You are winding down your 8a-8p shift in the fast track section of your emergency department when a 19-month girl is brought in my her father after falling out of a shopping cart at Home Depot at around 7:15pm. Her father saw her fall and couldn’t catch her before she hit the ground. She immediately began crying and her father denies any loss of consciousness or vomiting. She cried for approximately 30 minutes and her father started to worry that she is now “sleepy”. Other than the sleepiness, her behavior has been normal per her father.
Physical examination does not reveal any periorbital or posterior auricular ecchymosis and there is no hemotympanum. There are no other abrasions or ecchymosis present and her eyes are open and she can track your movements. There is no palpable depressions or crepitus on the skull. She is moving all extremities, reaching for her toys, and saying “Daddy” towards her father.
Does this child need further imaging?
What studies are available to help make this decision?
Definition – Set of clinical decision instruments to help predict pretest probability in various injuries and need for further radiographical studies
Clinical Significance – There are four Ottawa Rules clinical decision instruments that are currently used:
Knee
Foot and Ankle
Cervical Spine
Head CT in mild head injury
History – Named after The Ottawa Hospital Research Institute and the University of Ottawa over series of publications from 1992-2001. These publications have been validated numerous times and shown to decrease health care costs, unnecessary radiographic studies, and decrease throughput time in the emergency department. The brain behind these studies is Ian Stiell, a Canadian physician researcher who received his medical doctorate from the University of Ontario and completed his residency at McGill University. With over 370 publications to his name, he is a powerhouse in the realm of emergency medicine research.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Stiell IG, Wells GA, Vandemheen KL, et al. The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA. 2001; 286(15):1841-8. [pubmed]
Stiell IG, Greenberg GH, Wells GA, et al. Derivation of a decision rule for the use of radiography in acute knee injuries. Annals of emergency medicine. 1995; 26(4):405-13. [pubmed]
Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Worthington JR. A study to develop clinical decision rules for the use of radiography in acute ankle injuries. Annals of emergency medicine. 1992; 21(4):384-90. [pubmed]
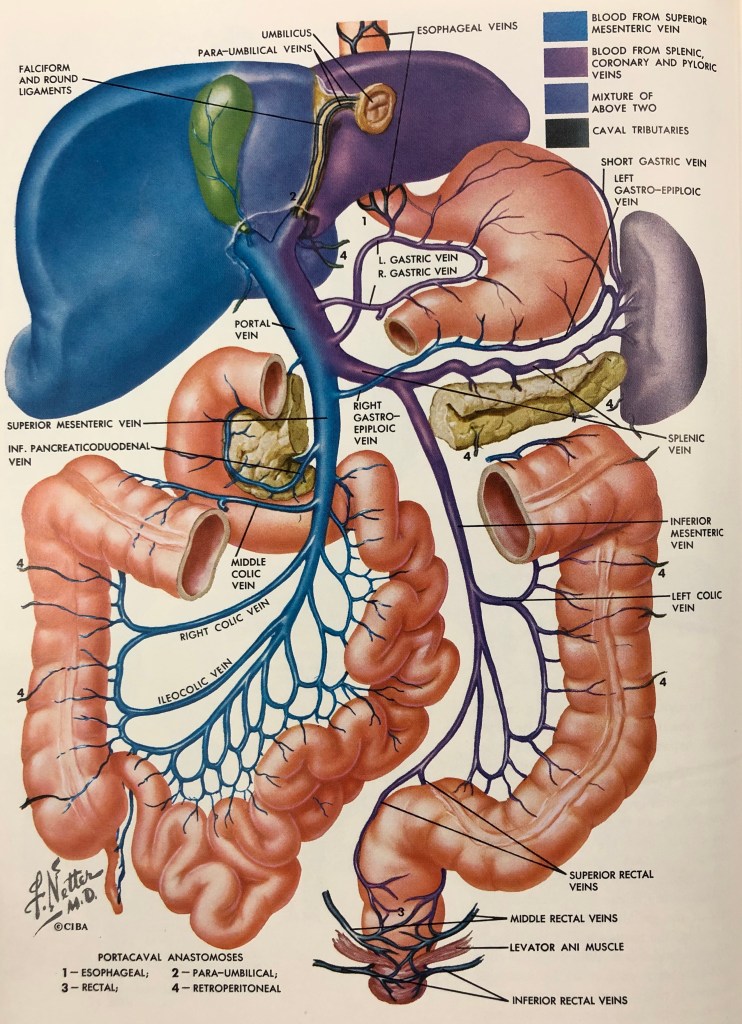
Cirrhosis and intrinsic liver disease can cause a significant increase in pressure within the portal system and result in dilation of the caval tributaries. What are the three (3) most common locations these dilations occurs?
