***LISTEN TO THE PODCAST HERE***
2015 American Academy of Pediatrics Schedule for Preventive Pediatric Health

2018 Centers for Disease Control Immunization Schedule

Denver Developmental Milestones

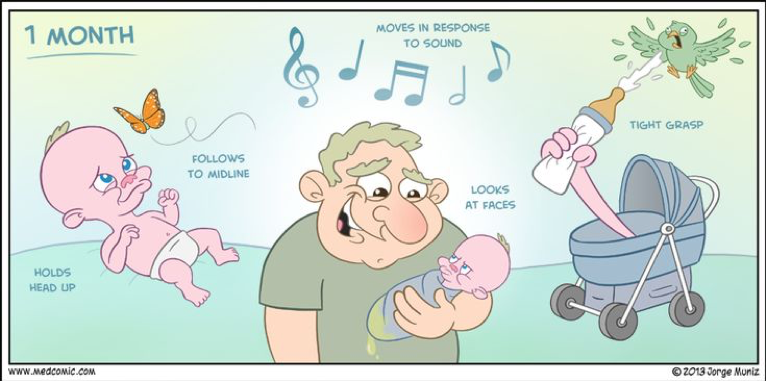
Initial Office Visit (within 2 weeks)
Development
- Rooting and suckling reflex strong
- Indiscriminate tight grasp of hands
- Responds to light, noise, and movement
- Lift head from supine
- Follow to midline
- Regained birthweight
Anticipatory Guidance
- Feeding
- Encourage breastfeeding and its benefits:
- Decreased risk of infections
- Decreased SIDS risk
- Decreased obesity risk
- Increases emotional connection
- Frequency
- On-demand, but generally every 2-4 hours
- Amount
- 1 oz/kg/day
- Reflux
- Encourage breastfeeding and its benefits:
- Sleeping
- Back to sleep
- Fever
- Jaundice
Vaccinations
- Hepatitis B #1 (if not given in hospital)
2 Month Visit
Development
- Smile socially and start cooing
- Lift head from prone
- Turns head towards sounds and follow past midline
- Push up on arms from prone
- Recognize parents

Anticipatory Guidance
- Feedings
- Start to delay middle of the night feedings
- Sleep
- Move to another room to help with self-soothing
Vaccinations
- Hepatitis B #2
- Rotavirus #1
- DTaP #1
- HIB #1
- Pneumococcal #1
- Polio #1
4 Month Visit
Development
- Neonatal reflexes will begin to disappear
- Smiles spontaneously
- Likes to play/interact with people
- Begins to babble
- Different cries for different complaints
- Reach with one hand
- Uses hands and eyes together
- Hold head unsupported and support on forearms when prone
- Start rolling over prone to supine
- Brings hands to mouth


Anticipatory Guidance
- Feeding
- 32oz/day = max
- 4-5 feedings per day
- Start to introduce rice cereal and solid foods
- Counsel that stools will change
- One food at a time
- Sleeping
- May start to sleep through the night
- Counsel to start a bedtime routine
- No more middle of night feedings
- May start to sleep through the night
Vaccinations
- Rotavirus #2
- DTaP #2
- HIB #2
- Pneumococcal #2
- Polio #2
6 Month Visit
Development
- Doubled birth weight
- Stranger danger
- Likes to look at self in the mirror
- Responds to name
- Imitate speech
- Voice happy and displeasure
- Pass objects from hand to hand
- Rollover in both directions
- Sits unsupported

