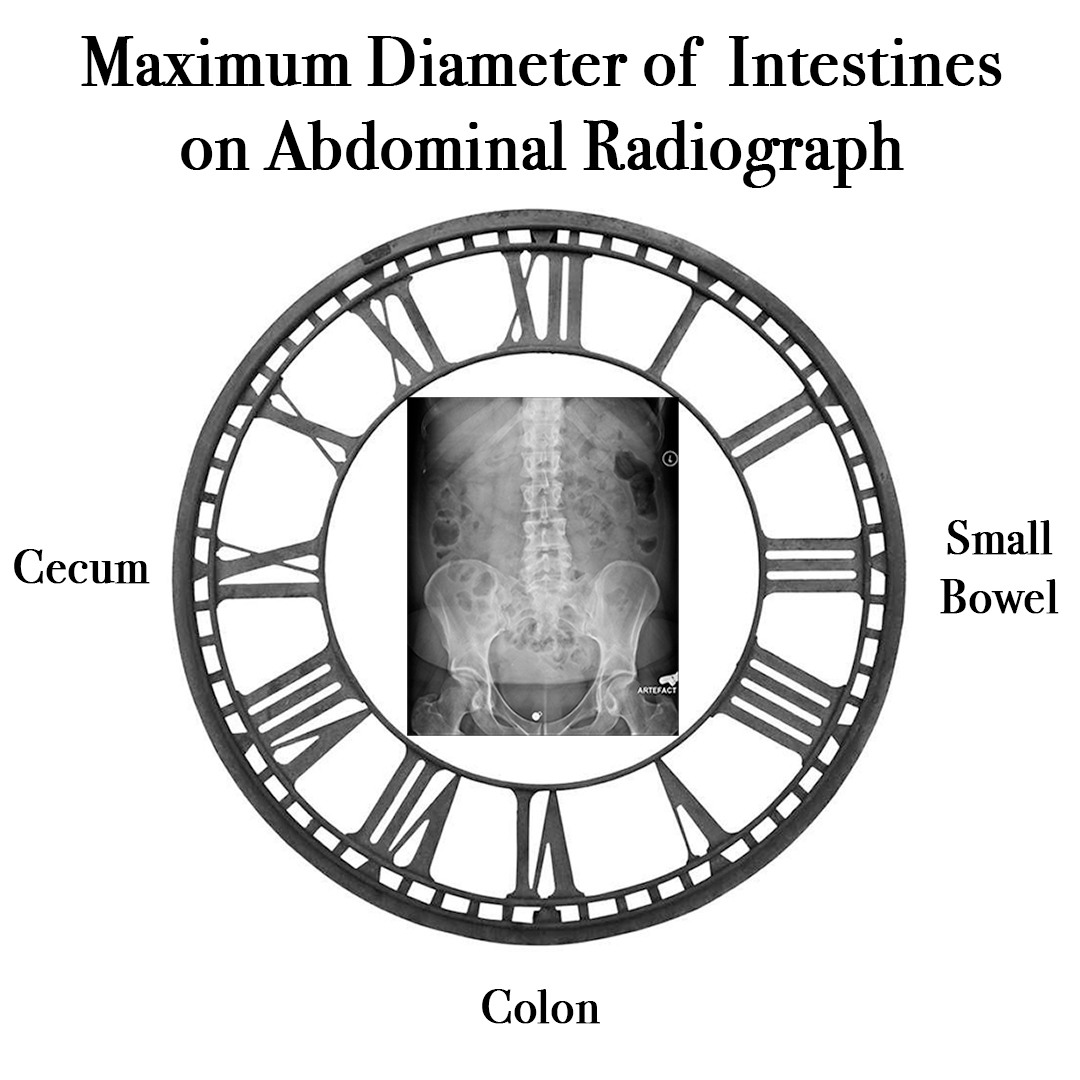
When looking an abdominal radiograph, what are the bowel diameter measurements that are generally NOT normally exceeded and would be concerning for potential obstruction?
Answer
The normal diameter of the intestines on an abdominal radiograph generally do not exceed:
Definition – space in the peritoneal cavity between the rectum and the posterior wall of the uterus
Clinical Significance – As this is the most posterior and inferior recess in the peritoneal cavity, it is a potential space for fluid and blood to accumulate. This area should always be investigated in trauma as part of the FAST examination.