Answer
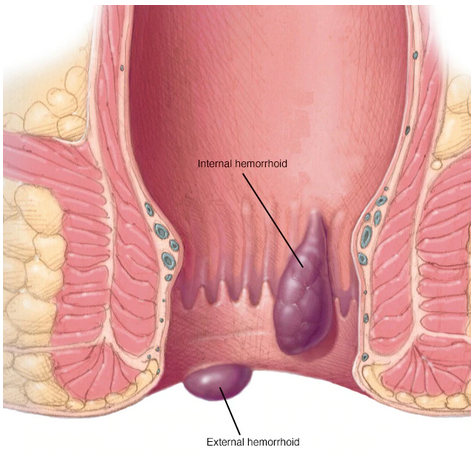
The three (3) most common locations where you can find dilation of portal caval tributaries as a result of portal hypertension are:
Other Known Aliases – gastro-esophageal laceration syndrome
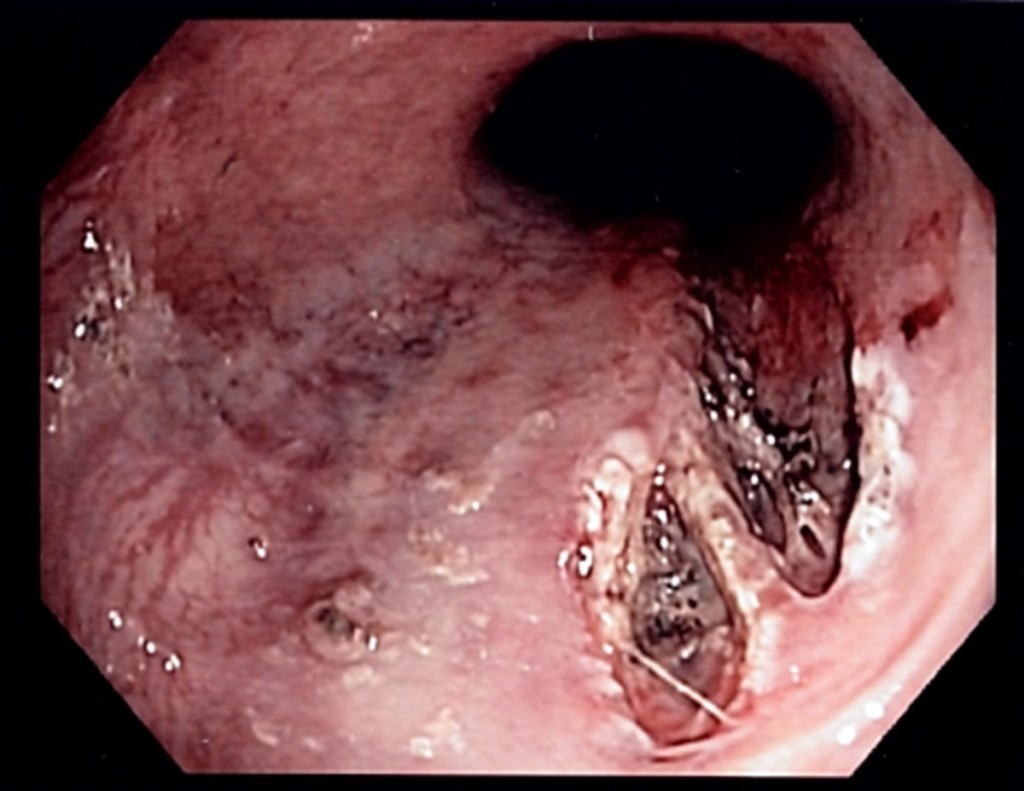
Definition – longitudinal mucosal lacerations in the distal esophagus and proximal stomach often leading to bleeding from submucosal arteries
Clinical Significance – These tears often occurs as a result of forceful vomiting and can present with hematemesis or melena. Risk factors include alcohol abuse, hiatal hernias, and bulemia. In contrast to Boerhaave’s syndrome, this only involves the mucosa and submucosa and therefor, is not a full thickness rupture. Diagnosis is made via endoscopy and treatment depends on how active the bleed is at the time of endoscopy.
