Other Known Aliases – superficial fascia of abdominal wall
Definition – The fatty outer layer of the superficial abdominal fascia and is continuous with the superficial fascia of the thigh.
Clinical Significance – This is one of the classic nine abdominal layers you cut through when performing open abdominal procedures and is a favorite pimp question among general surgeons.
History – Named after Petrus Camper (1722-1789), who was a Dutch physician and anatomist, and received both a PhD and medical doctorate from the University of Leiden in 1746 at the age of 24. He spent many years as a traveling doctor throughout Europe. He subsequently held positions as professorships of surgery and philosophy at Franeker University and University of Amsterdam. He was a scholar and gentleman throughout his illustrious career and made tremendous strides in the fields of human and veterinary medicine, anthropology,and the arts.
Camper’s Anatomy Lesson (1758)
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Other Known Aliases – gastroduodenostomy and gastrojejunostomy
Definition – In a Billroth I procedure, the distal stomach is removed and the distal stomach is connected with a end-to-end anastomosis to the duodenum. In a Billroth II procedure, the distal stomach is removed and connected with a side-to-side anastomosis to the jejunum.
Clinical Significance – Both of these procedures are used in distal gastric pathologies, including gastric cancer, recurrent peptic ulcer disease, large duodenal perforations, bleeding gastric ulcer, gastrointestinal stromal tumors, or corrosive stricture of the stomach. A Billroth I is generally preferred as it has less complications and restores normal GI continuity. A Billroth II is used to prevent undue tension on the anastomosis secondary to scarring.
History – Named after Christian Albert Theodor Billroth (1829-1894), who was an Austrian surgeon and generally regarded as the founding father of modern abdominal surgery. He received his medical doctorate from the Frederick William University of Berlin in 1852. His medical career was almost completely abandoned due to his love of music and was a close friend of Johannes Brahms. He became the Chair of Clinical Surgery at the University of Zurich in 1860. He was well known as a charismatic and infectious instructor, attracting students throughout Germany. It was at this post that he published is classic textbook Die allgemeine chirurgische Pathologie und Therapie (General Surgical Pathology and Therapy) in 1863. He was directly responsible for several landmark historical surgeries including:
1872 – first to perform an esophagectomy
1873 – first to perform an laryngectomy
1876 – first to perform rectal cancer excision
1881 – first to perform antrectomy for gastric cancer
Other notable mentions for Dr. Billroth is his early adoption of the “white coat” and surgical cleanliness. He also was an advocate for prolonged surgical apprenticeships following completion of medical studies and was the precursor to William Halsted’s pioneering residency program at Johns Hopkins
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
1/3rd of these are
incisional and 2/3rd are primary
Anatomy
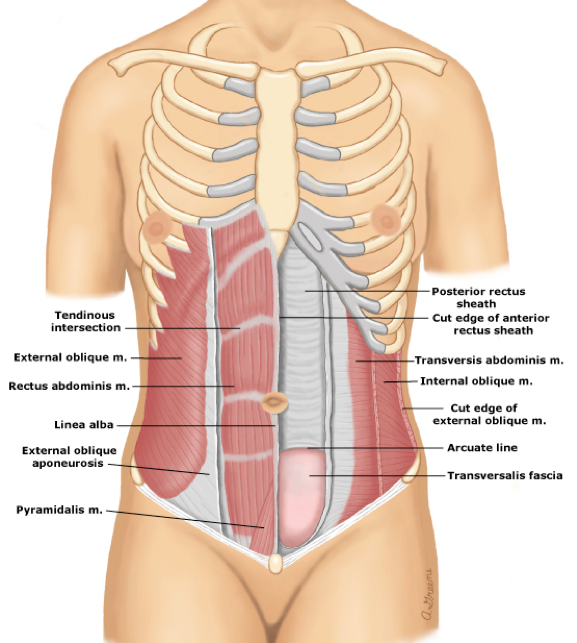
The abdominal wall is made up of multiple, overlapping muscles and connective tissue whose main purpose is to contain and protect the intra-abdominal organs, while also serving as accessary muscles of respiration and facilitating axial movements. The bony boundaries of the abdominal cavity are:
Xiphoid process superiorly and
costal margins laterally
With diaphragm separating the abdominal
cavity from thoracic cavity
Pubic symphysis inferiorly and iliac
crests laterally
With the inguinal ligament connecting
them
The lateral rectus abdominis muscles also fuse midline to
form the linea alba and laterally to the connect with the confluence of the
external oblique, internal oblique, and transverse abdominis muscles.
