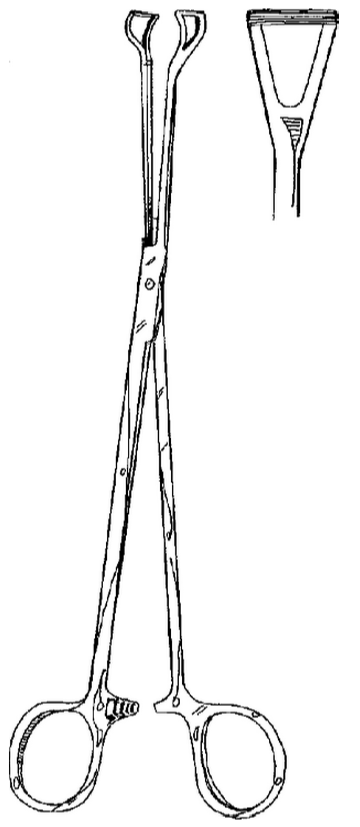
Clinical Significance – used for delicate vascular surgery as these forceps do not crush or damage tissue
History –Named after Michael Ellis DeBakey (1908-2008), an American cardiac surgeon who received his medical degree from Tulane University School of Medicine in 1932. He spent the majority of his career with Baylor in Texas and was prolific medical trailblazer and pioneered, among many others,:
The roller pump for the heart-lung machine and made open-heart surgery possible
Postulating the link between smoking and lung cancer
One of the first surgeons to perform coronary artery bypass
Performed the first successful carotid endarterectomy
Using synthetic grafts for blood vessel repair
Video live surgery for medical purposes
In 2005, at the age of 95, he suffered an aortic dissection (for which there is the DeBakey classfication for) and became the oldest person to survive the operation. He died 2 months before his 100th birthday. Dr. DeBakey received so many awards and recognition that they are too numerous to count and is arguable one of the main reasons modern cardiac surgery has advanced to where it is today.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Postoperative fever an elevation of body temperature to ≥ 38.3oC (100.4oF) following major surgical procedures. The vast majority of postoperative fevers occur within the first 5 days of surgery, which is why the timing of the fever is so important in differentiating the potential causes.
Physiologic Response to Surgery
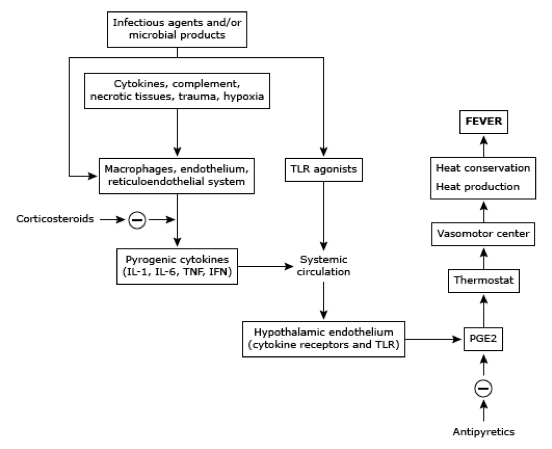
Surgery cause a massive inflammatory cascade due to the physiologic and cellular damage injury. This is a completely normal homeostatic response, but the release of IL-1, IL-6, and TNF-alpha (to name a few) are all pyrogenic cytokines that can contribute to a febrile response.
These cytokines act on the preoptic area of the hypothalamus to increase prostaglandin E2 secretion and raises the thermostatic endpoint of the body. This cascade usually peaks at 48 hours and care should be given to prevent costly and unnecessary infectious work-ups.
The Seven W’s of Postop Fever
Wind
Atelectasis usually occurs within the first 48 hours due to splinting and incomplete lung expansion secondary to pain following surgery. It has long been considered the leading cause of postop fever, but has been debunked in the literature for decades now with increased knowledge of the cellular inflammatory cascade. Decreased breath sounds , SOB, crackles, tachypnea can be indicators for atelectasis and CXR may show dependent, L>R infiltrates. Treatment should be incentive spirometry and early mobilization to promote expansion.
Water
Urinary tract infections (UTI) are the most common postoperative nosocomial infection secondary to the placement of a urinary catheter for surgery. Risk factors for postoperative UTI are length of catheterization need, female gender, older age, history of diabetes, and previous history of UTIs. Signs and symptoms can reveal suprapubic pain, CVA tenderness, flank pain, and malodorous, cloudy urine. Clean catch sample is ideal, but a clean aspirate from an indwelling catheter may be used. Urinalysis can provide a quick idea if it is infectious are not, specifically looking for positive nitrites and/or leukocyte esterase, or sending for a urine culture and finding > 105 cfu of the offending organism. Treatment should be removing the catheter (if possible) and tailoring antibiotic therapy to the organism in question.