History – Named after two physicians, George Kenneth Mallory (1900-1986) and Soma Weiss (1898-1942), from Boston. Dr. Mallory received his medical doctorate from Harvard Medical School in 1926 and followed in his father’s footsteps by working at the Mallory Institute of Pathology at Boston City Hospital. Dr. Weiss studied physiology and biochemistry in Budapest before immigrating to the United States immediately after World War I, when he wualified in medicine in 1923. He started his career at Cornell before moving to Harvard Medical School, and finally becoming physician-in-chief and professor at The Brigham Hospital in 1939. They partnered and co-authored the manuscript with their eponymous name in 1929, where they described 15 cases of severe, painless hemorrhage of the esophagus preceded by vomiting in alcoholics. They followed this up in 1932 with an additional 6 cases.
George Kenneth Mallory
Soma Weiss
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Mallory GK, Weiss A. Hemorrhages from lacerations of the cardiac orifice of the stomach due to vomiting. American Journal of the Medical Sciences. 1929; 178: 506-15
Weiss S, Mallory GK. Lesions of the cardiac orifice of the stomach produced by vomiting. Journal of the American Medical Association; 1932, 98: 1353-1355
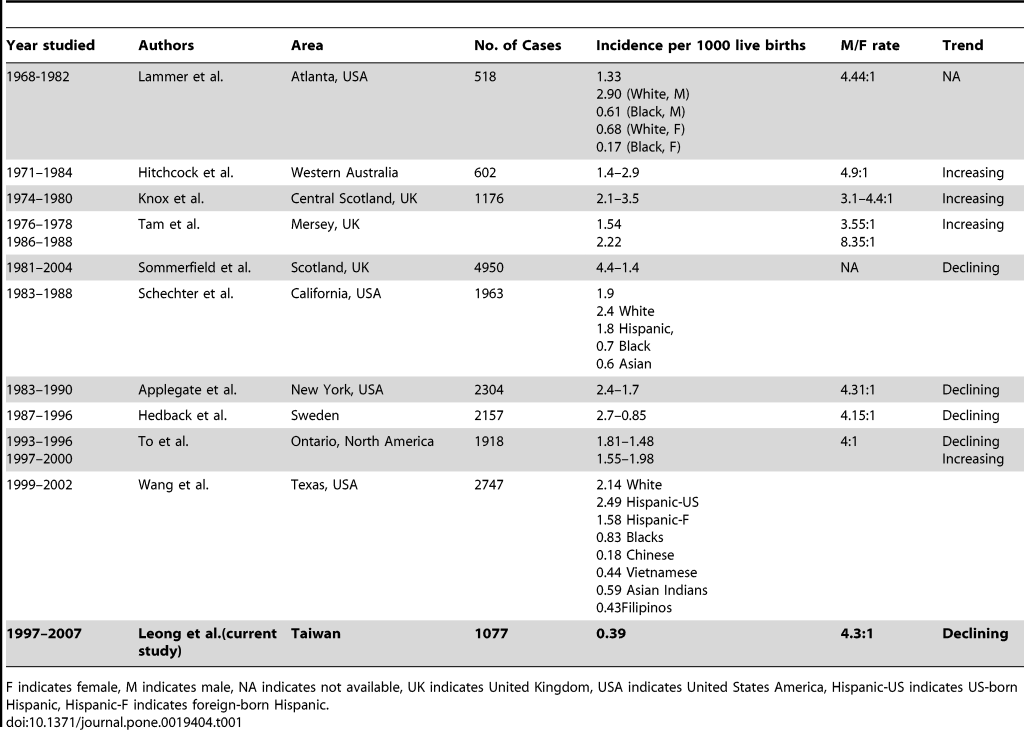
2-4 per 1000 live births worldwide and 20 per 10,000 live births in the US
Higher male to female ratio (4-6:1)
Higher incidence (1.5x) in first-born children
Highest incidence in caucasian infants
Less common in infants of older mothers
Risk Factors and Etiology
The exact mechanisms and etiologies are unclear, but it is hypothesized that it is multifactorial and is a result of both genetic predisposition and environmental triggers.