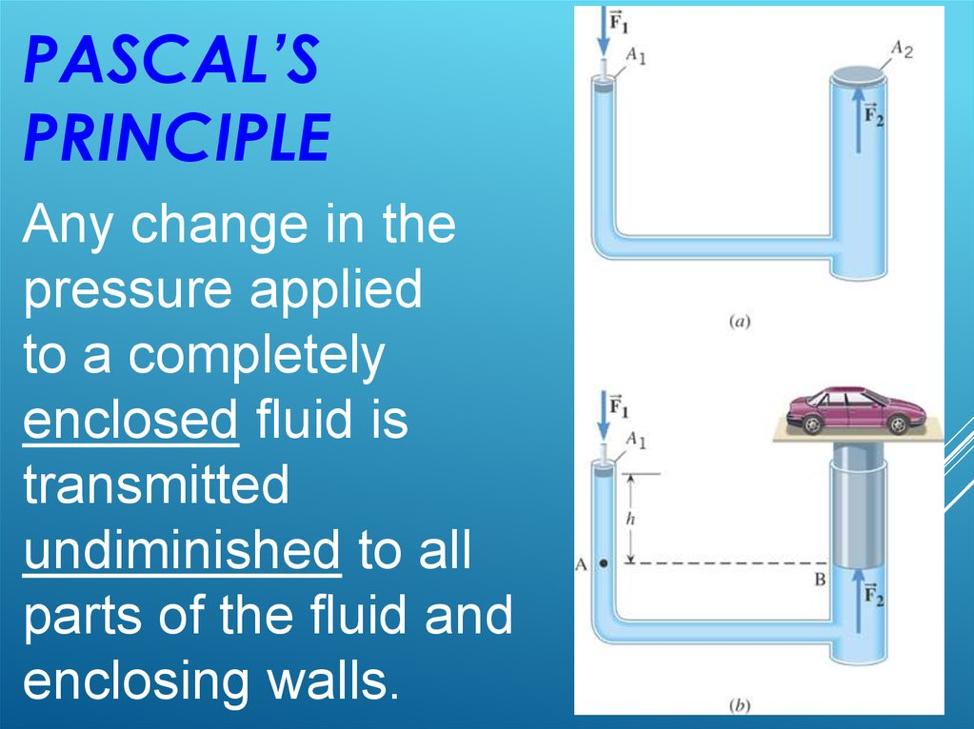
Weakness at any of these junctions (either anatomic or iatrogenic)
can allow herniation of abdominal contents through this defect. Pascal’s principle states that any pressure
generated within a closed system (abdominal cavity) is transmitted equally to
the walls of the system.
