History of FIGO
Because of confusing terminology and difficulty in translating to other languages, the International Federation of Obstetrics and Gynecology (FIGO) created a special task force in 2005 charged with clarifying the terminology and classifying the different causes. This way clinicians, patients, and researchers throughout the world could be talking the same language. Dysfunctional uterine bleeding (DUB) was replaced by abnormal uterine bleeding (AUB).. They also introduced a classification system to help sub-divide the causes of AUB.
But in order to define something as “abnormal”, they needed to define normality, which can obviously be very difficult when incorporating the world’s population. The consensus definitions were then agreed upon in 2015 to include the 5th to 95th percentiles form the available data.
The FIGO definition of AUB is any symptomatic variation from normal menstruation, with regards to frequency, regularity, duration, or volume.

Classifications of Abnormal Uterine Bleeding
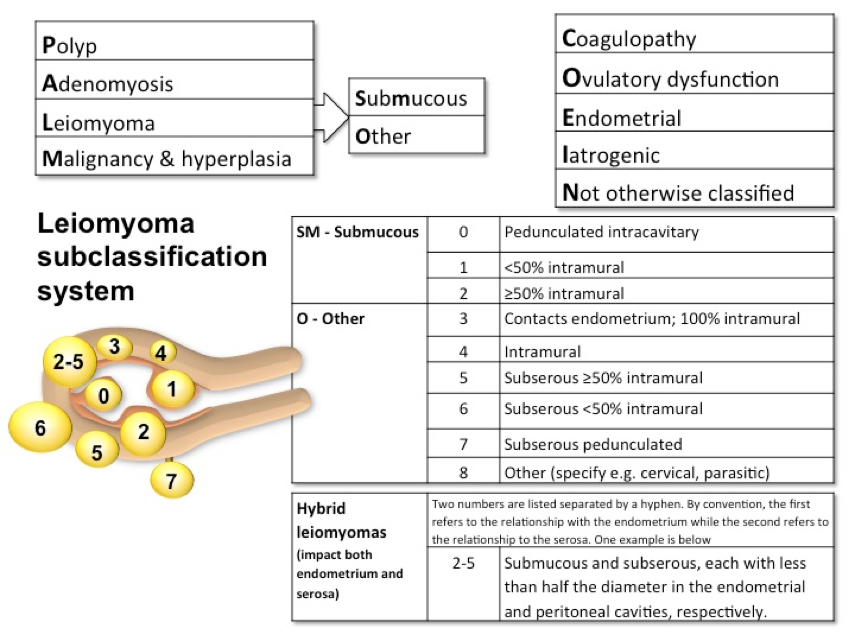
In 2011, FIGO created a classification system for the main causes of AUB. It is broken down into 2 main categories based on whether or not the pathology can be seen on imaging or histopathology. This also allows for subclassifications due to multiple etiologies.
- Structural (PALM)
- Polyps (AUB-P)
- Adenomyosis (AUB-A)
- Leiomyomas (AUB-L)
- Hierarchy of classification
- Primary
- Secondary
- Submucosal
- Abuts the endometrium or distorts the endometrial cavity
- Other
- Tertiary
- 0-8 numbering system based on endometrial or serosal involvement
- Hybrid (2-5)
- Submucosal and subserosal
- Malignancy and hyperplasia (AUB-M)
- Non-structural (COEIN)
- Coagulopathy (AUB-C)
- Most commonly is von Willebrand disease
- Ovulatory dysfunction (AUB-O)
- At least one cycle that varies by more than 7 days in 12 months
- Endometrial (AUB-E)
- Iatrogenic (AUB-I)
- Medications
- Anticoagulants
- Hormone therapies
- IUDs
- Not otherwise classified (AUB-N)

Documentation
Very similar to the documentation for an OB patient (TPAL score), the documentation uses the PALM-COEIN scoring system for “simplicity”. Example:
- Patient with adenomyosis would be:
- Patient with endometrial hyperplasia and a subserosal leiomyoma < 50% intramural would be:
References
- Fraser IS, Critchley HO, Munro MG, Broder M, . A process designed to lead to international agreement on terminologies and definitions used to describe abnormalities of menstrual bleeding. Fertility and Sterility. 2007; 87(3):466-76. [pubmed]
- Woolcock JG, Critchley HO, Munro MG, Broder MS, Fraser IS. Review of the confusion in current and historical terminology and definitions for disturbances of menstrual bleeding. Fertility and Sterility. 2008;90(6):2269-80. [pubmed]
- Fraser IS, Critchley HO, Munro MG, Broder M. Can we achieve international agreement on terminologies and definitions used to describe abnormalities of menstrual bleeding? Human reproduction (Oxford, England). 2007;22(3):635-43. [pubmed]
- Harlow SD, Lin X, Ho MJ. Analysis of menstrual diary data across the reproductive life span applicability of the bipartite model approach and the importance of within-woman variance. Journal of clinical epidemiology. 2000;53(7):722-33. [pubmed]
- Fraser IS, Critchley HO, Broder M, Munro MG. The FIGO recommendations on terminologies and definitions for normal and abnormal uterine bleeding. Seminars in reproductive medicine. 2011;29(5):383-90. [pubmed]
- Munro MG, Critchley HO, Broder MS, Fraser IS, . FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2011;113(1):3-13. [pubmed]