This week’s PAINE Pearl revolves around hyperlipidemia management.
- What are the indications for high-intensity statin therapy?
- What are the drugs and dosing for high-intensity statin therapy?


This week’s PAINE Pearl revolves around hyperlipidemia management.
Epidemiology
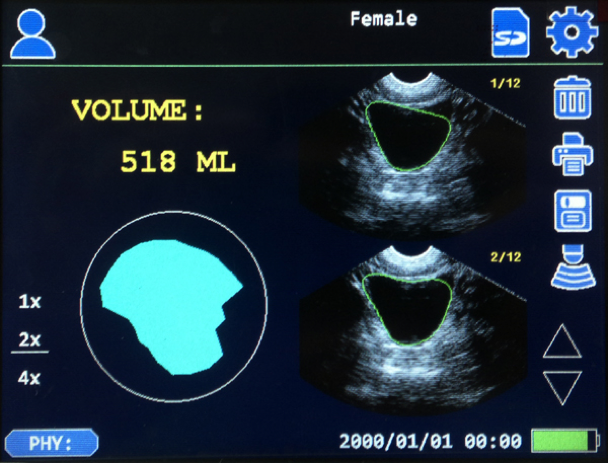
The prostate begins to enlarge in the 4th decade of life with a significant jump in the 6th decade of life. Mean prostate weight in normal men < 30yo is around 20g and steadily increases after this. Volume of the prostate also steadily increases after the 4th decade with symptoms typically starting to manifest once it reaches 30cc3.

Up-To-Date. 2016
Risk Factors
Pathogenesis of BPH
The main areas of the prostate that contribute to BPH are the periurethral (transitional zone) of the prostate and the hyperplastic nodules that develop are primarily comprised of stromal cells. The specific pathogenesis of BPH is still not completely understood and only 2 variables that have been identified as essential for BPH development: age and functioning Leydig Cells of the testes. Androgens, estrogens, inflammation, genetics, and stromal growth factors have all been studied and have variable results.

De Marzo. 2007.
Clinical Manifestations of BPH
The signs of symptoms of BPH can be broken down into 3 main categories:
Differential Diagnosis of BPH Symptoms
International Prostate Symptom Score
The original AUA score was developed in 1992 and is used to assess the severity of symptoms of BPH, BUT NOT FOR DIFFERENTIAL DIAGNOSIS. This is a seven-part questionnaire that evaluates symptoms on a 0-5 scale and then calculates the symptoms as mild, moderate, or severe. An eight question was added to evaluate quality of life.

International Prostate Symptom Score
Work-Up



Management
BPH can be managed by PCP if the patient has mild symptoms (low IPSS ≤ 7) and no complications.
Indications for urology referral are:
Treatment


Complications of Surgery
Cottage Physician

References

22yo male presents to emergency department with a 2-hour history of increasingly intense testicular pain. He reports being sexually active with multiple partners and intermittent condom use. He is a very active person and completed a triathlon the day before presentation. He denies dysuria, urethral discharge, or flank pain, but did have an episode of vomiting prior to arrival. He is in visible distress and can not seem to get comfortable. Evaluation of the scrotum reveals a tender, swollen left testicle.




References
22yo male presents to emergency department with a 2-hour history of increasingly intense testicular pain. He reports being sexually active with multiple partners and intermittent condom use. He is a very active person and completed a triathlon the day before presentation. He denies dysuria, urethral discharge, or flank pain, but did have an episode of vomiting prior to arrival. He is in visible distress and can not seem to get comfortable. Evaluation of the scrotum reveals a tender, swollen left testicle.
This patient is ready for extubation. Everyone has their own magic numbers they want to see on the vent before they think about extubating a patient, but mine are:
These are basic principles and there are many variables that go into deciding to extubate a patient. LITFL does a great review here and goes through a very systematic approach.
Once this is all good, then you can perform a few bedside tests or measurements that can help predict success of extubation.