Classification and Definitions of Hernia Types
Ventral
Anterior
Epigastric
Occur between Xiphoid and umbilicus
Generally < 1cm in size
Umbilical
Most common overall and more common
in women
Spigelian
Occurs through aponeurosis of the
transverse abdominal muscle bounded by the linea semilunaris and lateral edge
of the rectus muscle medially
Incisional
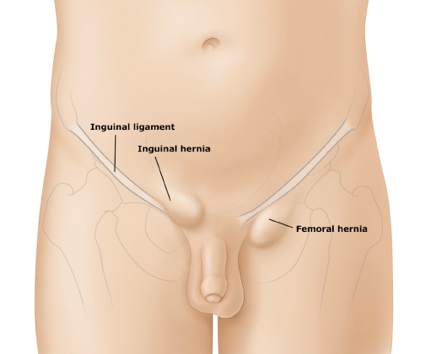
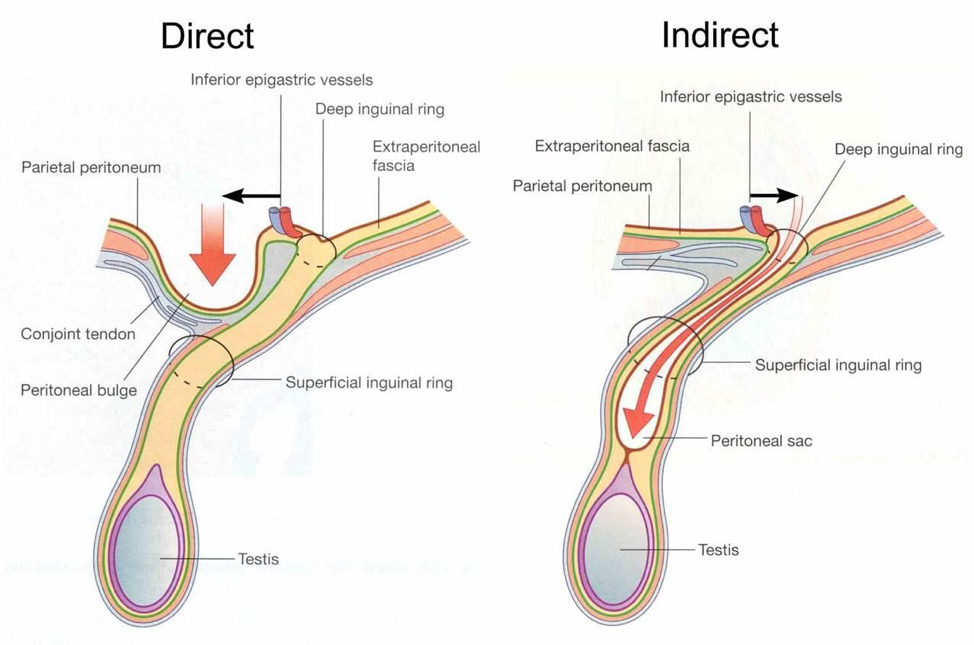
Groin
Inguinal
Direct
Weakness of posterior wall of the
inguinal canal inferior to the inferior vessels
Through the femoral ring into the
femoral canal posterior and inferior to the inguinal ligament
Signs and Symptoms
History
Can be asymptomatic if small
Most patients will feel a “bulge” and have varying degree of pain associated with this
Coughing, straining, or Valsalva worsen the pain or increase the size
Groin Hernias
Heaviness or dull discomfort in the groin
Pain improves when lying supine
Systemic symptoms (fever, nausea/vomiting, abdominal pain, bloating) should raise your suspicion of an incarcerated or strangulated hernia
Physical Examination
Abdominal wall should be examined with the patient standing and lying supine
Have patient bear down or cough to accentuate while palpating in the anatomic region
Examine for previous surgical incisions
Palpate around the umbilicus
In men, invaginate the scrotal skin to reach the inguinal canal
Femoral hernias most commonly occur medial to the femoral pulse
If any erythema or induration is visible, or if the bulge is tender to palpation, this should raise your suspicion of an incarcerated or strangulated hernia
Diagnosis
Most hernias in non-obese patients should be diagnosed by
careful and thorough history and physical examination. In others, radiographic investigation must be
performed.
Computed Tomography
Gold standard to identify sac,
contents, and surrounding edema or inflammation
Ultrasound
Can be very helpful if the diagnosis
of groin hernia is unclear
Most hernias will require surgical repair at some
point. The decision for operative
management comes down to risk of future complications, size, and symptom
tolerance. Patients with strangulation
or incarceration MUST emergent/urgent surgical repair to limit the risk of bowel
ischemia.
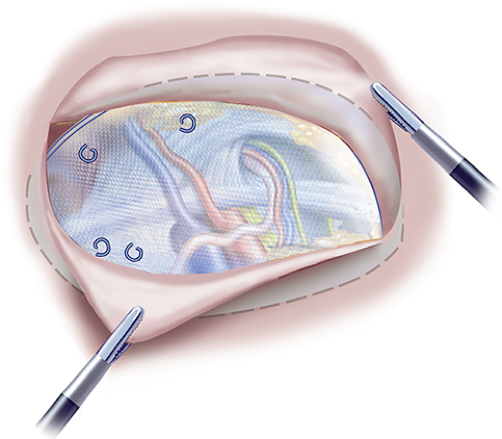
Surgeon preference and patient considerations dictate laparoscopic vs open hernia repair.
