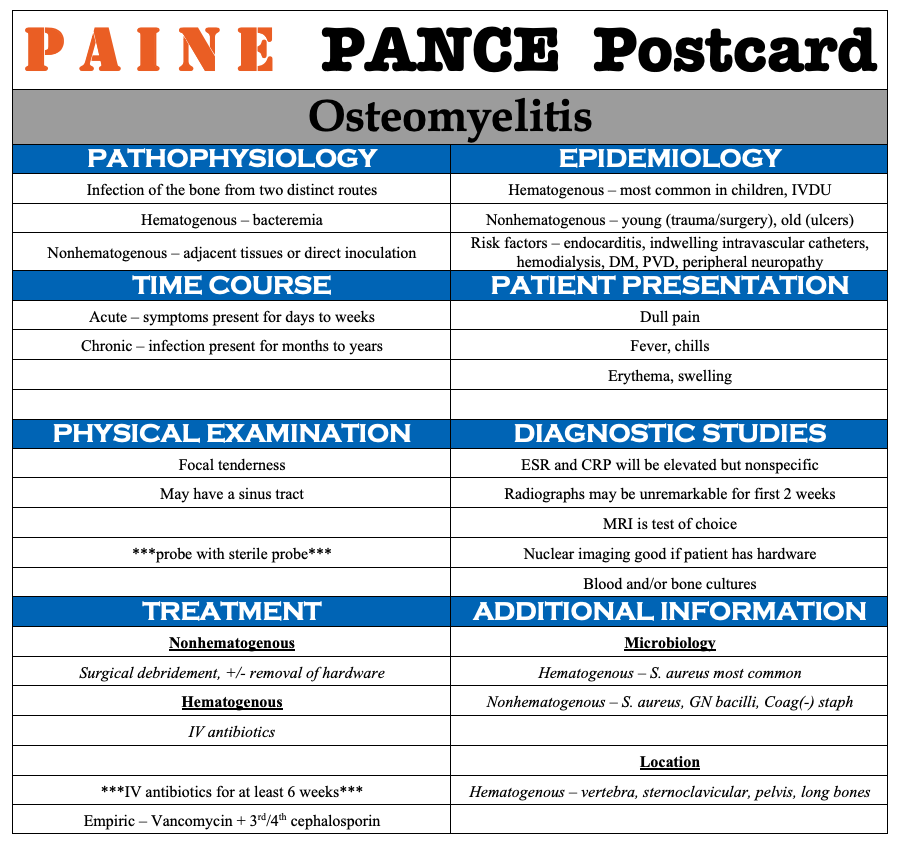
PAINE PANCE Postcard – Osteomyelitis Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
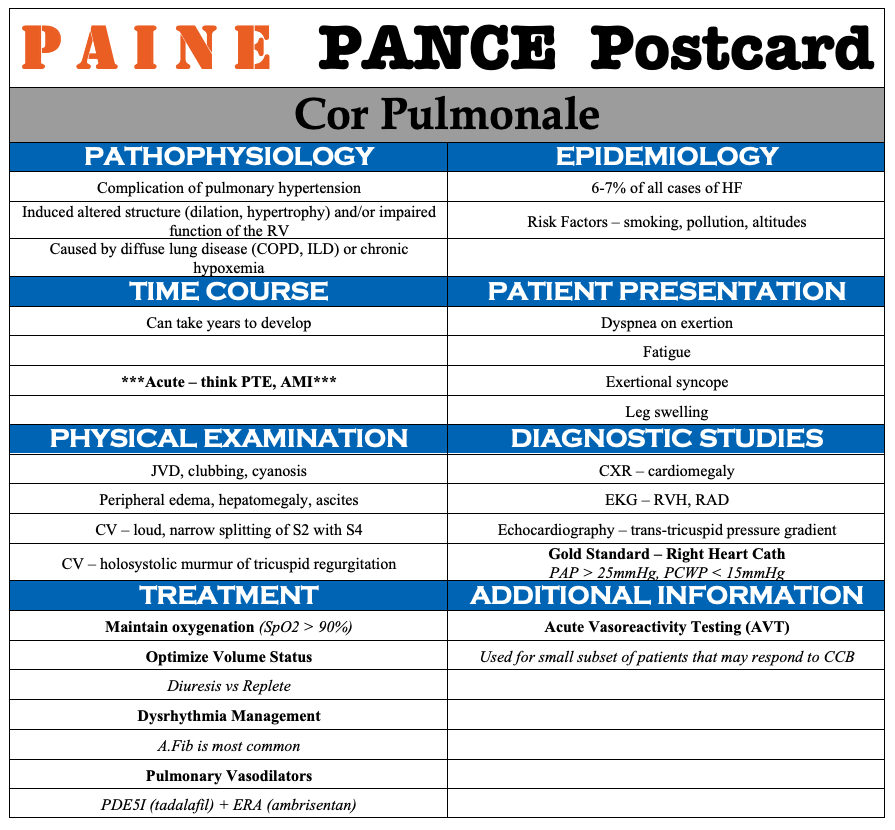
PAINE PANCE Postcard – Cor Pulmonale Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
PAINE PANCE Postcard – Tuberculosis Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE *** EpPAINEnym – Ghon Complex
PAINE PANCE Postcard – Hiatal Hernia Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