Prediction of Successful Extubation. The ICU Book.
Great post from Intensive Blog on “The Art and Science of Extubation”
References

Definition and Cellular Physiology of Shock
The definition of shock is a clinical state of cellular and tissue hypoxia/perfusion due to:
It basically comes down to the ratio between oxygen delivery (DO2) and oxygen extraction (VO2).
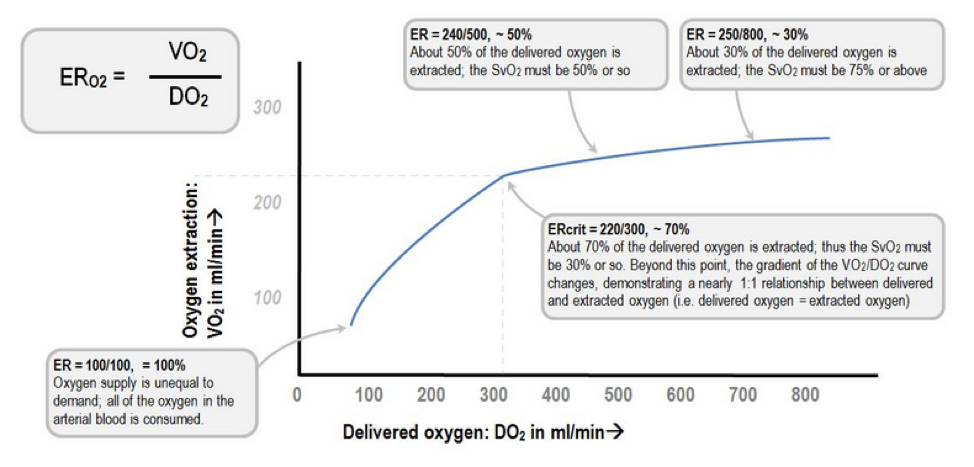
Extraction Ratio (ER)

Deranged Physiology

At the cellular level, shock hypoxemia causes cell membrane dysfunction leading to intracellular edema and leakage, as well inability to regulate cellular pH. This causes progressive acidemia, which in turn, have severe systemic effects on multiple organ systems.

Kherallah M.
Pathophysiology of Shock
BP = (HR x SV) x SVR
Factors effecting HR:
Factors effecting SV:
Factors effecting SVR:
Signs and Symptoms of Shock
As perfusion decreases and hypoxia starts, the body begins to compensate and the signs and symptoms of shock are generally a result of this compensation.

Classifications and Causes of Shock

UpToDate
How to Diagnose Shock
Laboratory studies should be performed very early in the screening process for a patient with suspected shock as it will help you determine the degree of end organ perfusion. These include:
There has been a tremendous amount of advancement in the diagnosis and management of patients in acute shock. For years, the pulmonary artery catheter was the gold standard for critically ill patients admitted to the ICU. It allowed for serial “measurements” of almost all the hemodynamic parameters you needed (PACWP, CO, CI, SVR, PAP, SvO2), but it was not without serious complications. It still has it’s place for certain disease management, but it is no longer indicated for diagnosing the different types of shock. I bring this up only because these parameters can be helpful when learning the different shock states as you can focus on 3 main variables: PACWP, CO/CI, and SVR.

Point-of-Care ultrasonography (POCUS) has really become the test of choice for an undifferentiated shock patient, as it provides fast, vital information of the different causes of shock and allows for rapid rule-out of life-threatening conditions. There are several different types of POCUS algorithms used depending on the history and clinical context of the patient.

Rapid Ultrasound in Shock (RUSH) is used for undifferentiated patients. Scott Weingart does a great podcast on this technique here and Sinae EM Ultrasound did a step-by-step review here.