Wound
Surgical site infections (SSI) generally begin to manifest 3-10 after surgery and risk factors for developing are ASA score of 3-5, contaminated or dirty procedure, or an extended length of surgery. Signs and symptoms of an SSI are increased pain, redness, and swelling at or near the incision. These can be superficial skin, deep skin, or deep space and ultrasound can help differentiate between cellulitis and focal infection. Treatment is either antibiotics (for cellulitis) or drainage (for abscess).
Walking
Deep venous thrombosis (DVT) can be common in surgical patient (up to 20%) secondary to immobilization and resistance to move due to pain. To make matters worse, many can be asymptomatic with the exception of the fever. The incidence is highest 3-5 days after surgery and you should have a low threshold to order a bilateral lower extremity ultrasound. Treatment for a DVT following surgery can be tricky due to bleeding risk.
Wonder Drugs
Medications are the most common, noninfectious cause of fever in patients following surgery. Timing is variable from immediately after administration to hours, or even days, later. Most cases are due to antibiotics or heparin and result in only a mild, transient febrile response. There are 3 life-threatening cause of medication induced fevers that you at least need to think of and rule-out:
Serotonin syndrome
Malignant hyperthermia
Neuroleptic malignant syndrome
Withdrawal
Up to 50% of adults over the age of 18 admit to regular alcohol consumption and up to 50% of these patients report withdrawal symptoms when abstinent. Signs and symptoms of acute withdrawal can begin to manifest 6-72 hours after the last ingestion and range in severity from mild, vague symptoms to florid delirium tremens. Treatment is aggressive benzodiazepine regimens to abate the symptoms, with a gradual taper while in the hospital.
“Wonky” Glands
Though rare, two endocrinologic conditions can cause fever in the postoperative period. Adrenal insufficiency and thyrotoxicosis can both occur due to disruption of the hypothalamic-pituitary-adrenal/thyroid axis by the inflammatory mediated response of surgery. Coupled with a patient being NPO prior to surgery, a patient may not be able to take their medications to keep these conditions at bay. Careful preoperative history will identify these patients prior to surgery and recommendations can be made on which medications can be taken the morning of surgery, or what medications can be given in perioperatively.
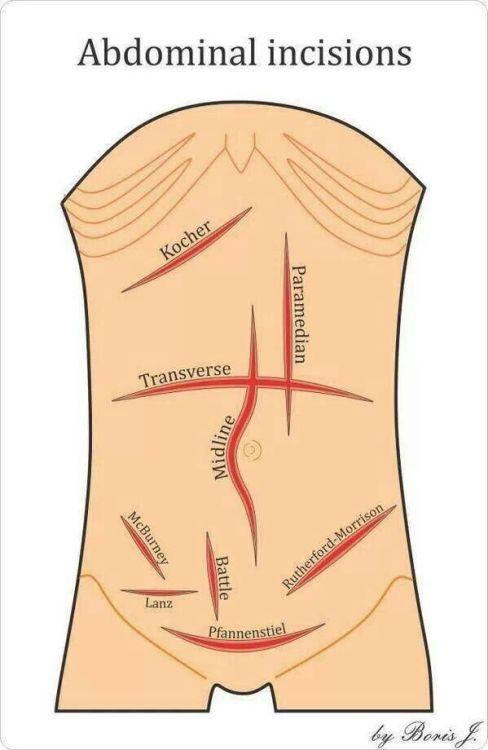
Definition – oblique incision in the right subcostal area starting 2-5cm below the xiphoid process, running parallel to the ribs, and extending to 2.5cm below the inferior costal margins
Clinical Significance – classic incision used for open cholecystectomy
Kocher Maneuver
Other Known Aliases – retroperitoneal exposure
Definition – maneuver to expose the retroperitoneal structure (pancreas, duodenum, vena cava)
Clinical Significance – this maneuver is used for resection of pancreatic head tumors or in trauma with retroperitoneal hemorrhage. The peritoneum is incised at the right edge of the duodenum and continued in a “C” shaped from superior to inferior. The duodenum and head of the pancreas is then reflected medially to the left to expose the retroperitoneal structures.