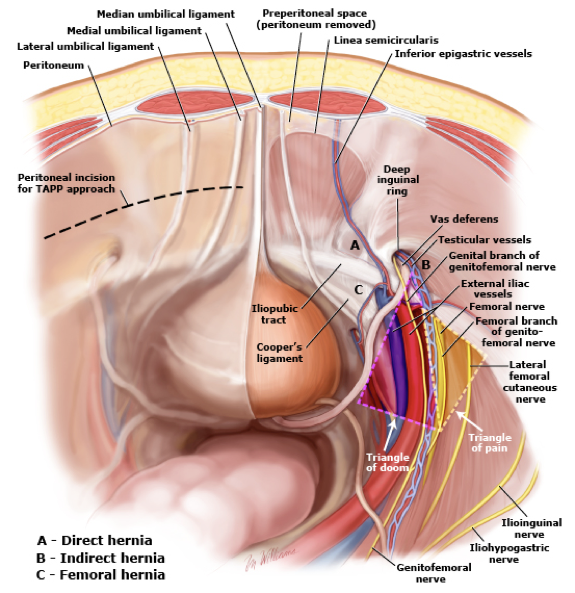
Avoids the peritoneal cavity by developing
a plane of dissection in the preperitoneal space
Landmarks for entry to the preperitoneal
space are:
Median umbilical ligament
Hernia defect
This space is entered by
establishing a plane between the posterior surface of the rectus muscle and
posterior rectus sheath and peritoneum
Transabdominal preperitoneal patch
(TAPP) repair
Advantage is that all three groin
hernia types are well visualized and in close proximity to each other
Surgical Repair for Ventral Hernias
Goals for repair
Prevent hernia recurrence
Low rate of surgical site infection
Provide dynamic muscle support
Provide a repair with physiologic tension
Prevent eventration or abdominal
wall bulging
Incorporate the abdominal wall
< 1cm
Open repair with or without mesh
directly over the defect
1-10cm
Can be repaired either open or
laparoscopic with mesh
1-4cm midline ventral – open
1-4cm incisional – open or laparoscopic
4-10cm all types – laparoscopic
> 10cm
Unlikely to be closed laparoscopic
and require open
Cottage Physician
References
Park AE, Roth JS, Kavic SM. Abdominal wall
hernia. Current problems in surgery. 2006; 43(5):326-75. [pubmed]
Earle DB, McLellan JA. Repair of umbilical and
epigastric hernias. The Surgical clinics of North America. 2013; 93(5):1057-89.
[pubmed]
Flament JB. [Functional anatomy of the abdominal
wall]. Der Chirurg; Zeitschrift fur alle Gebiete der operativen Medizen. 2006;
77(5):401-7. [pubmed]
Ellis H. Applied anatomy of abdominal incisions.
British journal of hospital medicine (London, England : 2005). 2007;
68(2):M22-3. [pubmed]
Rutkow IM. Demographic and socioeconomic aspects
of hernia repair in the United States in 2003. The Surgical clinics of North
America. 2003; 83(5):1045-51, v-vi. [pubmed]
McIntosh A, Hutchinson A, Roberts A, Withers H.
Evidence-based management of groin hernia in primary care–a systematic review.
Family practice. 2000; 17(5):442-7. [pubmed]
Murphy KP, O’Connor OJ, Maher MM. Adult
abdominal hernias. AJR. American journal of roentgenology. 2014;
202(6):W506-11. [pubmed]
Bedewi MA, El-Sharkawy MS, Al Boukai AA,
Al-Nakshabandi N. Prevalence of adult paraumbilical hernia. Assessment by
high-resolution sonography: a hospital-based study. Hernia : the journal of
hernias and abdominal wall surgery. 2012; 16(1):59-62. [pubmed]
Earle D, Roth JS, Saber A, et al. SAGES
guidelines for laparoscopic ventral hernia repair. Surgical endoscopy. 2016;
30(8):3163-83. [pubmed]
Sailes
FC, Walls J, Guelig D, et al. Synthetic and biological mesh in component
separation: a 10-year single institution review. Annals of plastic surgery.