Another approach to undifferentiated shock is the Abdominal and Cardiac Evaluation with Sonography (ACES) protocol. It is used primarily in the UK and a good review can be found here.
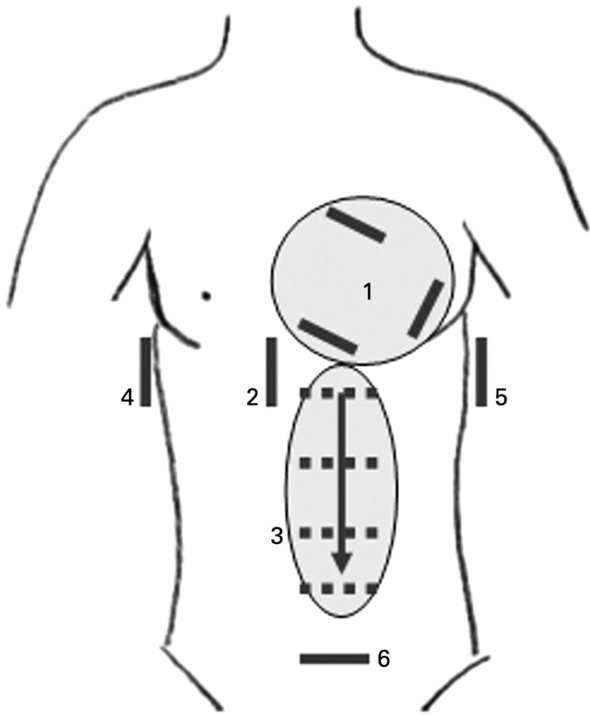
ACES Exam
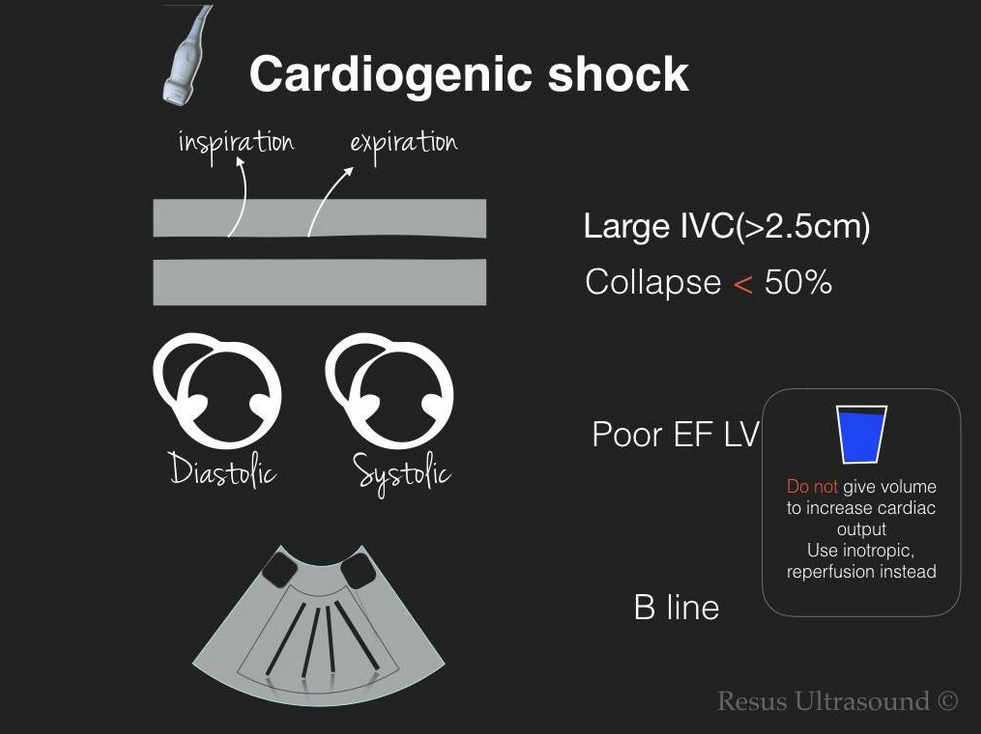
Focus Assessed Transthoracic Echo (FATE) is a more detailed look at the heart to identify specific cardiac abnormalities.