History –Named after Emil Theodor Kocher (1841-1917), a Swiss surgeon who obtained his medical doctorate from the University of Bern in 1865. He was arguably the most accomplished surgeon of his time and true pioneer in the field of surgery by promoting and advocating the use of aseptic technique, meticulous dissection with attention to minimal blood loss, and implementation of the scientific method in surgery. His “Text-Book of Operative Surgery” was the definitive guide to surgery in the early 1900s. He received the Nobel Prize in Physiology and Medicine in 1909…the first Swiss citizen and first surgeon to do so. The practice of modern surgery would certainly not be where it is today without the work of Dr. Kocher and his other notable eponyms are:
Kocher forceps – hemostatic tooth and groove forceps
Kocher’s point – entry point for intrventricular catheter to drain CSF from the cerebral ventricles
Kocher-Debre-Semelaigne Syndrome – hypothyroidism in infancy
Kocher collar incision – used in thyroid surgery
Kocher’s sign – eyelid phenomenon in hyperthyroidism
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Gautschi OP, Hildebrandt G. Emil Theodor Kocher (25/8/1841-27/7/1917)–A Swiss (neuro-)surgeon and Nobel Prize winner. British journal of neurosurgery. 2009; 23(3):234-6. [pubmed]
Clinical Significance – One of the more common self-retaining retractors used in surgery. They have a ratchet locking system and may also be available with jointed hinges. Primarily used for small to medium incision exposures.
History –Named after Franz Weitlaner (1872-1944), an Austrian physician who received his medical doctorate from Innsbruck Medical University in Austria at the age of 26 in 1898. He enjoyed a prolific career as as ship surgeon and house physician practicing in St. Poelten and Ottenthal in his homeland. In 1905, he published an article in the Vienna Clinical Review entitled “Ein Automatischer Wundspreizer” (An Automatic Wound-spreader), which would be the first description of his famous retractor. They were originally manufactured by Windler Instrument Makers in Berlin in 1912, but Weitlaner never patented his design or received any monetary gains from his invention, only the right to have the instrument named after him.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Other Known Aliases – Cotard delusion, Walking Corpse Syndrome
Definition – Rare mental illness in which a person feels they are dead, do not exist, parts of them are decaying or rotting, or they have lost internal organs, blood, or extremities.
Clinical Significance – The pathophysiology is not well understood and the two thoughts are that it is due to lesions or atrophy in the parietal and/or frontal lobes, or due to neural misfiring in the fusiform gyrus that is responsible for facial recognition.
The core concept of Cotard’s syndrome is a delusion of negation and classically progresses through three stages:
Germination Stage – symptoms of psychotic depression and hypochondria
Blooming Stage – full development of the syndrome and the appearance of the delusions of negation
Chronic Stage – severe delusions with chronic depressive symptoms
It is most common in patients with underlying schizophrenia and psychosis and patients often withdraw from society and the outside world. Partly because of the delusions and partly due to personal neglect of appearance and hygiene.There is no DSM-V diagnosis for Cotard’s syndrome, so it falls under the category of somatic delusions.
History –Named after Jules Cotard (1840-1889), a Parisian neurologist, psychiatrist, and surgeon who received his medical doctorate in 1868 from the University of Paris and worked at the Hospice de la Salpétriére under Jean Martin Charcot. In June 1880, he read a report on “Du délire hypochondriaque dans une forme grave de la mélancolie anxieuse” where he described a case of a 43yo woman who believed she had no brain, nerves, or entrails and that she did not need food, for she was eternal and would live forever. Emil Régis was the first to coin the eponym in 1893. In 1889, his daughter contracted diptheria and for 15 days he refused to leave her bedside until she recovered. Unfortunately, he contracted the same illness and succumbed to disease later that year.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
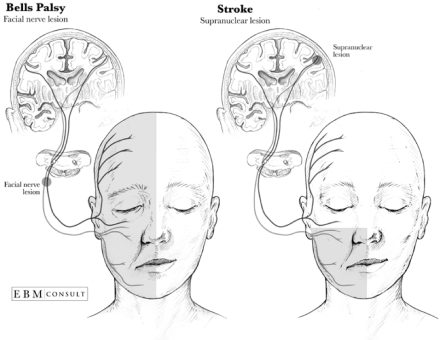
Other Known Aliases – facial nerve palsy, cranial nerve VII palsy
Definition – paralysis of cranial nerve VII that can can effect both motor and sensory function
Clinical Significance – This condition affects up to 20 patients per 100,000 population with no gender, race, or geographic predilection. It is the most common cause of unilateral acute peripheral nerve palsies. Although benign in clinical course, providers must pay close attention to differentiate between Bell’s palsy and a supranuclear lesion (stroke). The most significant clinical difference between these two condition is the ability to raise the eyebrow and wrinkle the forehead.