History – Named after James Douglas (1675-1742), who was a Scottish physician, anatomist, and physician extraordinaire to Queen Caroline. He received his medical doctorate from University of Reims and went on to have a prolific career as an obstetrician and anatomist. He also befriended an early career William Hunter and made him an assistant prior to his own fame as an anatomist. Due to his anatomic research in female pelvic anatomy, there are many eponymonic structures that bear his name including the Douglas fold, Douglas line, and Douglas septum.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
When looking an abdominal radiograph, what are the bowel diameter measurements that are generally NOT normally exceeded and would be concerning for potential obstruction?
Other Known Aliases – factitious disorder imposed on self
Definition – intentional falsification of physical and/or mental signs and symptoms in oneself, or in another individual, for no obvious external gain or reward
Clinical Significance – Falling under the factitious disorders section of the DSM-V 300.19 (ICD-10 – F68.10), patients deceptively misrepresent, simulate, or cause symptoms of an illness or injury in themselves, even in the absence of obvious external rewards such as financial gain, housing, or medications.
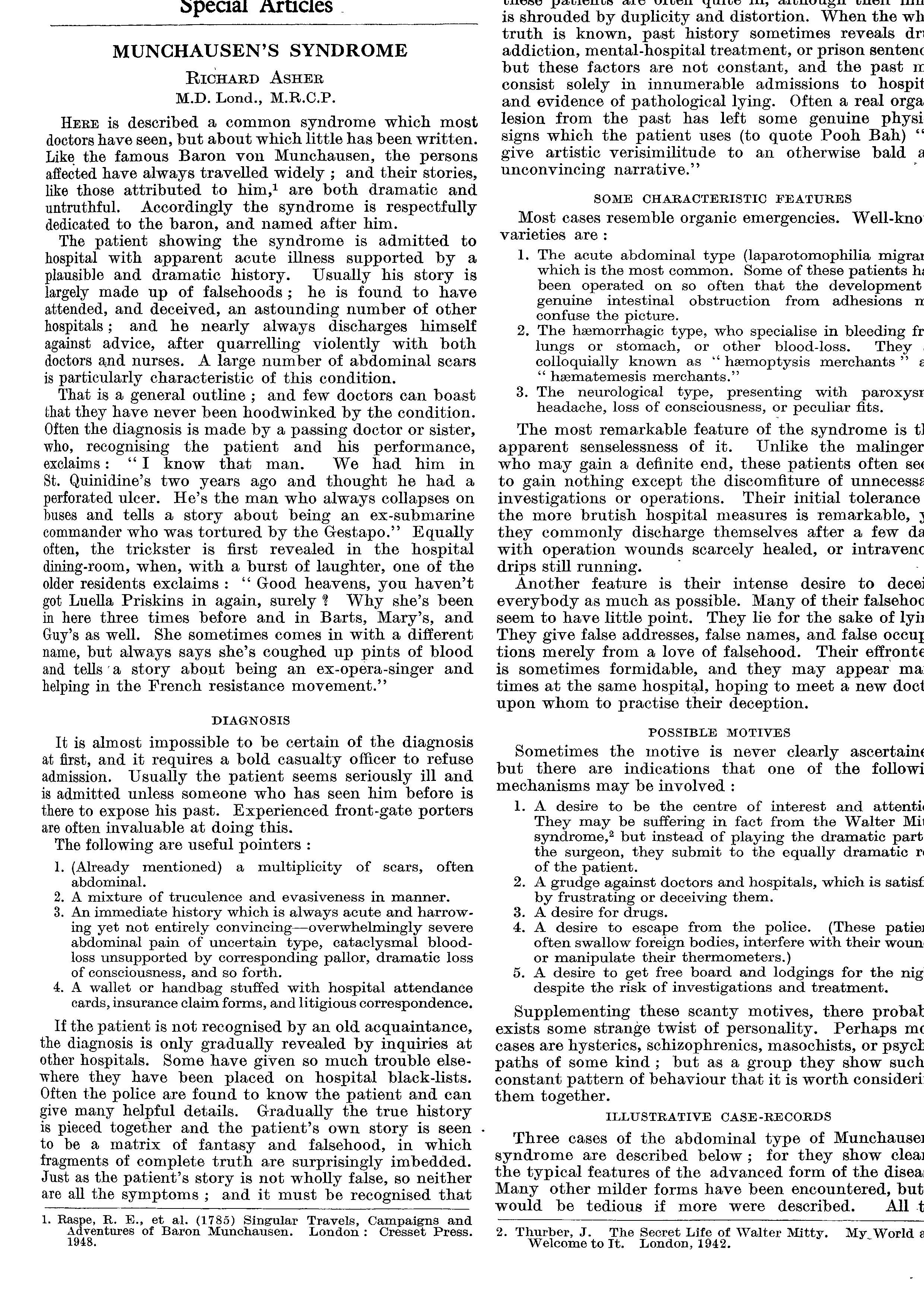
History – Named after Hieronymus Karl Friedrich von Münchhausen (1720-1797), who was a German aristocrat and military veteran. He was best known for telling elaborate stories at aristocratic dinner parties where he would embellish his tales of being a soldier and huntsman. It was during these dinner parties that he met Rudolf Erich Raspe, who was a German writer, scientist, and con artist. He found these stories so alluring and entertaining that he used them (almost verbatim) in a series of publications describing these adventures of the titular character Baron von Munchausen. Münchhausen took offense to his noble name being used to entertain commoners and attempted litigious retribution against Raspe for many years to no avail. This story did not reach eponymous notoriety until 1951 when Dr. Richard Asher published an article in The Lancet entitled “Munchausen’s Syndrome” did the eponym stick.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Definition – chronological progression of emotional states after experiencing profound personal loss