If you have a trauma patient, you would use the Focused Assessment with Sonography for Trauma (FAST) exam to rapidly identify traumatic causes for hemorrhage and need for operative intervention.

FAST Exam
Really good paper in Critical Care that reviews echocardiography in shock management
http://ccforum.biomedcentral.com/articles/10.1186/s13054-016-1401-7
Management of Shock
Once you diagnose a patient with a specific type of shock, the management is pretty straight forward. If the patient is in hypovolemic, distributive, or obstructive shock, IV fluids should be used to improve perfusion and hemodynamics. The amount depends on the conditions, but usually starting with 1-2L of crystalloids is a good bet and then you can re-evaluate and repeat your ultrasound to look at the effects. If you have a trauma patient, then blood products should be started early on in the course until definitive control can be performed.
If adequate fluid resuscitation has not improved the hemodynamics or clinical picture, then pharmacologic agents are needed to improve perfusion. These can be broken down into vasopressors (increase vasomotor tone) and inotropes (increase contractility).
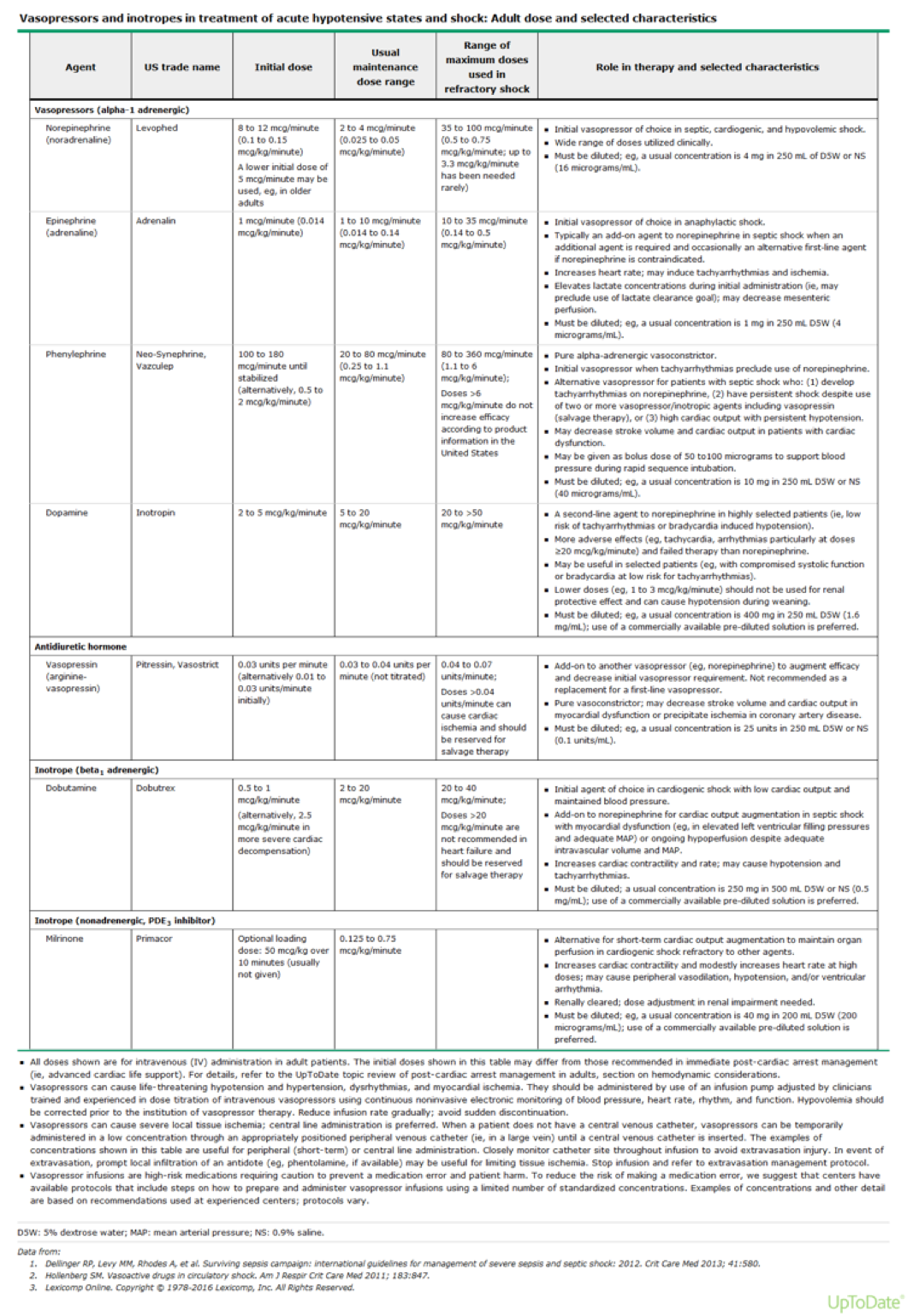
UpToDate



