


Other Known Aliases – Palm Sign, Cossio’s Sign, Cossio-Levine’s Sign
Definition – Clenched fist held over the sternum while a patient is describing their chest pain and classically is the right hand, as cardiac pain can refer to the left arm.

Clinical Significance – There is very little significance to this sign and has been studied to only have a 14% sensitivity for cardiac chest pain, but is a classic physical exam finding and frequent pimp fodder.
History – Named after Samuel Albert Levine (1891-1966), who was an American cardiologist and attending physician at The Brigham Hospital in Boston, MA, and assistant professor of medicine at Harvard University. He graduated Harvard at the age of 20 and was the first physician to diagnose President Franklin Roosevelt with poliomyelitis. He was a pioneer in coronary thrombosis research and was the second physician to ever diagnose the condition, which he described it in his classic book Clinical Heart Disease in 1936.

He is also the namesake of The Levine Scale, a 1 to 6 grading system to characterize the intensity of heart murmurs, and Lown-Ganong-Levine syndrome, which is a pre-excitation syndrome causing a shortened PR interval with normal QRS complexes in tachycardia.

The Levine Scale

Lown-Ganong-Levine Syndrome
References
What are some of the chest scores we use to evaluate the likelihood a patient with chest pain is having ACS?

What are the 5 main life-threatening causes of chest pain?

The 5 main life-threatening causes of chest pain you should ALWAYS think of are:

There are a few others that should also cross your mind:
References
82-year-old male, with a history of HTN, HLD, and CAD, presents to your clinic with a six-month history of dyspnea on exertion. He states he is unable to walk as far as he used when exercising, and when he over exerts himself, he reports having some mild chest pain and feeling lightheaded. This resolves with rest and he denies any syncope with these events.
Medications
Metoprolol 50mg daily
Lisinopril 10mg daily
Simvastatin 30mg daily
Vital Signs
BP – 158/97
HR – 62
RR – 13
O2% – 100%
Physical exam
General – WN/WD male in NAD
Pulmonary – CTA without adventitial breath sounds
CV – Soft S2 with murmur over right 2nd intercostal space
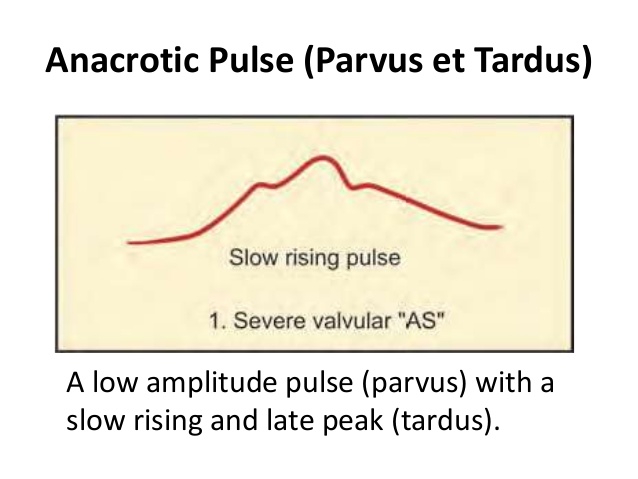
PV – carotid pulse is weak and has a slow rise, murmur is appreciated
Neuro – No focal deficits
EKG

This patient has aortic stenosis. The suggestive parts of the H&P are:


These variables will help with staging the severity of the stenosis, as well as determine need for operative intervention.
Other known aliases – Atrial Reflex
Definition – Compensatory increase in heart rate caused by a rise in right atrial pressure. Opposite of carotid baroreceptors.
Clinical Significance – Respiratory sinus arrythmia. Inspiration causes increased venous return.
History – Described by Francis Arthur Bainbridge in 1915
References
82-year-old male, with a history of HTN, HLD, and CAD, presents to your clinic with a six-month history of dyspnea on exertion. He states he is unable to walk as far as he used when exercising, and when he over exerts himself, he reports having some mild chest pain and feeling lightheaded. This resolves with rest and he denies any syncope with these events.
Medications
Metoprolol 50mg daily
Lisinopril 10mg daily
Simvastatin 30mg daily
Vital Signs
BP – 158/97
HR – 62
RR – 13
O2% – 100%
Physical exam
General – WN/WD male in NAD
Pulmonary – CTA without adventitial breath sounds
CV – Soft S2 with murmur over right 2nd intercostal space
PV – carotid pulse is weak and has a slow rise, murmur is appreciated
Neuro – No focal deficits
EKG
Questions

Anatomy
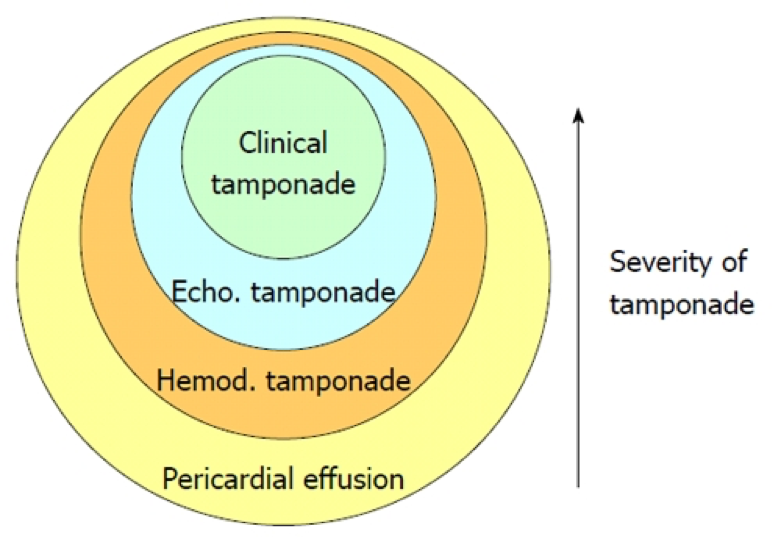
The pericardium consists of a double-layered semi-elastic sac that holds the heart in the mediastinum. Basically, so the heart doesn’t flop around inside the thoracic cavity. There should be a small amount of fluid (15-50mL) present to prevent adhesion of the pericardial sac to the heart. It is then termed an effusion when it is more than the normal amount. How much quantifies an effusion? Doesn’t matter…. what does matter is how fast that fluid develops. Because the pericardium is semi-elastic, it can accommodate and stretch over time if the accumulation is slow. This would lead to a greater volume of fluid before symptoms occur. If the fluid accumulates rapidly, less volume can produce profound effects due to the restrictive nature of the fibrous pericardium.

Etiology
Signs and Symptoms
There are no reliable historical clues or physical exam findings that are specific to pericardial effusions. They are helpful, though, to sort out the cause of the effusion. Common findings include:
Work-Up
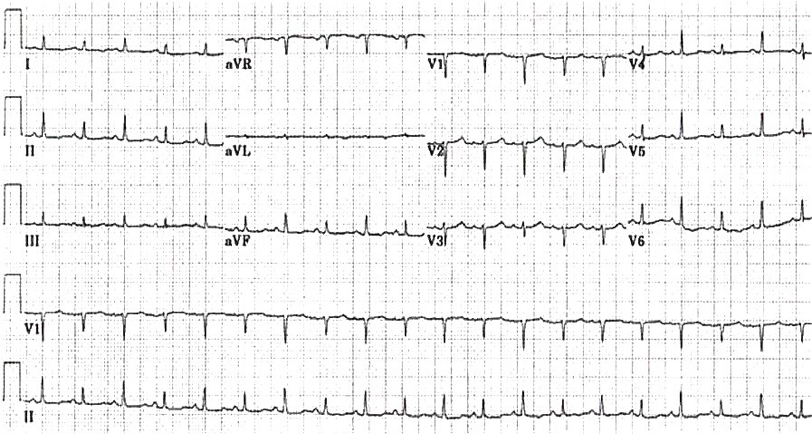
Life In The Fastlane – o http://lifeinthefastlane.com/ecg-library/basics/low-qrs-voltage/
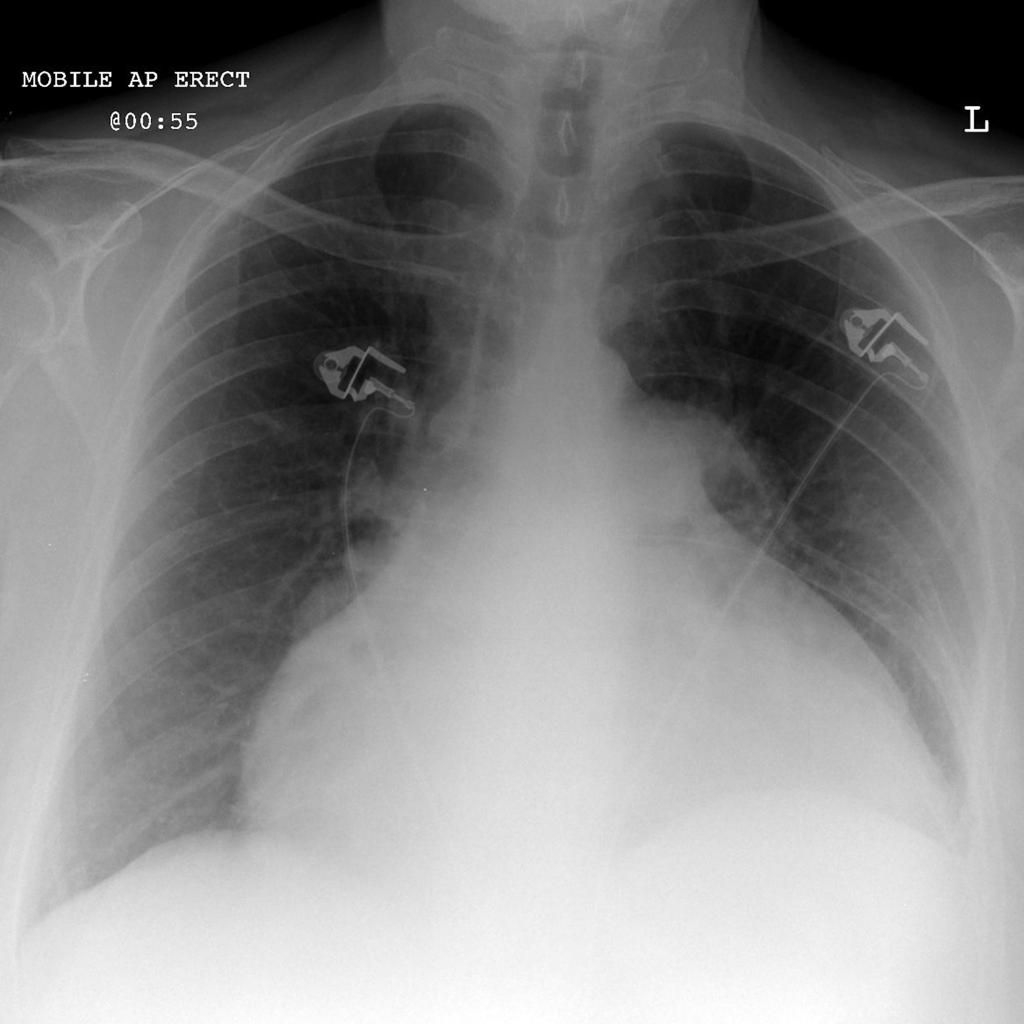
Radiopaedia

Treatment
References
Question
What are the 3 eponymous physical exam findings in patients with bacterial endocarditis and who were they named after?
Answers
Osler Nodes

Janeway Lesions

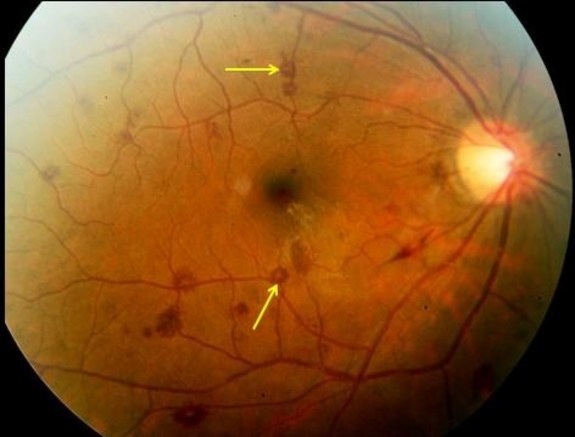
Roth Spots
References
Happy 2017!!! I apologize for the delay in having the pearls coming out, but life is life. So here you go:
What are the 3 eponymous physical exam findings in patients with bacterial endocarditis and who were they named after?