Environmental Factors
Maternal smoking (up to 2x increased risk)
Bottle feeding
Bottle feeding during first 4 months increased risk by 4x
Didn’t delineate formula vs breastmilk
Genetic Factors
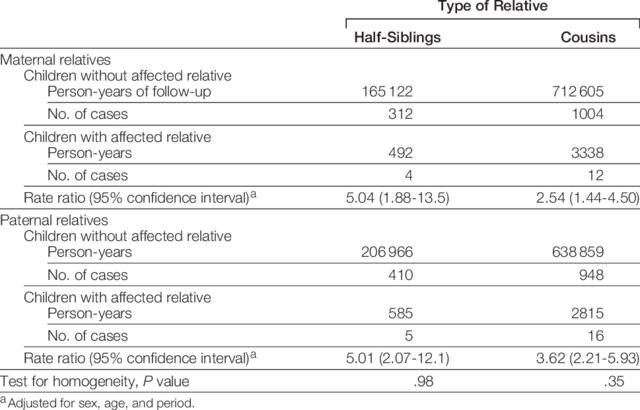
Reports of familial aggregation, but there is no clear research association
Apolipoprotein A1 (APOA1) gene cluster
Hypothesized low plasma cholesterol at birth and increased risk
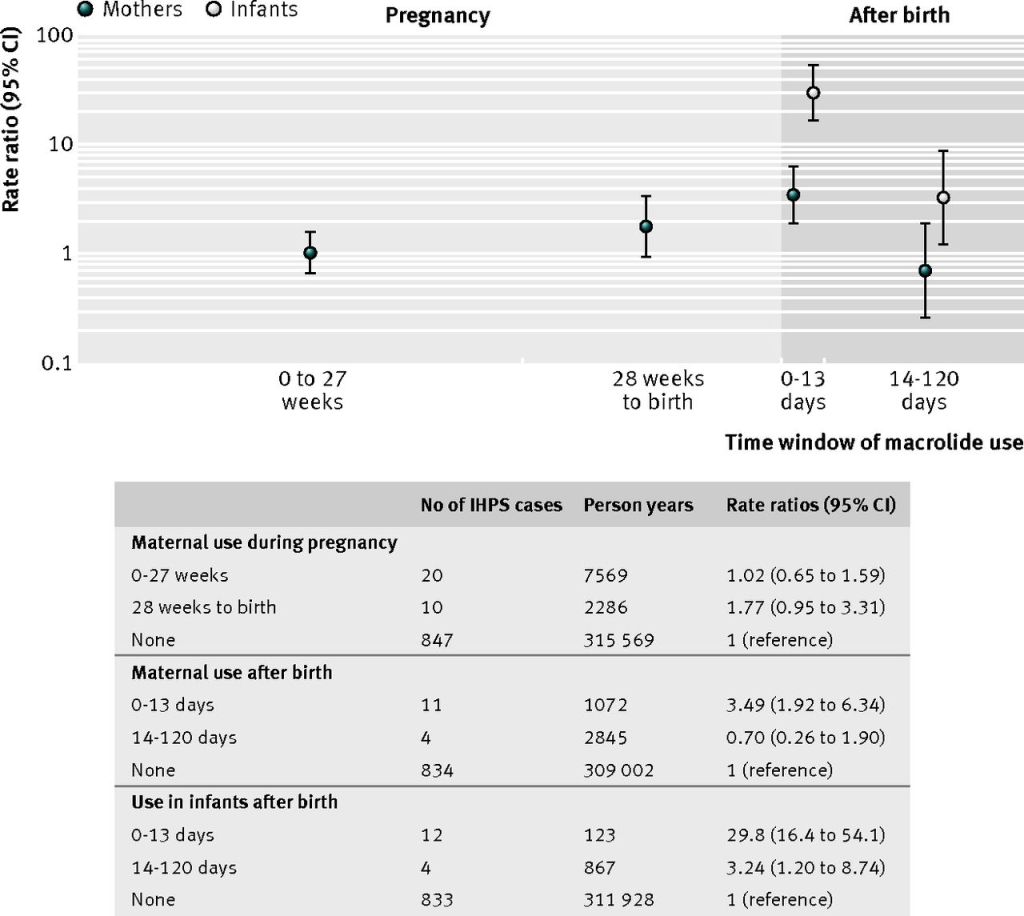
Macrolide Antibiotics
Increased risk if given to infants < 2 weeks old
Treatment/prophylaxis for pertussis
Association with maternal use during first two weeks of life
Icteropyloric syndrome
Unconjugated hyperbilirubinemia
Most commonly from early Gilbert’s Syndrome
History and Physical Examination
Class presentation for PANCE
< 6 week old with post-prandial, non-bilious projectile vomiting around 10 minutes after cessation of feeding
Ravenous feeder even after vomiting
May be emaciated and/or dehydrated
Though we are diagnosing earlier and infants tend to be healthier
Palpable mass in the epigastrium (50-90%)
This is also less commonly seen due to healthier infants and ease of obtaining radiologic students
73% in the 1970s to only 30% now
Felt as a firm mass at the lateral edge of the rectus abdominis muscle in the RUQ
Although pyloric stenosis has a classic presentation, you must entertain the other important causes of vomiting in infancy.
Treatment
Definitive management is surgery
Timing of surgery depends on the clinical status of the infant
If healthy, surgery can be performed on the day of diagnosis
If ill, then resuscitation and feeding need to be performed to limit perioperative complications.
Technique
Ramstedt Pyloromyotomy
Longitudinal incision of the pylorus with blunt dissection down to the submucosa
Open vs Laparoscopic
No difference in operating time, time to full feeding, or length of stay
Laparoscopic had lower incidence of emesis and better pain control, but higher incidence of incomplete surgical release
Postoperative Management
Feeding
Resumed within a few hours after surgery
Regurgitation is common, but should
not delay/stop feedings
Breathing
Monitor for apnea at least for 24
hours
Complications
Mucosal perforation (rare)
Follow-Up