References
You are rounding on a ICU patient who has been on the ventilator for the past 4 days due to respiratory failure from community acquired pneumonia. She has been gradually weaned down to the following settings:
Pressure Support Mode
PEEP – 6 cmH2O
Pressure Support – 8 cmH2O
Oxygen – 0.40
She is A&Ox3 and follows commands. Vital signs show BP – 122/72 mmHg, HR – 78, RR – 15, O2 – 100%, Temp – 99.8.
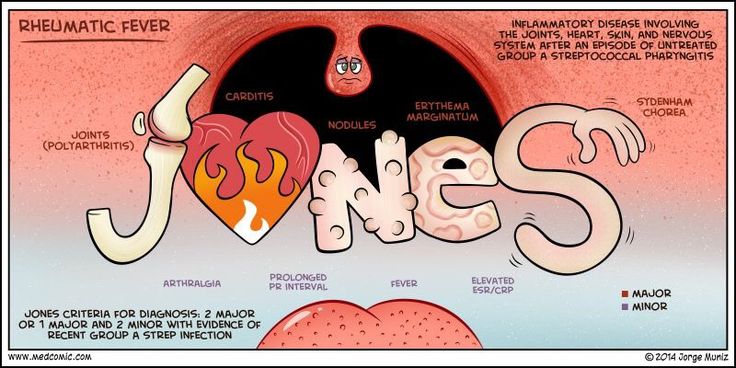
Diagnosis: Acute rheumatic fever
Criteria: Jones criteria
Acute rheumatic fever (ARF) is a sequella of symptoms that typically occur 2-4 weeks after an untreated bout of group A Streptoccocal (GAS) pharyngitis. Symptoms include arthritis, carditis, erythema marginatum, CNS symptoms, and subcutaneous nodules.
Jones criteria is constellation of symptoms of ARF and are subdivided into major and minor manifestations.
Major
Carditis
Arthritis
CNS involvement
Subcutaneous nodules
Erythema marginatum
Minor
Arthralgia
Fever
Elevated acute phase reactants
Prolonged PR interval
The diagnosis of ARF is made using the Jones criteria and is positive if the patient has evidence of a preceding GAS infection and:
or

This is a lecture I gave to a group of biomedical science students on how to write a personal statement for graduate professional programs. It is directed towards medical professions (PA, MD, DO, DMD, etc.), but the basic tenets are the same. By following a few basic rules and sprinkling in your unique experiences, your narrative will win over the selection committee.
You are participating in a medical mission in South America and are seeing a 11yo boy who is brought in by his mother. He has been complaining of joint pain and fever for the past 2 weeks. She tells you that it seems to “move” from joint to joint over this time and nothing seems to help. She does report that he has seemed to be sick for 4-6 weeks with various “cold” symptoms, but they didn’t seem too severe. On examination, he has temperature of 101.2oF and the below rash.

What should be your concern and what criteria can help make the diagnosis?