History –Named after Sir Charles Bell (1774-1842), a Scottish surgeon, anatomist, physiologist, neurologist, and noted philosophical theologian who received his medical doctorate at the University of Edinburgh in 1799. While still a student, he illustrated and published an extraordinary textbook entitled “A System of Dissection Explaining the Anatomy of the Human Body” After graduation, he was admitted and enrolled at The Royal College of Surgeons where he proved himself to be as skilled in surgery as in anatomy. He further published two subsequent volumes of “Anatomy of the Human Body”, with his brother John (also a skilled anatomist and surgeon). He was such a prolific teacher and professor that the faculty at the University of Edinburgh blocked his advancement and he was forced to move to London where he first opened a private school of anatomy and then took over the Great Windmill Street School of Anatomy (founded by William and John Hunter). In 1811, he published “An Idea of a New Anatomy of the Brain” considered to be the quintessential textbook of neurology. In 1821, he published a paper entitled ” On The Nerves: Giving an Account of some Experiments on Their Structure and Functions, which lead to a new arrangement of the systems” where he described the trajectory of the facial nerve and the unilateral facial paralysis that could result. This paper is still considered one of the classics of neurology and led to the disease bearing his name. In 1824, he became the first professor of anatomy and surgery of the College of Surgeons in London and was knighted by King William IV due to his contributions of the advancement of medicine.
References
Firkin BG and Whitwirth JA. Dictionary of Medical Eponyms. 2nd ed. New York, NY; Parthenon Publishing Group. 1996.
Bartolucci S, Forbis P. Stedman’s Medical Eponyms. 2nd ed. Baltimore, MD; LWW. 2005.
Yee AJ, Pfiffner P. (2012). Medical Eponyms (Version 1.4.2) [Mobile Application Software]. Retrieved http://itunes.apple.com.
Bell C, Shaw A. Reprint of the “Idea of a New Anatomy of the Brain,” with Letters, &c. Journal of anatomy and physiology. 1868; 3(Pt 1):147-82. [pubmed]
What is the popular scoring system for determining a patient’s need for anticoagulation to prevent stroke in atrial fibrillation?
If you do start anticoagulation, what are some scoring systems to determine a patient’s risk for bleeding while on anticoagulation?
Answers
CHA2DS2-VASc is the most utilized scoring systems for determining anticoagulant selection to prevent stroke in patients with atrial fibrillation. The components are as follows
CHF (+1)
HTN (+1)
Age
< 65yr (0)
65-74 (+1)
≥ 75 (+2)
DM (+1)
Stroke/TIA (+2)
Vascular disease (+1)
Sex category (+1 for female)
Interpretation:
0 points (low risk) – consider antiplatelet only
1 point (low/moderate risk) – antiplatelet or anticoagulation
≥ 2 points (moderate/high risk) – anticoagulation
If you are deciding on whether to start anticoagulation or not, you should determine the bleeding risk of your patient on anticoagulation. There are three scoring systems that can help with this:
ATRIA
Anemia (Hgb < 13g/dL in male and < 12g/dL in female)(+3)
Severe renal disease (GFR < 30mL/min or dialysis)(+3)
Age ≥ 75yr (+2)
History of bleeding (+1)
HTN (+1)
Interpretation:
< 4 points – low risk
4 points – intermediate risk
> 4 points – high risk
HASBLED
HTN (uncontrolled or > 160mmHg)(+1)
Renal disease (+1)
Liver disease (+1)
Stroke history (+1)
Prior bleeding history (+1)
Labile INR (+1)
Age ≥ 65 (+1)
Medications (+1)
Alcohol (+1)
Interpretation:
0 points – low risk
1-3 points – moderate risk
≥ 4 points – high risk
HEMORR2HAGES
Hepatic or renal disease (+1)
Ethanol use (+1)
Malignancy (+1)
Older than 75 (+1)
Reduced platelet count/function (+1)
Rebleeding risk (+2)
HTN (+1)
Anemia (+1)
Genetics (+1)
Excessive fall risk (+1)
Stroke history (+1)
Interpretation:
0-1 points – low risk
2-3 points – intermediate risk
≥ 4 points – high risk
References
Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010; 137(2):263-72. [pubmed]
Fang MC, Go AS, Chang Y, et al. A new risk scheme to predict warfarin-associated hemorrhage: The ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation) Study. Journal of the American College of Cardiology. 2011; 58(4):395-401. [pubmed]
Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest. 2010; 138(5):1093-100. [pubmed]
Gage BF, Yan Y, Milligan PE, et al. Clinical classification schemes for predicting hemorrhage: results from the National Registry of Atrial Fibrillation (NRAF). American heart journal. 2006; 151(3):713-9. [pubmed]
Ruff T. Which risk score best predicts bleeding with warfarin in atrial fibrillation?. Online – American College of Cardiology. Sept. 26, 2011 [link]