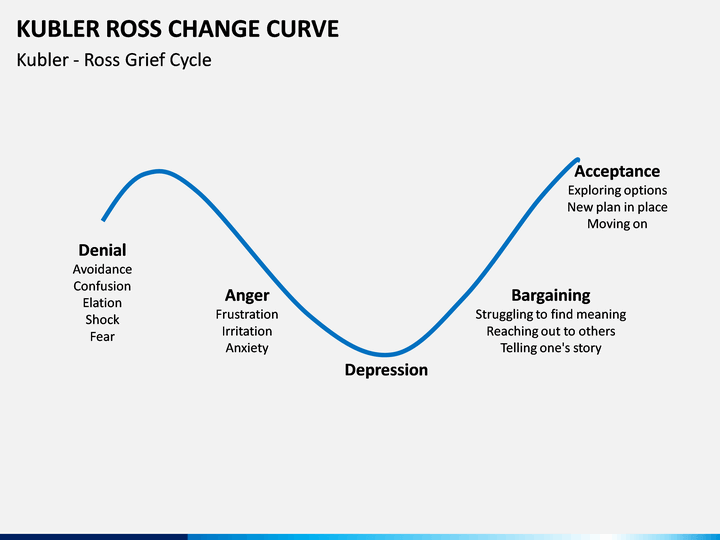
Clinical Significance – The five distinct phases of this model include denial, anger, bargaining, depression, and acceptance. Although widely used, it is not based on any empirical research or evidence and can be affected by cultural norms. In fact, many mental health professionals put this in the “myth” file and say that grief/loss is not a staged event, but rather a spectrum that a person can go backwards and forwards through at any point after the event.
History – Named after Elisabeth Kübler-Ross (1926-2004), who was a Swiss-American psychiatrist and recieved her medical doctorate from the University of Colorado in 1963. It was during this training that she was appalled by the treatment and management of terminally ill patients and began what would be her life’s work and passion. In 1965, she accepted an instructor position at the University of Chicago Pritzker School of Medicine and began given seminars using medical students to conduct interviews with terminally ill patients. These seminars drew both appraise and criticism, as she called into question many traditionally accepted practices of psychiatry at the time. This all culminated in 1969 where she proposed her 5 stages of grief model in her book entitled On Death and Dying. In her later career, she embraced holistic medicine and spiritulism and founded a spiritual healing center called “Shanti Nilaya” in California. Dr. Kübler-Ross suffered a series of strokes in 1995, which left her paralyzed on left side, and died in a nursing home in Scottsdale, AZ in 2004.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
There are two tests that you can perform at bedside in patients with suspected myasthenia gravis. One is an easy adjunct to the neurologic exam and the other is only included for historical purposes. Name these tests.
