Jones Fracture
Other Known Aliases – none
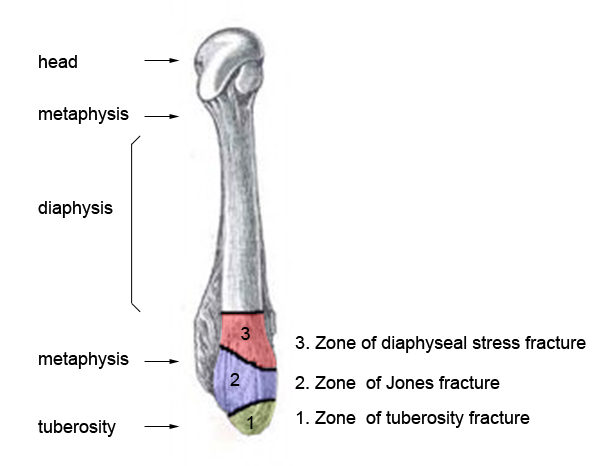
Definition – fracture of the base of the 5th metatarsal at the metaphyseal-diaphyseal junction

 Clinical Significance – Fairly easy radiographical diagnosis to make, but careful examination must distinguish between acute injuries in Zone 1 and 2 and chronic injuries in Zone 3.
Clinical Significance – Fairly easy radiographical diagnosis to make, but careful examination must distinguish between acute injuries in Zone 1 and 2 and chronic injuries in Zone 3.

History – Named after Sir Robert Jones (1857-1933), a Welsh orthopaedic surgeon and received his medical doctorate from the Liverpool School of Medicine in 1887 and achieved fellowship in 1889. Along with his uncle, he was a pioneer in the diagnosis and management of fractures. He first described the injury that bears his name in 1902 in the Annals of Surgery entitled “Fracture of the Base of the Fifth Metatarsal by Indirect Violence”. This paper was a six patient case report on the injury pattern and Dr. Jones was patient number one having injured his foot several months prior dancing. After Wilhem Rontgen published his discovery of x-rays in 1895, Dr. Jones adopted this new modality fully in the practice of orthopaedics and published the first clinical radiograph in 1896 about a 12yo with a bullet lodged in his wrist that could not be found clinically and required a 2hr long exposure.


References
- Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
- Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
-
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
- Whonamedit – dictionary of medical eponyms. http://www.whonamedit.com
- Up To Date. www.uptodate.com
- Jones Fracture. Wheeless’ Textbook of Orthopaedics. http://www.wheelessonline.com/ortho/jones_fracture
- OrthoBullets. https://www.orthobullets.com/foot-and-ankle/7031/5th-metatarsal-base-fracture
-
Jones R. I. Fracture of the Base of the Fifth Metatarsal Bone by Indirect Violence. Annals of surgery. 1902; 35(6):697-700.2. [pubmed]
- Jones R, Lodge O. The Discovery of a Bullet Lost in the Wrist by Means of the Roentgen Rays. Lancer. 1896;147(3782):476-477 [article]