Surgery is curative in the majority
of patients
Once normal feeds occur, only
routine pediatric care and follow-up is needed
Reflux is common and managed
conservatively
The Cottage Physician (1893)
References
Kapoor R, Kancherla V, Cao Y, et al. Prevalence and descriptive epidemiology of infantile hypertrophic pyloric stenosis in the United States: A multistate, population-based retrospective study, 1999-2010. Birth defects research. 2019; 111(3):159-169. [pubmed]
To T, Wajja A, Wales PW, Langer JC. Population demographic indicators associated with incidence of pyloric stenosis. Archives of pediatrics & adolescent medicine. 2005; 159(6):520-5. [pubmed]
Krogh C, Fischer TK, Skotte L, et al. Familial aggregation and heritability of pyloric stenosis. JAMA. 2010; 303(23):2393-9. [pubmed]
Krogh C, Gørtz S, Wohlfahrt J, Biggar RJ, Melbye M, Fischer TK. Pre- and perinatal risk factors for pyloric stenosis and their influence on the male predominance. American journal of epidemiology. 2012; 176(1):24-31. [pubmed]
Svenningsson A, Svensson T, Akre O, Nordenskjöld A. Maternal and pregnancy characteristics and risk of infantile hypertrophic pyloric stenosis. Journal of pediatric surgery. 2014; 49(8):1226-31. [pubmed]
Zhu J, Zhu T, Lin Z, Qu Y, Mu D. Perinatal risk factors for infantile hypertrophic pyloric stenosis: A meta-analysis. Journal of pediatric surgery. 2017; 52(9):1389-1397. [pubmed]
McAteer JP, Ledbetter DJ, Goldin AB. Role of bottle feeding in the etiology of hypertrophic pyloric stenosis. JAMA pediatrics. 2013; 167(12):1143-9. [pubmed]
Sørensen HT, Nørgård B, Pedersen L, Larsen H, Johnsen SP. Maternal smoking and risk of hypertrophic infantile pyloric stenosis: 10 year population based cohort study. BMJ (Clinical research ed.). 2002; 325(7371):1011-2. [pubmed]
Feenstra B, Geller F, Carstensen L, et al. Plasma lipids, genetic variants near APOA1, and the risk of infantile hypertrophic pyloric stenosis. JAMA. 2013; 310(7):714-21. [pubmed]
Eberly MD, Eide MB, Thompson JL, Nylund CM. Azithromycin in early infancy and pyloric stenosis. Pediatrics. 2015; 135(3):483-8. [pubmed]
Honein MA, Paulozzi LJ, Himelright IM, et al. Infantile hypertrophic pyloric stenosis after pertussis prophylaxis with erythromcyin: a case review and cohort study. Lancet (London, England). ; 354(9196):2101-5. [pubmed]