Answer
The most reliable way to diagnose myasthenia gravis is through serologic laboratory studies assessing acetylcholine receptor and muscle-specific tyrosine kinase antibodies. But……………there are two bedside tests that can help prior to expensive labs.
Ice Pack Test
Used as part of the neurologic examination, it is based on the physiologic principle that neuromuscular transmission improves at lower muscle temperature. In patients with myasthenia gravis, placing an ice pack over a closed eyelid for 2 minutes can improve ptosis in 80% of patients.
Taught more for historical purposes, edrophonium is an acetylcholinesterase inhibitor with a rapid onset and short duration of action. The main effect is prolonging acetylcholine in the neuromuscular junction to improve muscular strength.
It is not available in the US, nor used in the diagnosis
Definition – pupil with parasympathetic denervation that constricts poorly to light, but reacts better to accommodation.
Clinical Significance – The tonic pupil is the result of damage to the parasympathetic ciliary ganglion and the exact pathological cause is still unknown, but infectious inflammation to the ciliary ganglion is the most commonly accepted etiology. Adie’s pupils are hypersensitive to very low dose acetylcholine agonists, such as pilocarpine, and is used to diagnose this condition.
History – Named after William John Adie (1886-1935), who was a British physician and neurologist and received his medical doctorate from the University of Edinburgh in 1911. Upon graduating, he served in the British military during World War I as a medical officer. Following the war, he worked in various hospitals practicing neurology and making a name for himself, culminating in Fellowship in the Royal College of Physicians in 1926. He was also one of the founders of the Association of British Neurologists in 1932. The history of the eponym is interesting because there were numerous publications prior to Adie’s work describing this clinical syndrome and Adie referenced them in his 1931 article. The eponymonic term was given to him by French neurologist Jean-Alexandre Barré in 1934. Also, Gordon Morgan Holmes contemporaneously published the same findings in the same year. This led to the common eponym Holmes-Adie pupils.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Adie WJ. Pseudo-Argyll Robertson pupils with absent tendon reflexes. A benign disorder simulating tabes dorsalis. British Medical Journal, London, 1931, I: 928-930. [article]
Holmes GM. Partial iridoplegia associated with symptoms of other disease of the nervous system. Transactions of the Ophthalmological Societies of the United Kingdom, 1931, 51: 209-228.
There are two tests that you can perform at bedside in patients with suspected myasthenia gravis. One is an easy adjunct to the neurologic exam and the other is only included for historical purposes. Name these tests.
Definition – abnormal fluid and ion homeostasis of the inner that leads to distortion and distention of the membranous, endolymph-containing portions of the labyrnthine system. It is currently unclear why this occurs and several etiologies have been proposed.
Clinical Significance – Ménière’s disease classically has the triad of tinnitus, sensorineural hearing loss, and episodic vertigo lasting from 20 minutes to 24 hours. The course and severity are variable and the frequency may actually decline over time. Treatment is geared towards diet and lifestyle modifications, vestibular suppressants, diuretics, and interventional procedures in severe or refractory cases.