PAINE PANCE Postcard – Generalized Anxiety Disorder Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***
PAINE PANCE Postcard – Huntington Disease Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE *** EpPAINEnym – Huntington Disease
PAINE PANCE Postcard – Guillain-Barré Syndrome Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE *** Deep Dive – #71 – Guillain-Barré Syndrome
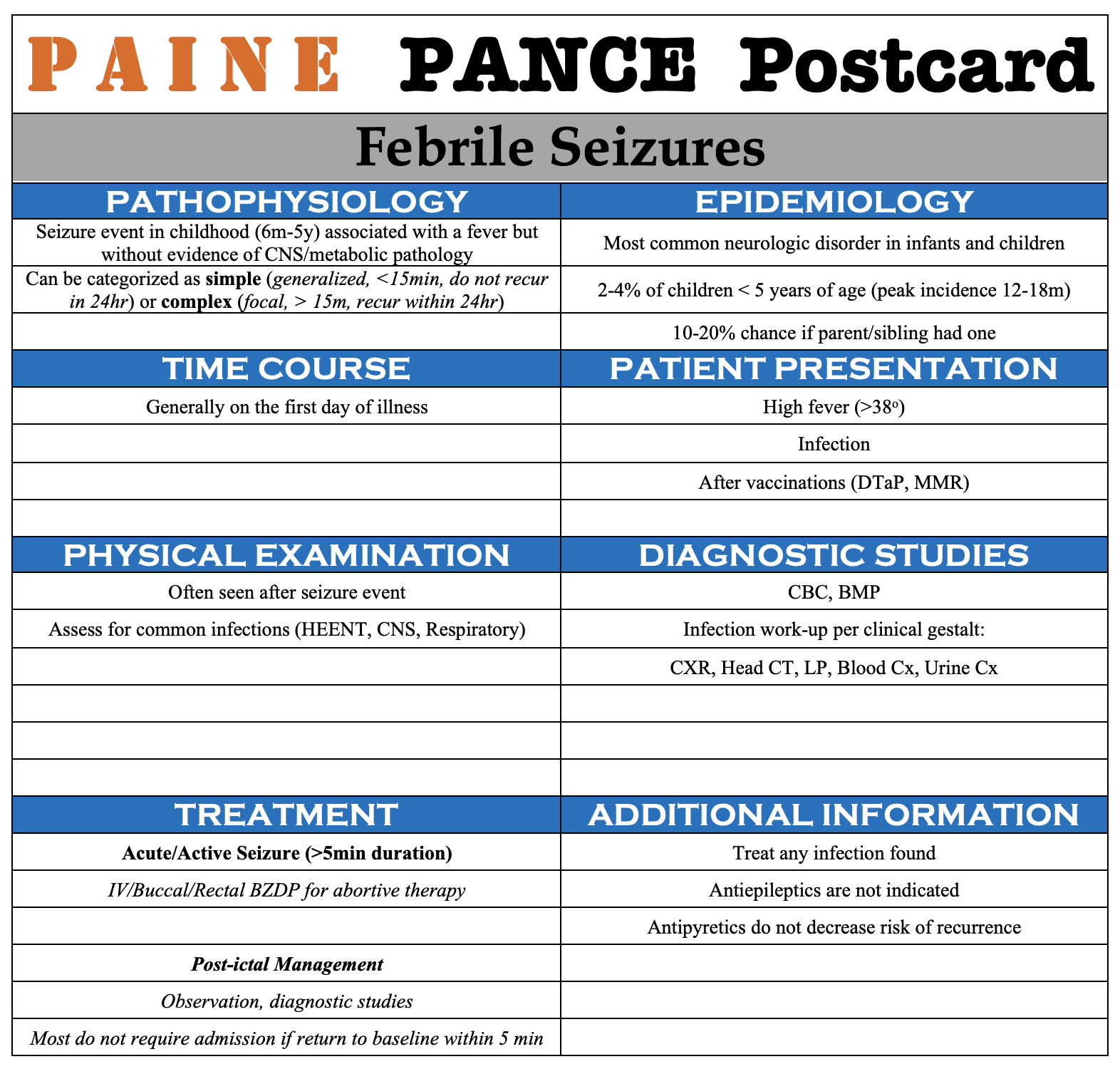
PAINE PANCE Postcard – Febrile Seizures Posted by Kristopher Maday PA-C 0 *** LISTEN TO THE PODCAST HERE ***