Lund M, Pasternak B, Davidsen RB, et al. Use of macrolides in mother and child and risk of infantile hypertrophic pyloric stenosis: nationwide cohort study. BMJ (Clinical research ed.). 2014; 348:g1908. [pubmed]
Touloukian RJ, Higgins E. The spectrum of serum electrolytes in hypertrophic pyloric stenosis. Journal of pediatric surgery. 1983; 18(4):394-7. [pubmed]
Bakal U, Sarac M, Aydin M, Tartar T, Kazez A. Recent changes in the features of hypertrophic pyloric stenosis. Pediatrics international : official journal of the Japan Pediatric Society. 2016; 58(5):369-71. [pubmed]
Sivitz AB, Tejani C, Cohen SG. Evaluation of hypertrophic pyloric stenosis by pediatric emergency physician sonography. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2013; 20(7):646-51. [pubmed]
Niedzielski J, Kobielski A, Sokal J, Krakós M. Accuracy of sonographic criteria in the decision for surgical treatment in infantile hypertrophic pyloric stenosis. Archives of medical science : AMS. 2011; 7(3):508-11. [pubmed]
Hernanz-Schulman M. Pyloric stenosis: role of imaging. Pediatric radiology. 2009; 39 Suppl 2:S134-9. [pubmed]
Said M, Shaul DB, Fujimoto M, Radner G, Sydorak RM, Applebaum H. Ultrasound measurements in hypertrophic pyloric stenosis: don’t let the numbers fool you. The Permanente journal. 2012; 16(3):25-7. [pubmed]
Iqbal CW, Rivard DC, Mortellaro VE, Sharp SW, St Peter SD. Evaluation of ultrasonographic parameters in the diagnosis of pyloric stenosis relative to patient age and size. Journal of pediatric surgery. 2012; 47(8):1542-7. [pubmed]
St Peter SD, Holcomb GW, Calkins CM, et al. Open versus laparoscopic pyloromyotomy for pyloric stenosis: a prospective, randomized trial. Annals of surgery. 2006; 244(3):363-70. [pubmed]
Hall NJ, Pacilli M, Eaton S, et al. Recovery after open versus laparoscopic pyloromyotomy for pyloric stenosis: a double-blind multicentre randomised controlled trial. Lancet (London, England). 2009; 373(9661):390-8. [pubmed]
Cirrhosis and intrinsic liver disease can cause a significant increase in pressure within the portal system and result in dilation of the caval tributaries. What are the three (3) most common locations these dilations occurs?
Definition – esophageal rupture from forceful vomiting
Clinical Significance – This rupture occurs as a result of sudden increased intraesophageal pressure with negative intrathoracic pressure and the associated tear is most commonly located on the left posterolateral aspect of the distal esophagus. Gastric contents then invade the mediastinum and cause mediastinitis, necrosis, and severe bacterial infection that can lead to significant mortality.
History – Named after Herman Boerhaave (1668-1738), who was a Dutch physician and earned his medical doctorate from the University of Harderwijk in 1693. He went on to earn a professorship at the University of Leiden in 1701, speaking on medicine, anatomy, botany, chemistry, and philosophy. It was during his time here that his repuatation as a skilled orator and teacher made international waves and physicians from all over the world came to listen and learn. He first described his eponymous disease in 1724 after witnessing the death of Baron Jan van Wassenaer after a retching following a particularly gluttonous feast.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Boerhaave H. Atrocis, nec descripti prius, morbii historia: secundum medicae artis leges conscripta. Leiden, the Netherlands: Lugduni Batavorum Boutesteniana, 1724
Underwood EA. Boerhaave after three hundred years. British medical journal. 1968; 4(5634):820-5. [pubmed]
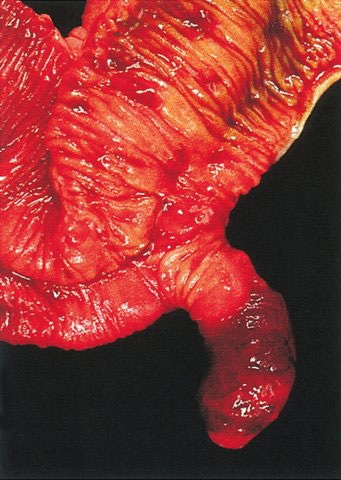
Definition – Vestigial remnant of the omphalomesenteric (vitiline) duct
Clinical Significance – It is the most common malformation in the GI tract and is mainly asymptomatic. When symptoms do occur, it commonly presents as painless, rectal bleeding in children. The “Rule of 2s” will help you remember the facts of this pathology:
Effects 2% of the population
2% of these will be symptomatic by age 2
2 types of heterotopic tissue
Boy-to-girl ratio is 2:1
Usually 2″ in length
2′ from the ileocecal valve
History – Named after Johann Friedrich Meckel, the Younger (1781-1833), who was a German anatomist and received his medical doctorate from the University of Halle in 1802. He then went on to become full professor of anatomy, surgery, and obstetrics at the University of Halle in 1808 after studying Würzburg, Vienna, and Paris. He made tremendous advancements in the area of anatomy and embryonic development with special attention to birth defects and abnormalities, where he pioneered the early study of teratology. He first published his eponymous finding in 1809 in an article entitled “Über die Divertikel am Darmkanal” in the Halle Archives of Physiology. Of note, he comes from a prestigous medical family, where both his father, grandfather, and brother were physicians….hence the surname “the Younger”.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Stallion A, Shuck JM. Meckel’s Diverticulum. Surgical Treatment: Evidence-Based and Problem-Oriented. 2001 [pubmed]
Blackbourne LH. Surgical Recall. 6th ed. 2012
J. F. Meckel. Über die Divertikel am Darmkanal. Archiv für die Physiologie, Halle, 1809, 9: 421–453
Klunker R, Göbbel L, Musil A, Tönnies H, Schultka R. Johann Friedrich Meckel the Younger (1781-1833) and modern teratology. Annals of Anatomy. 2002; 184(6):535-40. [pubmed]