History – Named after Prosper Ménière (1799-1862), who was a French physician and recieved his medical doctorate from the Hôtel-Dieu de Paris in 1828. He studied and assisted Guillaume Dupuytren at this famed hospital in France. During a particularly bad outbreak of cholera, he was sent by the king to Aude and Haute-Garonne to oversee this medical campaign and was so successful that he was made a knight of the Legion of Honour. Later, he became chief of medicine at the Imperial Institution for Deaf Mutes in Paris and published his findings on his eponymous disease in 1861.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
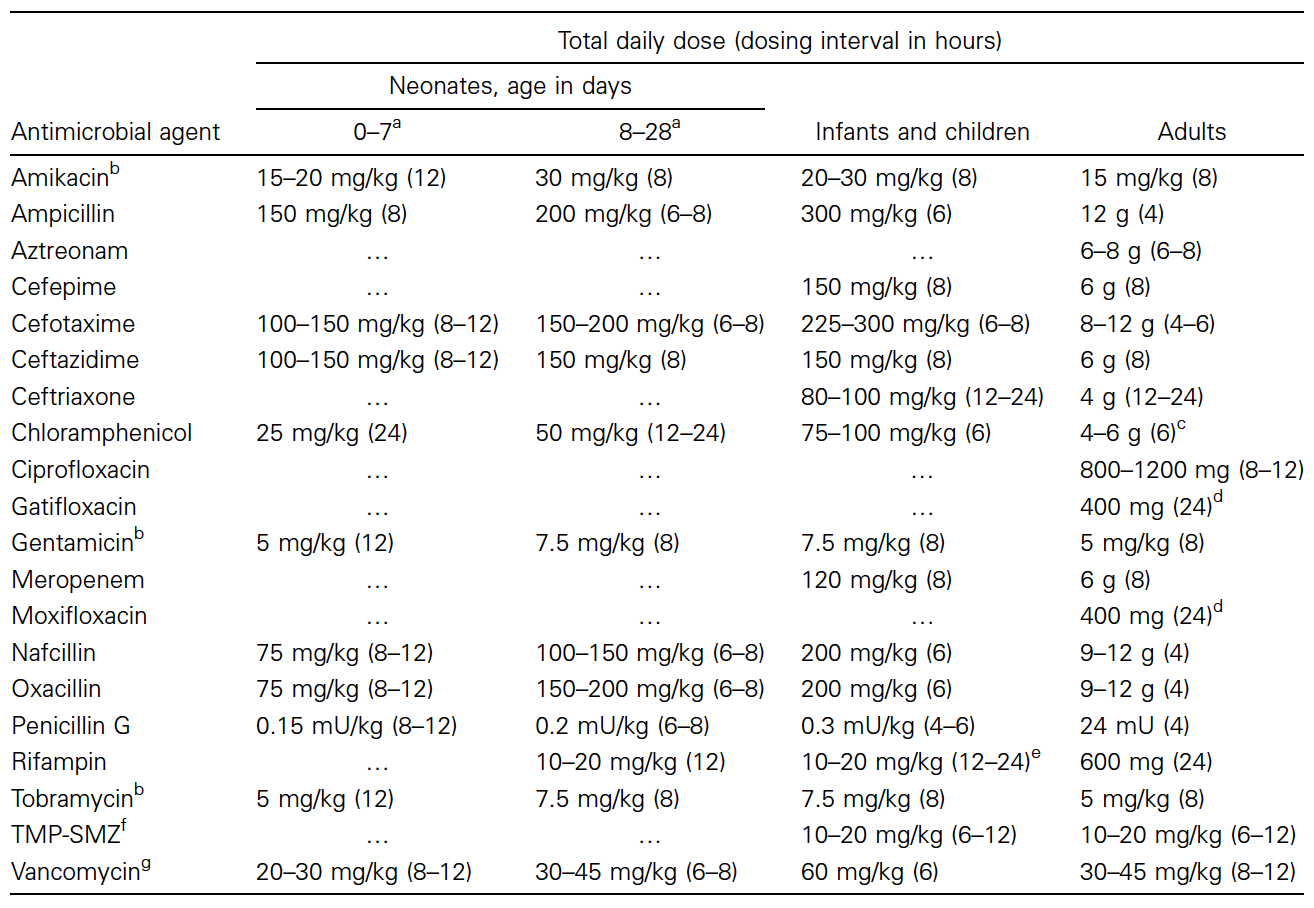
A 3-week old baby girl is sent to your emergency department after being seen by their pediatrician for irritability, poor feeding, and a seizure just prior to arrival at the pediatrician’s office. Vital signs are BP-103/73, HR-137, RR-25, O2-100% on room air, and Temp-39.2oC (102.5oF). Physical examination reveals a lethargic infant with decreased motor tone and a full, bulging frontal fontanelle. What is the most important diagnostic study to obtain and what is the empiric treatment of choice while awaiting results?
Answer
A full or bulging fontenelle is suggestive of meningeal edema and swelling are concerning for meningitis. Couple this with the lethargy and poor motor tone and this infant bought herself a lumbar puncture.
Now….because of her age (<30 days old), you have to cover for a specific set of pathogens due to a developing immune system. Classically, neonatal sepsis bugs include group B streptococcus (GBS), Escherichia coli, and Listeria monocytogenes. Empiric antibiotic coverage (until gram stain results) is: