Lyme serology should be entertained in patients from endemic regions.
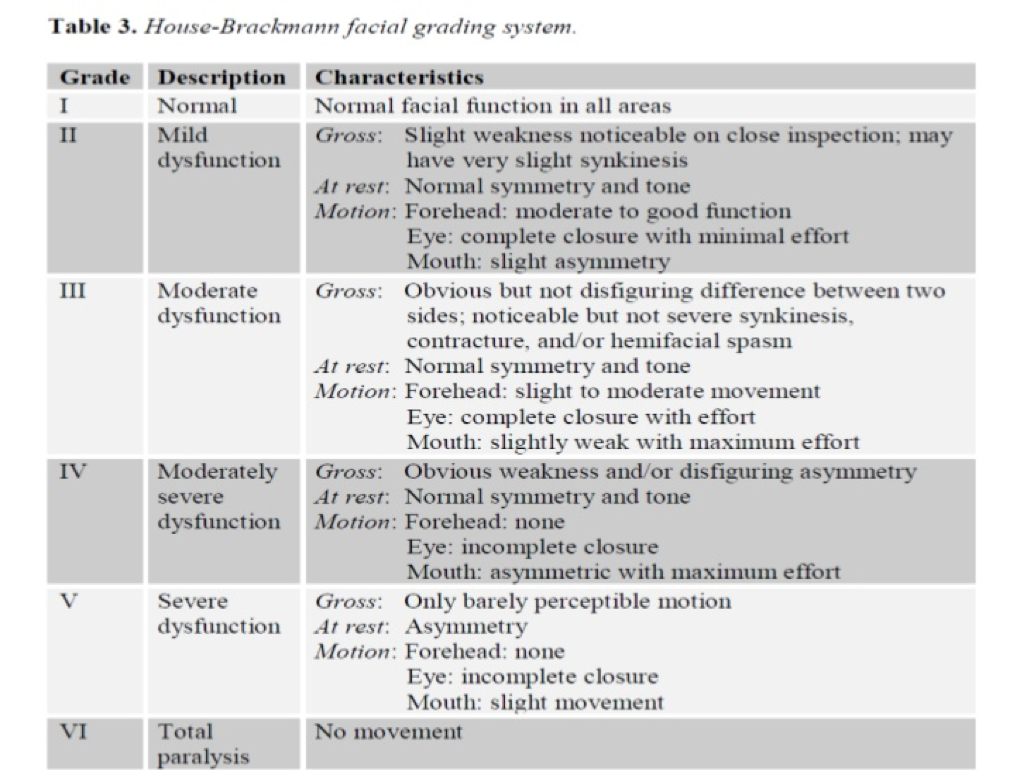
Severity Grading
The House-Brackman scale is the most common grading scale that uses objective criteria to score the severity, mark progression, and track return of function.
Treatment
Mainstay of therapy for Bell’s palsy is corticosteroids (for the inflammation) and antivirals (for the viral pathogens). Current recommendations are:
- Prednisone 60-80mg daily for 7 days
- Valacyclovir 1000mg TID for 7 days
- Within 72 hours of symptoms onset
Eye care should include artificial tears and an eye patch for sleeping.
Prognosis
Favorable prognosis if any recovery is seen within 21 days of symptom onset with data showing 71% with complete resolution, 13% with slight residual sequelae, and 16% with residual weakness, synkinesis, or contracture. 94% of patients with incomplete involvement have full resolution, while only 60% of complete involvement returned to normal function.
References
- Monkhouse WS. The anatomy of the facial nerve. Ear, nose, & throat journal. 1990; 69(10):677-83, 686-7. [pubmed]
- May M, Klein SR. Differential diagnosis of facial nerve palsy. Otolaryngologic clinics of North America. 1991; 24(3):613-45. [pubmed]
- Hilsinger RL, Adour KK, Doty HE. Idiopathic facial paralysis, pregnancy, and the menstrual cycle. The Annals of otology, rhinology, and laryngology. ; 84(4 Pt 1):433-42. [pubmed]
- Peitersen E. Bell’s palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta oto-laryngologica. Supplementum. 2002; [pubmed]
- Schirm J, Mulkens PS. Bell’s palsy and herpes simplex virus. APMIS : acta pathologica, microbiologica, et immunologica Scandinavica. 1997; 105(11):815-23. [pubmed]
- Kennedy PG. Herpes simplex virus type 1 and Bell’s palsy-a current assessment of the controversy. Journal of neurovirology. 2010; 16(1):1-5. [pubmed]
- Morgan M, Nathwani D. Facial palsy and infection: the unfolding story. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 1992; 14(1):263-71. [pubmed]
- Liston SL, Kleid MS. Histopathology of Bell’s palsy. The Laryngoscope. 1989; 99(1):23-6. [pubmed]
- Valls-Solé J. Electrodiagnostic studies of the facial nerve in peripheral facial palsy and hemifacial spasm. Muscle & nerve. 2007; 36(1):14-20. [pubmed]
- May M, Klein SR, Taylor FH. Indications for surgery for Bell’s palsy. The American journal of otology. 1984; 5(6):503-12. [pubmed]
- Gilden DH. Clinical practice. Bell’s Palsy. The New England journal of medicine. 2004; 351(13):1323-31. [pubmed]
- House JW, Brackmann DE. Facial nerve grading system. Otolaryngology–head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 1985; 93(2):146-7. [pubmed]
- Gronseth GS, Paduga R, . Evidence-based guideline update: steroids and antivirals for Bell palsy: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2012; 79(22):2209-13. [pubmed]
- Baugh RF, Basura GJ, Ishii LE, et al. Clinical practice guideline: Bell’s palsy. Otolaryngology–head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2013; 149(3 Suppl):S1-27. [pubmed]
- Schwartz SR, Jones SL, Getchius TS, Gronseth GS. Reconciling the clinical practice guidelines on Bell’s palsy from the AAO-HNSF and the AAN. Otolaryngology–head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2014; 150(5):709-11. [pubmed]
- de Almeida JR, Guyatt GH, Sud S, et al. Management of Bell palsy: clinical practice guideline. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne. 2014; 186(12):917-22. [pubmed]
- Peitersen E. The natural history of Bell’s palsy. The American journal of otology. 1982; 4(2):107-11. [pubmed]