2010; 64(5):696-8. [pubmed]
Shell
DH, de la Torre J, Andrades P, Vasconez LO. Open repair of ventral incisional
hernias. The Surgical clinics of North America. 2008; 88(1):61-83, viii. [pubmed]
Luijendijk
RW, Hop WC, van den Tol MP, et al. A comparison of suture repair with mesh
repair for incisional hernia. The New England journal of medicine. 2000;
343(6):392-8. [pubmed]
DiBello
JN, Moore JH. Sliding myofascial flap of the rectus abdominus muscles for the
closure of recurrent ventral hernias. Plastic and reconstructive surgery. 1996;
98(3):464-9. [pubmed]
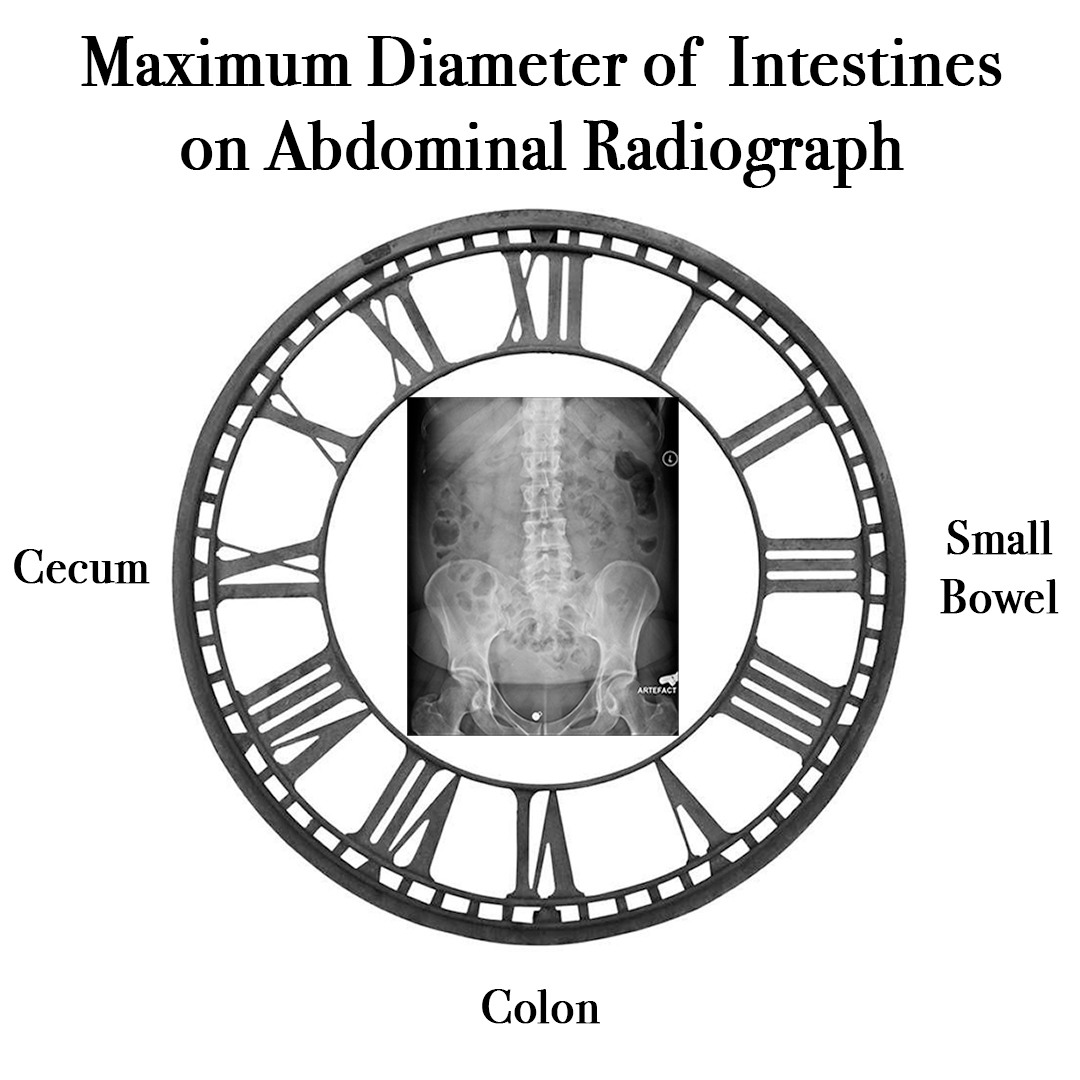
When looking an abdominal radiograph, what are the bowel diameter measurements that are generally NOT normally exceeded and would be concerning for potential obstruction?