Anticipatory Guidance
- Feeding
- Increase solid foods and decrease formula
- Introduce sippy cup
- Sleeping
- Separation anxiety common
Vaccinations
- Rotavirus #3 (if indicated)
- DTaP #3
- HIB #3 (if indicated)
- Pneumococcal #3
- Polio #3
- Hepatitis B #3
- Influenza #1
- Fluoride (if needed)
9 Month Visit
Development
- Crawls
- Understands “no”
- Starts saying “mama” and “dada” indiscriminently
- Takes 9 months to be a “mama”
- Can point
- Immature pincer grasp
- Pull to stand and cruise
- Wave “bye-bye”
- Object permanence begins to develop
Anticipatory Guidance
- Feedings
- Milk/formula down to 24oz/day
- Solid foods at meal time
- Introduction of finger foods
- Sleep
- Should be through the night
- Limit naps to 2x/day
- Introduce brushing as teeth should begin erupting
- Discipline plans
Vaccinations
- Catch-up (if needed)
- Influenza #2
12 Month Visit
Development
- Begin walking unsupported
- Increased vocabulary
- Follow simple, one-step commands
- Imitates actions and words
- Help with dressing
Anticipatory Guidance
- Feeding
- Introduce cow’s milk not to exceed 24oz/day
- Ween from bottle
- Juice not to exceed 8oz/day
- Sleep
- Bedtime ritual is important
- Discipline and Behavior Counseling
- Set limits and be consistent
- Can transition to forward facing car seat with harness if they exceed current manufacturers height/weight recommendations
- Routine CBC for anemia screening
Vaccinations
- HIB #3 or #4
- Pneumococcal #4
- MMR #1
- Varicella #1
- Hepatitis A #1
15 Month Visit
Development
- Kick and roll ball
- Can undress themselves
- Play hide and seek
- Attempts to name objects
- Vocabulary up to 5 words
- Build towers
- Needs social interaction
- Thought they don’t play well with others (sharing)
Anticipatory Guidance
- Feeding
- 3 balanced meals per day with 1-2 snacks
- Introduce utensils
- Sleeping
- Down to 1 nap per day
- Temper tantrums will be more common
- Have crib on lowest rung
- Child stays in room for bedtime
- Discipline and Behavior
- Praise for good behavior and redirect bad
Vaccinations
- DTaP #4
- HIB #4 (if indicated)
- Hepatitis A #2
18 month Visit
Development
- Plays simple pretend
- Likes to explore, but needs parent close
- Name body parts
- Scribbles on their own
- Climb stairs
- Turn pages in books while reading
- Put simple puzzles together
Anticipatory Guidance
- Feedings
- Drinking from cup exclusively and using utensils
- Decrease milk to 16oz/day
- Discipline and Behavior
- Introduce “timeouts” for discipline
Vaccinations
- Catch-up (if needed)
2 year Visit
Development
- Gets excited and enjoys playing with others
- Use two word sentences
- Knows names of familiar people
- Shows defiant behavior (Terrible Two’s)
- Increase autonomy and self-expression
- Echolalia
- Begins to sort colors and shapes
- Follow two-step commands
- Build towers of 4-6 blocks
- Start running
- Throw and kick balls
- Walk up and down stairs
- Vocab up to 50 words and use two-word sentences
Anticipatory Guidance
- Growth
- 2-3 inches and 3-6 pounds for the year
- Transition to toddler bed
- Naps down to 1 a day
- Begin potty training
- Safety
- House needs to be “babyproof” at this point
- Door latches, baby gates, outlet covers, cabinet locks
- House needs to be “babyproof” at this point
Vaccinations
- None
3 Year Visit
Development
- Pedal a tricycle
- 300 words in vocabulary
- Sort objects by color and shape
- Uses 3-5 word sentences
- Repeat their name, age, and gender
- Can play well with others (takes turns in games)
- Follow 2-3 step commands
- Copy a circle
- Alternate feet on stairs
Anticipatory Guidance
- Growth
- 2-3 inches and 3-6 pounds from previous visit
- Encourage autonomy and exploration with boundaries
Vaccinations
- DTaP #5
- Polio #4
- MMR #2
- Varicella #2
4 Year Visit
Development
- Play “mom and dad”
- Play is more creative with make-believe
- Tell stories and ask questions
- Sing songs
- Play board games
- Copy and recognize letters
- Uses scissors
- Understand the concept of counting
- Copy a square (4 sides)
- Speak in 4-5 word sentences
- Increased emotional range and understands them
Anticipatory Guidance
- Growth
- 40 inches and 40 lbs at 4 years
- Thrive on praise
- Be consistent and balanced in discipline
Vaccinations
- None
5 Year Visit
Development
- Wants to be with and like friends
- Follows rules more
- Use future tense
- Use full sentences
- Fully aware of gender
- Fully potty trained
- Likes to sing, dance, and act
- Count 10 objects correctly
- Stand on one-leg for 10 seconds or longer
- Draw a person with body parts
- Can tell difference between real and make-believe
Anticipatory Guidance
- Sibling jealously is common
- Prepare for kindergarten
- Start instilling morality in decision making
- TV Guidelines
- 1 hour per day max
- Don’t use as a reward
- Talk with other adults in house on plan
References
- 2015 Recommendations for Preventive Pediatric Health Care. Pediatrics. 2015;136(3):e727-e729 [link]
- 2018 CDC Immunization Schedule for Children and Adolescents 18 years or younger. [link]
- CDC – Developmental Milestones [link]
- Scharf RJ, Scharf GJ, Stroustrup A. Developmental Milestones. Pediatrics in review. 2016; 37(1):25-37; quiz 38, 47. [pubmed]