Answer
The normal diameter of the intestines on an abdominal radiograph generally do not exceed:
Definition – space in the peritoneal cavity between the rectum and the posterior wall of the uterus
Clinical Significance – As this is the most posterior and inferior recess in the peritoneal cavity, it is a potential space for fluid and blood to accumulate. This area should always be investigated in trauma as part of the FAST examination.
History – Named after James Douglas (1675-1742), who was a Scottish physician, anatomist, and physician extraordinaire to Queen Caroline. He received his medical doctorate from University of Reims and went on to have a prolific career as an obstetrician and anatomist. He also befriended an early career William Hunter and made him an assistant prior to his own fame as an anatomist. Due to his anatomic research in female pelvic anatomy, there are many eponymonic structures that bear his name including the Douglas fold, Douglas line, and Douglas septum.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
When looking an abdominal radiograph, what are the bowel diameter measurements that are generally NOT normally exceeded and would be concerning for potential obstruction?
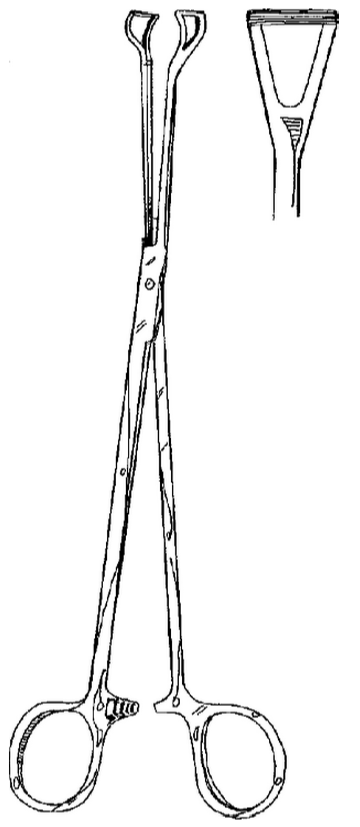
What is the main difference between these two instruments?
vs
Answer
The first instrument is an Allis clamp, which has sharp teeth and can crush tissue. It is used for grasping fascia or tissue that needs to be removed or manipulated during procedures.
The second instrument is a Babcock forceps, which is non-toothed and has a wider grasping surface. These forceps do not damage tissue and are considered non-crushing and can be used to grasp delicate tissue. The head of the forceps is open and helps for rapid identification.
Clinical Significance – used for delicate vascular surgery as these forceps do not crush or damage tissue
History –Named after Michael Ellis DeBakey (1908-2008), an American cardiac surgeon who received his medical degree from Tulane University School of Medicine in 1932. He spent the majority of his career with Baylor in Texas and was prolific medical trailblazer and pioneered, among many others,:
The roller pump for the heart-lung machine and made open-heart surgery possible
Postulating the link between smoking and lung cancer
One of the first surgeons to perform coronary artery bypass
Performed the first successful carotid endarterectomy
Using synthetic grafts for blood vessel repair
Video live surgery for medical purposes
In 2005, at the age of 95, he suffered an aortic dissection (for which there is the DeBakey classfication for) and became the oldest person to survive the operation. He died 2 months before his 100th birthday. Dr. DeBakey received so many awards and recognition that they are too numerous to count and is arguable one of the main reasons modern cardiac surgery has advanced to where it is today.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.